
Open Access, Volume 10
Role of CD64 ratio determination in pneumococcal versus Legionella community-acquired pneumonia
Sergio Venturini1; Ingrid Reffo2*; Manuela Avolio3; Giancarlo Basaglia3; Giovanni Del Fabro1; Astrid Callegari1; Igor Bramuzzo1; Maurizio Tonizzo4; Silvia Grazioli4; Elena Garlatti4; Paolo Doretto5; Chiara Pratesi5; Gabriella Nadalin2; Massimo Crapis1
1Department of Infectious Diseases, ASFO Santa Maria degli Angeli Hospital of Pordenone, Italy.
1Department of Anesthesiology, ASFO Santa Maria dei Battuti Hospital of San Vito al Tagliamento (PN), Italy.
1Department of Microbiology, ASFO Santa Maria degli Angeli Hospital of Pordenone, Italy.
1Department of Internal Medicine, ASFO Santa Maria degli Angeli Hospital of Pordenone, Italy.
1Department of Laboratory, ASFO Santa Maria degli Angeli Hospital of Pordenone, Italy.
Ingrid Reffo
Department of Anaesthesiology, ASFO Santa Maria dei Battuti Hospital of San Vito al Tagliamento, via
Savorgnano 2, 33078 S. Vito al Tagliamento (PN), Italy.
Tel: +39-0434-841305;
Email: ingrid.reffo@asfo.sanita.fvg.it
Received : Mar 18, 2024,
Accepted : May 01, 2024
Published : May 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Community-Acquired Pneumonia (CAP) poses a major clinical challenge, with atypical pathogens contributing to a notable percentage of cases. Early identification of Legionella is essential for prompt therapeutic intervention. The Urinary Antigen Test (UAT), which targets Legionella pneumophila serogroup 1, stands out as a widely used and advantageous method for Legionella diagnosis due to its simplicity and ability to detect the pathogen even after antibiotic therapy.
Traditional biomarkers lack specificity in distinguishing between viral and bacterial infections. The neutrophil cluster of differentiation 64 (nCD64), which is recognized as a sensitive marker for bacterial sepsis, holds promise in CAP diagnosis and severity assessment.
This study delved into variations in nCD64 values within Legionella and Streptococcus pneumoniae subgroups, offering insights into their diagnostic potential. From January 2021 to November 2023, we included 121 CAP patients with positive UAT for Legionella (LP) or Streptococcus pneumoniae (SP). LP patients exhibited significantly higher nCD64 levels, indicating species-specific activation. Despite certain limitations, this study underscores the diagnostic significance of nCD64, especially in Legionella infections. Future research should explore its role alongside Legionella UAT, potentially influencing antibiotic stewardship in CAP management.
Keywords: Legionella spp; Urinary antigens test; UAT; Flow cytometry; CD64; Community-acquired pneumonia; Atypical pathogens.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Reffo I (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Venturini S, Reffo I, Avolio M, Basaglia G, Del Fabro G, Callegari A, Bramuzzo I, et al. Role of CD64 ratio determination in pneumococcal versus Legionella community-acquired pneumonia. Open J Clin Med Case Rep. 2024; 2235.
Introduction
Community-Acquired Pneumonia (CAP) is a prominent cause of mortality and morbidity with important clinical impact across the globe. Bacteria of the genus Legionella sp are important causative agents comprising over 50 species and 64 serogroups. Legionella pneumophila species cause approximately 90% of Legionella infections,Legionnaires’ disease, and nosocomial pneumonia [1,2]. Serogroup 1 of Legionella pneumophila is considered responsible for most reported cases of Legionella infections.Among the typical bacteria, Streptococcus pneumoniae is the most common cause of CAP.
The Urinary Antigen Test (UAT) is widely used for the microbiological diagnosis of Legionella and Streptococcus pneumoniae infections, while culture remains the diagnostic gold standard despite the limitations imposed by the time required for identification and the potential interference of prior antibiotic therapy.
Several established biomarkers (e.g. C-Reactive Protein (CRP), leukocyte count, and procalcitonin) are employed to assist emergency physicians in narrowing down possible diagnoses. However, many studies have demonstrated that they are not able to differentiate between bacterial infections, especially for some types of pathogens [3,4].
