
Open Access, Volume 10
Can endobronchial metastasis from uterine leiomyosarcoma be managed by sleeve lobectomy? A case report and systematic review
Christoph Bacri1*; Isabelle Serre2; Sanaa Kamel1; Youcef Lounes3; Pierre Alric1; Ludovic Canaud1; Kheira Hireche1
1Department of Thoracic and Vascular Surgery, Arnaud de Villeneuve Hospital, Montpellier, France.
2Department of Anatomical Pathology, Guy De Chauliac Hospital, Montpellier, France.
3Department of Vascular Surgery, Cardio-Vascular Institute, Paris South, Massy, France.
Christoph Bacri
Vascular and Thoracic Surgery Department, Villeneuve Hospital, 191 av Doyen Gaston Giraud
34090-Montpellier, France.
Email: c-bacri@chu-montpellier.fr
Received : Mar 15, 2024,
Accepted : Apr 26, 2024
Published : Apr 30, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Uterine Leiomyosarcoma (uLMS) is an exceptionally rare yet aggressive tumor, characterized by poor clinical outcomes. It exhibits a high potential for metastasis, even long after apparent remission. Surgical excision remains the cornerstone of treatment for localized uLMS and isolated metastatic cases.
Endobronchial Metastases (EBM) originating from uterine leiomyosarcoma represent an exceedingly infrequent neoplasm, occasionally manifesting as gross endobronchial extension without bronchial wall invasion. Left untreated, this condition can lead to dyspnea resulting from bronchial obstruction, hemoptysis, recurrent pulmonary infections, and ultimately, respiratory failure or fatality. Precise assessment of the bronchial tree through bronchoscopy allows for better surgical planning, especially when considering bronchial sleeve resection.
The preservation of the non-invaded lung parenchyma must be consistently taken into account, even in the presence of apparent complete bronchial obstruction. In this report, we present the case of a 67-year-old woman who underwent upper sleeve lobectomy for a bulky and obstructive EBM originating from uterine leiomyosarcoma, nine years after total hysterectomy for uterine leiomyoma. To date, only eleven other cases of uterine leiomyosarcoma metastasizing to the bronchus have been published.
Keywords: Endobronchial Metastasis; Uterine Leiomyosarcoma; Bronchoscopy; Sleeve Lobectomy.
Abbreviations: EBM: Endobronchial Metastasis; ER / PR: Estrogen / Progesteron Receptor; PET/CT FDG: Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography; SMA: Smooth Muscle Actin; Ulms: Uterine Leiomyosarcoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Bacri C (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Bacri C, Serre I, Kamel S, Lounes Y, Alric P, Canaud L, Hireche K. Can endobronchial metastasis from uterine leiomyosarcoma be managed by sleeve lobectomy? A case report and systematic review. Open J Clin Med Case Rep. 2024; 2234.
Introduction
Uterine Leiomyosarcoma (uLMS), a rare and aggressive tumor, represents approximately 1% of uterine malignancies [1]. The only potentially curative treatment for this condition, particularly in its early stages, is total abdominal hysterectomy with or without bilateral salpingo-oophorectomy. Distant metastases from uLMS account for 2.9% of cases [2], making it difficult to establish standard treatment protocols for recurrent cases. Systemic treatment and radiotherapy have not been proven effective in the adjuvant setting, leaving complete surgical resection as the best strategy for managing local relapse or metastasis of uLMS [3]. These metastases primarily occur through hematogenous dissemination rather than via the lymphatic duct, explaining why their sites are independent of pelvic and paraaortic nodal metastasis [4]. Unusual patterns of recurrence, such as involvement of the skin, bones, brain, spine, gastrointestinal tract, and thyroid, have been reported [5-7]. Although the lungs are the most commonly affected organs (67.7%) in metastatic cases, Endobronchial Metastases (EBM) are rare, and limited information exists regarding the management of uLMS metastasizing to the bronchus. In this report, we describe a unique case of gross EBM of uLMS and present the first reported instance of surgical management through sleeve lobectomy. The clinical significance of preoperative histological diagnosis, thorough exploration of the bronchial tree, and the use of parenchymal-sparing surgical techniques prompted this report. Furthermore, we provide a review of the pertinent literature concerning the diagnosis and therapeutic management of these specific metastatic entities.