In the absence of specific biomarkers, various non-specific laboratory abnormalities are associated with Legionella CAP. These abnormalities include otherwise unexplained hyponatremia, hypophosphatemia, mildly elevated serum transaminases, elevated creatine phosphokinase, markedly elevated C-reactive protein, or microscopic hematuria [5,6]. In a short case series [7], all 14 hospitalized patients with Legionella CAP exhibited significantly elevated (twelve times the normal value) serum ferritin levels (range 396-5990 ng/mL). In another study, Higa et al. [8] demonstrated that serum levels of IFN-gamma (Th1 cytokines) were elevated in patients with Legionella pneumonia, while levels of IL-4 and IL-10 were not increased in these patients.
Recently, neutrophil cluster of differentiation 64 (nCD64), also referred as high-affinity immunoglobulin Fc- receptor I (FcγR1), has emerged as a sensitive and specific marker for the diagnosis of sepsis due to bacterial infections. It has also been shown to be effective in differentiating sepsis from non-septic conditions [9].
This new biomarker is upregulated after exposure to proinflammatory cytokines such as IFN-γ or bacterial cell wall components such as Lipopolysaccharide (LPS) and shows good sensitivity and specificity for the diagnosis of sepsis caused by bacterial infections [9,10]. In the context of CAP, nCD64 has been demonstrated to be useful for diagnosing bacterial infection and is associated with disease severity, but its exact role remains to be elucidated [11-13].
This new biomarker is upregulated after exposure to proinflammatory cytokines such as IFN-γ or bacterial cell wall components such as Lipopolysaccharide (LPS) and shows good sensitivity and specificity for the diagnosis of sepsis caused by bacterial infections [9,10]. In the context of CAP, nCD64 has been demonstrated to be useful for diagnosing bacterial infection and is associated with disease severity, but its exact role remains to be elucidated [11-13].
Patients and Methods
From January 2021 to November 2023, we conducted a retrospective investigation in our 800-bed Healthcare Authority, which includes Pordenone and San Vito al Tagliamento Hospitals in northeastern Italy.
We collected cases of confirmed CAP (diagnosed by the ED attending physician based on clinical, biological, and radiological findings) in which UAT was positive for either S. pneumoniae (SP group) or Legionella (LP group). Patients under the age of 18 were excluded. In our EDs, laboratory investigations for suspected respiratory infections and sepsis include the determination of nCD64 as part of the diagnostic work-up together with the leukocyte count, CRP, Procalcitonin (PCT), and UAT for S. pneumoniae and Legionella.
Consent to use personal clinical data was obtained from all participants in accordance with Italian law. Data were anonymized before storage and analysis. The study followed international and national regulations in accordance with the Declaration of Helsinki.
Urinary antigen testing: Urine samples were analyzed with STANDARD F Legionella and S. pneumoniae Ag FIA from SD Biosensor (Gyeonggi, South Korea). Fluorescence immunodiagnosis STANDARD F is a fluorescence immunodiagnostic system that can perform a variety of qualitative and quantitative diagnoses and provide accurate diagnostic results. Briefly, STANDARD F Legionella Ag FIA is based on immunofluorescence technology with STANDARD F Analyzer for detecting Legionella pneumophila serogroup 1 antigen. STANDARD F S. pneumoniae Ag FIA is a fluorescence immunoassay for qualitatively detecting S. pneumoniae Capsular Polysaccharide (CPS) antigen present in urine samples from patients with respiratory symptoms. The intensity of the fluorescent light generated on the membrane is scanned with the STANDARD F Analyzer from SD BIOSENSOR. The STANDARD F Analyzer can analyze the presence of the analyte in the clinical sample by processing the results using pre-programmed algorithms and displaying the test result on the screen.