Case Presentation
A 67-year-old Caucasian woman presented herself for pulmonary consultation due to a persistent cough and progressively worsening dyspnea. The patient had never smoked and had a significant medical history, including a total abdominal hysterectomy performed nine years ago. The pathology report from that time indicated that the fibroids were benign leiomyomas with a Ki-67 index of 1%. During the current examination, a physical assessment revealed diminished breath sounds in the right lung, while a chest X-ray revealed a thoracic mass on the right side accompanied by a pleural effusion. Subsequent computed tomography scans of the chest, abdomen, and pelvis revealed a 45 x 47 mm opacity in the right upper lobe, extending into the right main bronchus, leading to complete atelectasis of the middle and lower lobes (Figure 1). The lesion was lightly hypermetabolic with a SUV max of 4.1. Staging imaging, conducted using fluorodeoxyglucose Positron Emission Tomography (PET/CT FDG), did not detect any other metastatic sites.
At the initial bronchoscopy, a polypoid, highly vascularized mass was discovered, almost completely obstructing the right main bronchus, preventing exploration beyond the lesion. Unfortunately, the biopsies taken at that time were inconclusive (insufficient material, compromising further immunologic investigations) and had to be repeated in order to determine the histological type. During the second bronchoscopy, the mass could be crossed, providing a clear view of the intermedius truncus without any signs of tumor invasion. The carina was also found to be tumor-free (Figure 2). Based on the bronchoscopic impression, the tumor pedicle appeared to be located on the anterior bronchial wall between the carina and the upper bronchus. Subsequent biopsy samples revealed a bronchial localization of a differentiated smooth muscle tumor with intermediate Ki-67 proliferative activity (15%). As a result, it was not possible to definitively determine whether the tumor was benign or aggressive. However, considering the patient’s surgical history and the high expression of estrogen and progesterone receptors (ER and PR +++), the possibility of a bronchial metastasis from a uterine tumor was considered during the diagnostic process (Figure 3 for histopathology).
Preoperative pulmonary function testing was good enough to permits extensive resection if needed (FEV1 67%).
The interdisciplinary tumor board approved surgical resection without neoadjuvant therapy, followed by adjuvant aromatase inhibitor therapy (Letrozole 2.5 mg per day).
The patient underwent an upper sleeve lobectomy with bloc resection of the endobronchial extension of the tumor and systematic lymphadenectomy (sites 4-11) via a postero-lateral thoracotomy. No intraoperative section analyses were conducted during surgery because the sectioning of the bronchus was distant enough from the lesion to guarantee a clear margin. The postoperative course was uneventful, and the patient was discharged on the 7th post-operative day with satisfactory fibroscopic control of the bronchial anastomosis.
Upon final histology examination, the malignancy was identified as a 45 x 55 mm metastatic leiomyosarcoma in the upper lobe, with a continuous 35 x 25 mm endobronchial tumor extension from the right upper lobe to the right main bronchus. Microscopic analysis revealed a dense proliferation of spindle cells with weakly acidophilic cytoplasm, but no necrosis was observed. The neoplastic cells exhibited immunoreactivity for Smooth Muscle Actin (SMA), desmin, and caldesmon, but were negative for CD 10+. Ki67 proliferative activity reached 30%, and 100% of nuclei showed strong positivity for estrogen receptors (ER+++) and progesterone receptors (PR+++), supporting the histological diagnosis of EBM from uLMS. Bronchial margins were free of tumor (R0). Unfortunately, the histological results could not be compared with those of the primary tumor as the initial treatment was conducted in a different country, thereby impeding any direct comparison.
Four weeks after discharge, adjuvant anti-aromatase therapy was initiated and has been continued up to the present with no side effect to report. The patient is currently 26 months post-surgery and shows no evidence of recurrence for either malignancy. The patient is in good shape and remains active in daily life.
Systematic Review
A comprehensive literature search was conducted to identify published studies reporting the findings and therapeutic management of EBM from uLMS. Candidate studies published in English up to April 2023 were sought through computerized searches of PubMed, Web of Science, and Google Scholar databases. The search utilized keywords and MeSH terms were «EBM,» «pulmonary metastases,» «uLMS,» and «uterine malignancies.» Articles containing case reports of uLMS metastasizing to the lung were further analyzed to specifically identify cases involving metastasis to the bronchus.
Through this comprehensive research, only 11 other cases [8-15] of ULMS metastasizing to the bronchus were identified (Table 1). The mean age at diagnosis of metastasis was 52 years old, with 64% of cases showing localization on the main bronchus. The main symptoms observed were dyspnea and cough, followed by hemoptysis. Initial radiography revealed a large atelectasis with or without visible nodules in most patients. The mean interval between the diagnosis of the primary tumor and EBM was 41,2 months (range: 0-96 months), with two patients presenting synchronous metastasis at the time of diagnosis. Among the identified cases, five patients underwent surgical resection.
During follow-up, most patients experienced disease relapse, with a mean survival of 15,3 months (range: 0-66 months) after treatment. Notably, the current case is the first to emphasize the importance of performing a repeat bronchoscopic examination to accurately assess the entire bronchial tree, enabling the implementation of parenchymal sparing surgery through bronchial sleeve lobectomy.
Table 1: Matrix of the systematic review of 11 cases.
| CASE | Age (yrs) |
Localisation | Symptom of the metastase |
Radiological findings |
Interval* (Month) |
Neo-adjuvent therapy |
Type of treatment | Survival (month) |
|---|---|---|---|---|---|---|---|---|
| Gerst et al. [8] |
56 | Bronchus and small bowel |
abdominal pain | atelectasis | 96 | No | lobectomy | 24 --------- (relapse) |
| Erkal et al. [9] |
63 | Left main bronchus | Dyspnea, cough | Total atelectasis | 12 | No | RT (30Gy) | 7 --------- (relapse) |
| Flynn et al. [10] |
53 | Left main bronchus | Dyspnea, Wheezing | atelectasis | 48 | No | RT | 0 (died day 4) |
| Richman et al. [11] |
46 | Bronchus intermedius | Dyspnea, hemoptysis | Nodules, atelectasis, pleural effusion |
0 | No | 3 C of gemcitabine and docetaxel --------------------- + 7 C of ifosfamide. |
12 ------------------ (relapse) |
| Warren et al. [12] |
53 | Left main bronchus | Fever, cough | atelectasis, shift of mediastinum |
84 | No | Left pneumonectomy |
66 (free) |
| 40 | Right main bronchus | Dyspnea, chest pain | Nodule, atelectasis | 72 | No | Right inferior lobectomy |
22 ------------ (relapse) |
|
| 71 | Right main bronchus | Dyspnea, cough | atelectasis, shift of mediastinum |
84 | No | middle and lower lobectomy |
7 (free) | |
| 42 | Right main bronchus | Dyspnea, cough | atelectasis, shift of mediastinum |
18 | No | middle and lower lobectomy |
7 (free) | |
| Gosh et al. [13] |
38 | Left main bronchus | Cough, pain | atelectasis, shift of mediastinum |
4 | 6C Doxorubicin- Ifosfamide-Mesna ----------------------- +RT |
3C ----------------------- Gemcitabine |
? |
| Ono et al. [14] |
54 | Left upper bronchus | cough | Nodule and atelectasis |
0 | No | 1. doxorubicin --------------------- and ifosfamide--------------------- 2. pazopanib |
6 (relapse) |
| Giudice et al. [15] |
56 | Right upper and middle lobe |
hemoptysis | nodules | 0 | 2 (died) |
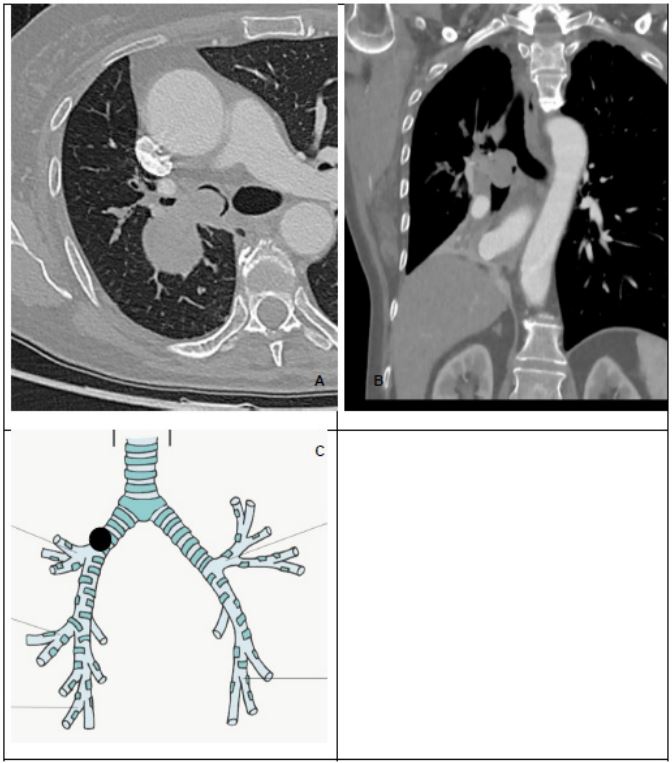
Figure 1: Imaging of the lesion: Thoracic transverse (A) and coronal (B) section of injected CT showing the obstruction of
the right bronchus. (C) is a schema of the bronchial tree showing the position of the lesion.