Flow cytometry procedures: A rapid and simple whole blood flow cytometry assay was performed, combining the measurement of CD64 on neutrophils and CD169 on monocytes to differentiate between bacterial and viral causes of systemic infections, respectively. Briefly, a 10 μL EDTA whole blood sample was simultaneously lysed with 500 μL VersaFix lysis solution (Beckman Coulter, Hialeah, FL) and stained with 5 μl CD45KO and 10 μL IO Test Myeloid Activation antibody cocktail (Beckman Coulter) containing three markers: anti-CD169-PE (clone 7-239), anti-CD64-PB (clone 22), anti-HLA-DR-APC (clone Immu357). After a 15-minute incubation at room temperature in the dark, the samples were immediately analyzed on a Navios EX flow cytometer with three lasers and 10 colors (Beckman Coulter) according to a compensation-free protocol and evaluated using Kaluza software version 2.1.1 (Beckman Coulter). For data analysis, leukocytes were categorized as lymphocytes (low SSC CD64−), monocytes (intermediate SSC CD64+), and neutrophils (high SSC) based on side scatter (SSC) vs. cluster of differentiation (CD45) positive, CD64 expression. The Median Fluorescence Intensity (MFI) of CD64 expression on neutrophil to lymphocyte ratio (nCD64) and the MFI of CD169 expression on monocyte to lymphocyte ratio (CD169) were calculated. The threshold values were 3.51 for the CD169 ratio and 4.59 for nCD64 to discriminate between acute viral and bacterial infections.
Statistical analysis: The demographic and clinical characteristics of the sample were described using descriptive statistical techniques. Categorical data were presented as absolute values and percentages and analyzed using Pearson’s chi-square test. Quantitative variables were summarized by the following measures: Value, Range, Mean and Standard Deviation. Changes in quantitative variables were analyzed using the Mann-Whitney U-test.
Results
We obtained clinical and laboratory data from 121 patients with positive UAT and confirmed CAP. The UAT was positive for Legionella (LP) in 19 patients and for S. pneumoniae (SP) in 102 patients.
Table 1 shows the clinical characteristics and laboratory values. The patients in the LP group were significantly younger, while those with SP were older and showed a wider age range.
In all patients of the LP group, the nCD64 value was above the cut-off limit of 4.6, while a significant proportion of confirmed S. pneumoniae CAP (43%) displayed values below the positivity limit (Figure 1). The mean nCD64 value was significantly higher in the LP group than in the SP group (p-value<0,001), whereas PCT values were higher but not significant in LP patients compared to SP patients (p-value 0.04) (Figure 2).
The rate of ICU admission and the presence of a NEWS2 score greater than 7 upon presentation were not significantly different between the two groups.
Table 1: Characteristics of patients according to UAT positivity.
| Variables | LP group (n 19) | SP group (n 102) | p-value |
|---|---|---|---|
| Male (%) | 13 (68) | 48 (47) | 0,08c |
| Age, mean (range) | 63 (44-94) | 76 (30-95) | <0,001t |
| Viral co-infection (positive molecular nasal swab) (%) | 0 | 61 (50%) | <0,001 |
| NEWS2 admission >7 (%) | 6 (31,6) | 38 (37,2) | 0,09 |
| ICU admission (%) | 3 (15,8) | 19 (18,6) | 0,09c |
| PCT mcg/L, median (IQR) | 1,5 (2,18) | 1,39 (6,99) | 0,04u |
| CD64+ ratio, median (IQR) | 18,6 (10,05) | 5,05 (6,05) | <0,001u |
| CD64+ >4.6 (%) | 19 (100) | 58 (57) | <0,001 |
The bold p-value means that the associated analysis is statistically significant. t: t-test; u: Mann-Whitney U test; c: Pearson Chi square test.
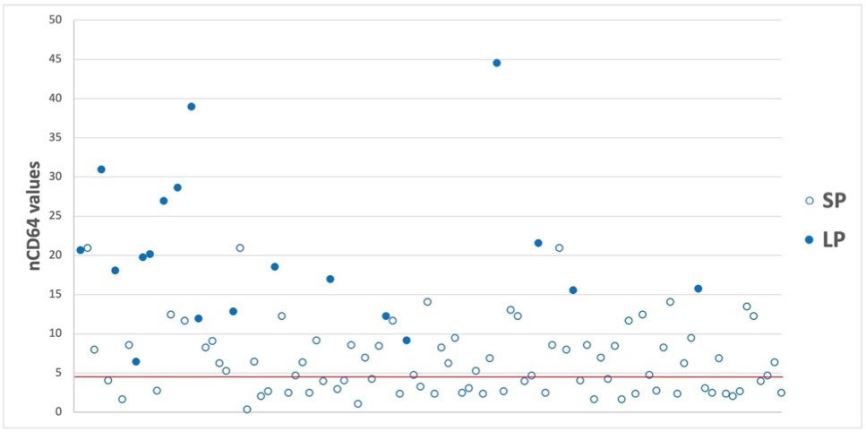
Figure 1: Distribution of CD64 values according to UATs.