Figure 2: Endoscopic view of the mass obstructing the intermediate bronchus.
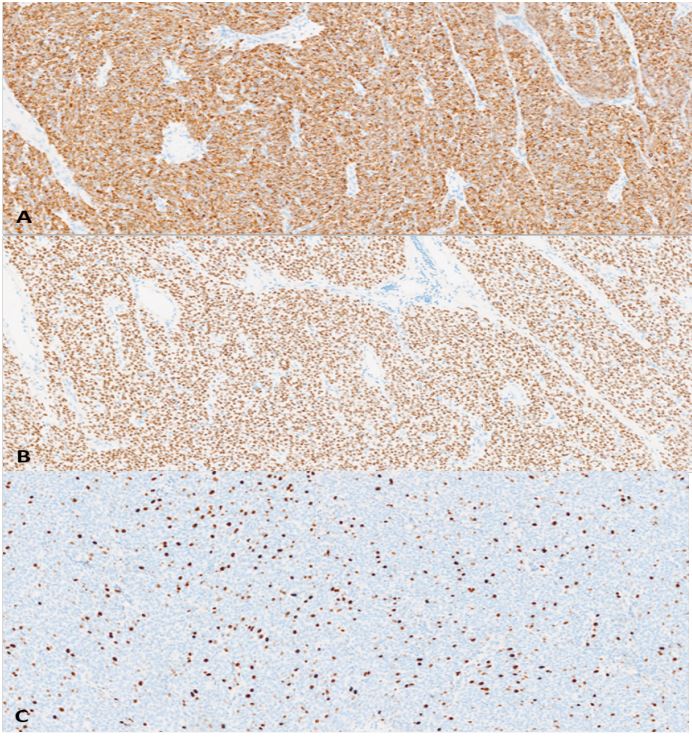
Figure 3: Histo-pathological analysis of the tumor: A - Immunohistochimic analysis looking for desmine: over represented
(+++), B - Research of hormonal receptors: Estrogen Receptors +++, C - Mitotic Index is high: Ki 67 up to 30% in the hotspots.
Discussion
Leiomyosarcomas are the fourth most common histological subtype of sarcomas, accounting for 11% of cases [16]. ULMS represents 30-40% of all uterine sarcomas and is associated with a poor prognosis, with a 5-year survival rate as low as 30%. Total abdominal hysterectomy with or without salpingo-oophorectomy is currently the only potentially curative treatment for localized uLMS. However, early-stage tumors (IA) tend to have a more favorable prognosis with 76.6% 5-year overall survival [17]. Post-operative recurrences are frequent, ranging from 50% to 70% [18]. Metastases often occur shortly after or even before the diagnosis of the primary tumor and can also develop after a long period without tumor activity [19]. The lungs are the most common site of hematogenous metastasis in uterine cancer, and surgical management of three or fewer pulmonary metastases has shown positive predictive value in gynecologic malignancies [20].
Clinically significant EBM from extrathoracic solid tumors are rare (2-4% in large series). The frequency estimates vary considerably depending on the study type and the definition of endobronchial metastasis. In a previous retrospective study that reviewed 1359 consecutive autopsies, metastatic involvement of a major airway was observed in only 2% of patients who died with solid tumors [21]. A clinical series of 174 cases by Marchionni et al. [22] showed that EBM from extrathoracic tumors occurred in 4% of all bronchoscopic biopsies performed for suspected malignancy. However, since bronchoscopy is not routinely performed in all patients with tumors, the incidence and frequency of EBM might be underestimated. The clinical presentation of EBM depends on the size and location of the tumor and can be difficult to differentiate from that of a primary pulmonary tumor. Consistent with our case, dyspnea, cough, and hemoptysis are the most common presenting symptoms. However, asymptomatic cases are not uncommon, accounting for 0 to 52% of cases [23]. Multiple pulmonary nodules and hilar-mediastinal lymphadenopathy are the most frequent findings in chest radiography, while peripheral masses and atelectasis are observed in approximately one-third of cases. However, these manifestations are not specific to EBM and can be seen in other diseases. The most common metastatic tumors causing symptomatic EBM include breast cancer, colon cancer, renal cell carcinoma, and melanoma [22].
Metastases of uLMS to the tracheobronchial tree are quite uncommon [4], and they are generally reported as individual case descriptions or very limited case series, as shown in Table 1. The present case is the first to undergo parenchymal sparing surgery with sleeve lobectomy. Sleeve resection is an established surgical procedure with better perioperative outcomes without sacrificing the oncological results compared with pneumonectomy in non– small cell lung cancer [24-26]. To our knowledge, only one case of sleeve lobectomy for endobronchial metastases of colorectal cancer has been previously reported [27]. We understand however, that due to the rarity of endobronchial metastasis, reports describing sleeve lobectomy for resecting this type of lesion are exceedingly rare, and so are the available outcome data.
Endobronchial exploration is an unavoidable diagnostic tool. Bronchoscopy must, therefore, meticulously and comprehensively examine the entire bronchial tree to ensure clearance of the bronchi. Additionally, multi-level biopsies of bronchial divisions upstream and downstream of the tumor should be performed to ensure the absence of tumor invasiveness, especially when planning a bronchial sleeve resection. It is important to note that the tumor may extend from the pulmonary parenchyma through the airway for a considerable distance without involving the bronchial wall. The bronchoscopy also allows for differentiation between bulky endobronchial tumor extension and true EBM involving the bronchial submucosa. Moreover, primary pulmonary leiomyosarcoma should also be considered in the differential diagnosis. In our case, bronchoscopy was performed twice, not only to establish a reliable diagnosis but also to thoroughly explore the bronchi. In a series of four patients, Warren et al. [28] reported a case of successful pneumonectomy for EBM of uLMS; however, the final anatomopathology of the specimen did not show evidence of bronchial wall involvement above the tumor site of origin. The authors rightly concluded that if the endobronchial growth pattern had been recognized, it might have been possible to save the left upper lobe. Understanding the developmental pattern of the tumor is crucial for a well-planned surgical procedure. In the present case, the developmental pattern was classified as type IV according to the classification proposed by Kiryu et al. [29]. This type corresponds to the extension of a parenchymal tumor through the airway without involvement of the bronchial wall. It is considered the most common condition. The other three types are: type I, direct metastasis to the bronchus; type II, bronchial invasion by a parenchymal lesion; and type III, bronchial invasion by mediastinal or hilar lymph node metastasis.