Distribution of CD64 values. Empty dots = SP group, Solid dots = LP group. The red line represents nCD64 ratio 4.6, which is
the cut-off for test positivity.
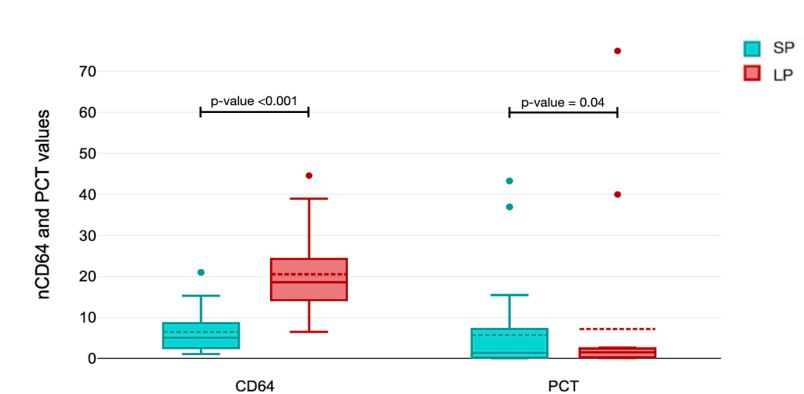
Figure 2: Box plot distribution of PCT and nCD64 values according to UATs.
Discussion
This study was conducted on patients who presented to the ED with signs of pulmonary infection and a positive Legionella or S. pneumoniae urinary antigen test.
One factor contributing to the differences in nCD64 values could be the range of delays in presenting to the emergency department after the onset of symptoms: it has been demonstrated that the up-and down-regulation of nCD64 after the infectious insult displays time-dependent kinetics [14]. In this scenario, although precise data on the diagnostic delay from the onset of symptoms are not available, it is important to emphasize that all these patients had to be treated in the emergency department due to their acute clinical condition. This indeed restricts the presence of confounding factors between the LP and SP groups.
Among the biomarkers used for the diagnosis of pneumonia, studies on Procalcitonin (PCT) have shown mixed results regarding possible differences between different pathogens. In the study conducted by Franzin, a quantitative assessment of procalcitonin in serum was performed in 140 patients with Legionella pneumonia [15]. Positive values (>0.5 ng/mL) were found in 73.9% of patients within the first week of illness. However, PCT levels have been reported to be significantly higher in patients with typical CAP than in atypical CAP: Horie and colleagues conducted an observational study in this regard at a single center involving patients with CAP. Thirty-one of the 102 patients included were diagnosed with streptococcal pneumonia [16]. The PCT values were significantly higher in individuals with pneumococcal pneumonia than those with other bacterial pneumonia (P<0.0001). In multivariable regression analysis, elevated PCT levels were significantly associated with pneumococcal etiology, and this association remained after adjustment for disease severity and demographic factors.
In a large study of 1337 patients, Kruger and colleagues also demonstrated that PCT values, along with CRP, and WBC were significantly higher in CAP due to classical bacterial pathogens than in atypical bacterial or viral pneumonia and increased with increasing disease severity [17]. Jereb and Kotar postulated that among patients with atypical pneumonia, the highest PCT concentration could be found in patients with legionellosis, as immune stimulation and cytokine production properties of Legionella are higher than those of other atypical microorganisms [18]. In our study, the difference in PCT between the two groups studied seems to be at the limit of significance and therefore not useful for differential diagnosis in a clinical setting, which is why PCT can be considered an unreliable diagnostic marker.
The impact of infections by various pathogens on the upregulation of nCD64 remains uncertain, as ex vivo research on this topic has yielded conflicting results. Some authors have reported that infections with Gram-negative bacilli induce higher expression of nCD64 compared to other bacterial infections, although there are no consistent findings in this regard [19].
Our case series seems to confirm previous studies that have shown that different microorganisms can trigger specific host inflammatory response pathways depending on their peculiar characteristics, leading to differential expression of the biomarker nCD64, which could serve diagnostic purposes [20].