Leiomyosarcomas are smooth muscle tumors originating from embryonic mesenchyme cell lines. They are primarily detected during histopathological analysis of hysterectomy or myomectomy specimens, often presenting clinical symptoms similar to benign leiomyomas, which can lead to an inaccurate diagnosis [30]. The correct histological diagnosis can be challenging due to equivocal features resembling common benign uterine fibroids. Additionally, leiomyomas can undergo various degenerative changes, including malignant transformation. The incidence of sarcomatous transformation in benign uterine leiomyomas is only 0.1%-0.8% and is commonly observed in women in their 50s. Previous reports by Ogawa et al. [31] and Song et al. [32] have suggested that pulmonary benign metastasizing leiomyoma can also undergo malignant transformation, thereby supporting the hypothesis that these lesions represent metastatic low-grade leiomyosarcoma [33]. In the present case, despite the inability to compare the histology of the metastasis with that of the primary tumor, the patient’s clinical history, previous fibroid diagnosis, histological findings and the high Expression of Hormonal Receptors (ER, PR), prompted the tumor board to consider that the endobronchial and lung involvement were part of a metastatic process from uetrine leiomyosarcoma . This emphasizes the significance of contextualizing each individual case using clinical data, imaging studies, meticulous morphological examination, and appropriate immunohistochemical markers.
Radical surgery involving complete resection emerges as the most potent approach for locally metastatic uLMS. Anraku et al. [34] conducted a review of outcomes from 133 cases of surgical resection for pulmonary metastases of uterine malignancies, reporting a 38% 5-year survival rate (n=11) specifically for uLMS metastases. These findings, along with studies by Anderson et al. [20] and Levenback et al. [35], underscore the significant survival benefits associated with resecting solitary lung metastases.
Regarding EBM from uLMS, the available evidence is insufficient to support a specific treatment approach. Management should be personalized based on factors such as lesion sites, presence of other metastatic sites, and the patient’s overall condition. Various therapeutic strategies, including surgery, chemotherapy, bronchoscopic intervention, and radiation, should be considered. In the early stage with endobronchial localized metastases, because the bronchial wall is often uninvolved, surgical resection with preservation of uninvolved lung parenchyma is the preferred procedure. It is worth noting that even in cases of large endobronchial localized lesions, patients with sufficient pulmonary reserve should not be discouraged from surgical resection, even if pneumonectomy is required.
While adjuvant chemotherapy has not demonstrated significant benefits following complete surgical resection, the assessment of Estrogen and Progesterone Receptor (ER/PR) status in the metastases holds paramount importance. This information plays a crucial role in guiding additional treatment options, such as pregestational agents. Patients with positive ER/PR receptor status have demonstrated an 80% response rate and average survivals of up to 33 months [20].
When surgery is not a suitable option, bronchoscopy may be an important therapeutic option for endobronchial metastasis. Various techniques, including mechanical debulking, electrocautery, diathermy, argon plasma coagulation, laser resection, and cryoextraction, enable effective debulking therapy for endobronchial tumors. Interventional bronchoscopy plays a vital role in alleviating respiratory symptoms, improving the clinical status of patients, and providing opportunities for further palliative treatment [36]. In this case, the patient was deemed suitable for surgery, and given the inability to definitively determine whether the tumor was benign or aggressive, surgical resection was chosen for better anatomopathological determination. Furthermore, interventional treatment may not be as effective due to the nature of the EBM (Type 4: extension of a parenchymal tumor through the airway without involvement of the bronchial).
In palliative settings where surgery is not feasible, chemotherapy must be considered. However, its efficacy remains limited. Only one prospective randomized trial has shown an advantage for a docetaxel/ gemcitabine combination over gemcitabine alone in patients with metastatic soft tissue sarcomas [37]. Immunotherapy, while still under investigation, has yet to demonstrate significant efficacy. The addition of bevacizumab has not shown improved effects when combined with conventional chemotherapy [38]. On the other hand, Trabectedin has exhibited efficacy as a second-line therapy, with a four-month progressionfree survival in uterine sarcoma [39], and is approved for use after anthracycline failure. Radiotherapy may be considered after resection of an isolated single metastasis in the postoperative period to enhance local control or for palliative purposes in patients with localized unresectable disease.
Conclusion
In conclusion, we report a case of bulky EBM from uLMS successfully managed through bronchial sleeve lobectomy. This case not only underscores the significance of an aggressive surgical option while sparing parenchyma but also highlights... but also delves into the existing literature, shedding light on the different methods to improve diagnostic (use of bronchoscopy, immunohistological markers) and therapeutic. Given the protracted latency period associated with endobronchial metastasis, it is imperative for physicians to remain vigilant and consider the possibility of such metastases when encountering endobronchial lesions.