Indeed, we observed an increased expression of nCD64 in the LP group compared to the SP group, suggesting a species-specific activation. In fact, during Legionella infection, a strong cytokine response is triggered as the first immune defense: in particular, Natural Killer (NK) cells produce high levels of IFN-γ in response to infection and subsequent alveolar macrophage apoptosis, which in turn triggers the overexpression of CD64 on the surface of neutrophils; this could account for the higher CD64 levels in LP patients [21-24]. Based on the data currently available, we cannot conclude with certainty whether hyperactivation of nCD64 in patients with negative UAT and high suspicion of Legionella infection warrants second-tier diagnostic testing (molecular or cultural), taking into account the patient’s risk factors [25]. Further studies are needed to explore this aspect in detail.
As the reports indicate, there seems to be a difference in nCD64 values related to the different microbiological isolations and not only to the severity of the disease, as indicated by some studies conducted in the ICU setting [26]. Also, in our case series, no significant difference in patients admitted to the ICU was found between the two groups in contrast to a significantly higher nCD64 level in the LP group.
Even if the prognostic role of CD64 is not addressed in our series, it becomes evident, in line with other studies, that this biomarker’s diagnostic significance is more compelling [11].
This study has several limitations. First, the sample size differs between the two groups. Second, we lack information on how many patients had previously received antibiotic therapy; these data are crucial as antibiotic therapy may negatively impact nCD64 [11,12]. Another limitation is the lack of an LP control group with negative UAT. Finally, there is a lack of information on the baseline conditions of the two patient groups.
Biomarker nCD64 should be included in the battery of nonspecific laboratory tests when Legionella is a diagnostic consideration for hospitalized patients with CAP. Highly nCD64 levels that are otherwise unexplained in hospitalized patients with CAP should suggest Legionnaires disease and should prompt specific Legionella diagnostic testing.
Future studies are needed to assess whether the combination of negative Legionella UAT and negative CD64 can definitively rule out the diagnosis of Legionella pneumonia. Alternatively, in patients with Community-Acquired Pneumonia (CAP), initiating antibiotic therapy with a spectrum directed against Legionella may be reasonable while waiting for the CD64 value. The clinical implication would be the potential discontinuation of antibiotic therapy for this microorganism in the event of a negative result, leading to significant savings in terms of antimicrobial stewardship.
Declarations
Author contributions: Conceptualization, S.V.; methodology, S.V., I.R. and M.A.; validation, C.P., L.P., and E.G.; formal analysis, S.V., I.R. and M.A.; investigation, G.D.F., I.B., A.C., C.P.; data curation, S.V., I.R and M.A.; writing — original draft preparation, S.V., I.R. and M.A.; writing — review and editing, M.C., S.G., and P.D.; supervision, G.B., M. T. and G.N.
Funding: No fund was used for this study.
Institutional review board statement: This study was guided by ethical standards and national and international laws. All participants signed informed consent form for data collection and publication.
Data availability statement: Data supporting the study results can be provided followed by request sent to the corresponding author’s e-mail.
Conflicts of interest: None.
References
- Palusińska-Szysz M, Cendrowska-Pinkosz M. Pathogenicity of the family Legionellaceae. Arch Immunol Ther Exp (Warsz). 2009; 57(4): 279-90.
- Phin N, Parry-Ford F, Harrison T, Stagg HR, Zhang N, et al.Epidemiology and clinical management of Legionnaires’ disease. Lancet Infect Dis. 2014; 14(10): 1011-21.
- Van der Meer V, Neven AK, van den Broek PJ, Assendelft WJ. Diagnostic value of C reactive protein in infections of the lower respiratory tract: Systematic review. BMJ. 2005; 331(7507): 26.
- Durán A, González A, Delgado L, Mosquera J, Valero N. Serum level of C-reactive protein is not a parameter to determine the difference between viral and atypical bacterial infections. J Med Virol. 2016; 88(2): 351-5.
- Cunha BA. Clinical diagnosis of legionnaires’ disease. Semin Respir Infect. 1998; 13: 116-27.
- Cunha BA. Hypophosphatemia: Diagnostic significance in legionnaires’ disease. Am J Med 2006; 119: e5-6.
- Cunha BA. Highly elevated serum ferritin levels as a diagnostic marker for Legionella pneumonia. Clin Infect Dis. 2008; 46(11): 1789-91.
- Higa F, Haroon A, Iha Y, Tasato D, Nakamura H, et al. Interleukin-17A in Legionella pneumonia: A retrospective study. Jpn J Infect Dis. 2015; 68(2): 148-50.
- Van der Meer W, Pickkers P, Scott CS, van der Hoeven JG, Gunnewiek JK. Hematological indices, inflammatory markers and neutrophil CD64 expression: Comparative trends during experimental human endotoxemia. J Endotoxin Res. 2007; 13(2): 94-100.
- Bourgoin P, Soliveres T, Barbaresi A, Loundou A, Belkacem IA, Arnoux I, et al. CD169 and CD64 could help differentiate bacterial from CoVID-19 or other viral infections in the Emergency Department. Cytometry A. 2021; 99(5): 435-445.
- Li S, Huang X, Chen Z, Zhong H, Peng Q, et al. Neutrophil CD64 expression as a biomarker in the early diagnosis of bacterial infection: a meta-analysis. Int J Infect Dis. 2013; 17(1): e12-23.
- Cid J, Aguinaco R, Sánchez R, García-Pardo G, Llorente A. Neutrophil CD64 expression as marker of bacterial infection: A systematic review and meta-analysis. J Infect. 2010; 60(5): 313-9.
- Burgos J, Los-Arcos I, Álvarez de la Sierra D, Falcó V, Aguiló A, et al. Determination of neutrophil CD64 expression as a prognostic biomarker in patients with community-acquired pneumonia. Eur J Clin Microbiol Infect Dis. 2016; 35(9): 1411-6.
- Thiriet C, Mahjoub K, Courte G, Labroca P, Cravoisy A, et al. Automated measurement of neutrophil CD64 expression for diagnosing sepsis in critically ill patients. Minerva Anestesiol. 2019; 85(9): 943-950.
- Franzin L, Cabodi D. Legionella pneumonia and serum procalcitonin. Curr Microbiol. 2005; 50(1): 43-6.
- Horie M, Ugajin M, Suzuki M, Noguchi S, Tanaka W, et al. Diagnostic and prognostic value of procalcitonin in communityacquired pneumonia. Am J Med Sci. 2012; 343(1): 30-5.
- Krüger S, Ewig S, Papassotiriou J, Kunde J, Marre R, et al. CAPNETZ Study Group. Inflammatory parameters predict etiologic patterns but do not allow for individual prediction of etiology in patients with CAP: results from the German competence network CAPNETZ. Respir Res. 2009; 10(1): 65.
- Jereb M, Kotar T. Usefulness of procalcitonin to differentiate typical from atypical community-acquired pneumonia. Wien Klin Wochenschr. 2006; 118(5-6): 170-4.
- Wang B, Tang R, Wu S, Liu M, Kanwal F, et al. Clinical Value of Neutrophil CD64 Index, PCT, and CRP in Acute Pancreatitis Complicated with Abdominal Infection. Diagnostics (Basel). 2022; 12(10): 2409.
- Menéndez R, Sahuquillo-Arce JM, Reyes S, Martínez R, Polverino E, et al. Cytokine activation patterns and biomarkers are influenced by microorganisms in community-acquired pneumonia. Chest. 2012; 141(6): 1537-1545.
- Liu X, Shin S. Viewing Legionella pneumophila Pathogenesis through an Immunological Lens. J Mol Biol. 2019; 431(21): 4321-4344. doi: 10.1016/j.jmb.2019.07.028.
- Chauhan D, Shames SR. Pathogenicity and Virulence of Legionella: Intracellular replication and host response. Virulence. 2021; 12(1): 1122-1144.
- Bourgoin P, Biéchelé G, Ait Belkacem I, Morange PE, Malergue F. Role of the interferons in CD64 and CD169 expressions in whole blood: Relevance in the balance between viral- or bacterial-oriented immune responses. Immun Inflamm Dis. 2020; 8(1): 106-123.
- Copenhaver AM, Casson CN, Nguyen HT, Fung TC, Duda MM, et al. Alveolar macrophages and neutrophils are the primary reservoirs for Legionella pneumophila and mediate cytosolic surveillance of type IV secretion. Infect Immun. 2014; 82(10): 4325-36.
- Kutsuna S, Ohbe H, Kanda N, Matsui H, Yasunaga H. Epidemiological analysis of Legionella pneumonia in Japan: A national inpatient database study. J Epidemiol. 2023.
- Pham HM, Nguyen DLM, Duong MC, Phan XT, Tran LT, et al. Neutrophil CD64-a prognostic marker of sepsis in intensive care unit: A prospective cohort study. Front Med (Lausanne). 2023; 10: 1251221.