Declarations
Ethics approval and consent to participate: The review has been approved by local IRB and the patient of the case gave written consent for the use of pictures and data.
Consent for publication: The patient gave consent for publication of the pictures and data.
Availability of data and materials: No open access.
Competing interests: The authors have no conflicts of interest.
Funding: No funding was provided.
Authors’ contributions: C.B. and K.H. wrote the main manuscript text and I.S. prepared figures 1-3. All authors reviewed and approved the final version of the manuscript.
Acknowledgements: I am grateful to all of those with whom I have had the pleasure to work during this and other related projects.
References
- Echt G, Jepson J, Steel J, Langholz B, Luxton G, et al. Treatment of uterine sarcomas. Cancer. 1990; 66(1): 35-9.
- Seagle BLL, Sobecki-Rausch J, Strohl AE, Shilpi A, Grace A, et al. Prognosis and treatment of uterine leiomyosarcoma: A National Cancer Database study. Gynecol Oncol. 2017; 145(1): 61-70.
- Juhasz-Böss I, Gabriel L, Bohle RM, Horn LC, Solomayer EF, et al. Uterine Leiomyosarcoma. Oncol Res Treat. 2018; 41(11): 680-6.
- Rose PG, Piver MS, Tsukada Y, Lau T. Patterns of metastasis in uterine sarcoma. An autopsy study. Cancer. 1989; 63(5): 935-8.
- LiBrizzi CL, Vankara A, Meyer CF, Levin AS, Morris CD. Bone Metastases in Patients with Leiomyosarcoma: A Retrospective Analysis of Survival and Surgical Management. Sarcoma. 2022; 2022: 6806932.
- Contartese D, Bandiera S, Giavaresi G, Borsari V, Griffoni C, et al. Postoperative Survival and Clinical Outcomes for Uterine Leiomyosarcoma Spinal Bone Metastasis: A Case Series and Systematic Literature Review. Diagnostics (Basel). 2022; 13(1): 15.
- Bartosch C, Afonso M, Pires-Luís AS, Galaghar A, Guimarães M, et al. Distant Metastases in Uterine Leiomyosarcomas: The Wide Variety of Body Sites and Time Intervals to Metastatic Relapse. Int J Gynecol Pathol. 2017; 36(1): 31-41.
- Gerst PH, Levy J, Swaminathan K, Kshettry V, Albu E. Metastatic Leiomyosarcoma of the Uterus: Unusual Presentation of a Case with Late Endobronchial and Small Bowel Metastases. Gynecologic Oncology. 1993; 49(2): 271-5.
- Erkal HS, Oztürk AS, Kutluay L, Aydin D. Endobronchial metastases from a leiomyosarcoma of the uterus. Tuberk Toraks. 2008; 56(1): 92-5.
- Flynn KJ, Kim HS. Endobronchial Metastasis of Uterine Leiomyosarcoma. JAMA. 1978; 240(19): 2080.
- Richman M, Au J, Aoyama C, Kamangar N. Endobronchial Metastases of Gynecologic Leiomyosarcoma: A Case Report and Review of the Literature. Journal of Bronchology & Interventional Pulmonology. 2007; 14(2): 131.
- Warren WH, Bleck P, Kittle CF, Faber LP. Surgical management of pulmonary metastatic leiomyosarcoma with gross endobronchial extension. The Annals of Thoracic Surgery. 1990; 50(5): 739-42.
- Ghosh S, Kundu S, Pal A, Paul S. Rare Endobronchial metastasis from uterine leiomyosarcoma. Lung India. 2015; 32(2): 155.
- Ono M, Kobayashi S, Hanagama M, Ishida M, Sato H, et al. A case of metastatic endobronchial tumor from uterine leiomyosarcoma. Respiratory Medicine Case Reports. 2022; 40: 101747.
- Giudice JC, Komansky H, Gordon R. Endobronchial Metastasis of Uterine Leiomyosarcoma. JAMA. 1979; 241(16): 1684.
- Ducimetière F, Lurkin A, Ranchère-Vince D, Decouvelaere AV, Péoc’h M, et al. Incidence of sarcoma histotypes and molecular subtypes in a prospective epidemiological study with central pathology review and molecular testing. PLoS One. 2011; 6(8): e20294.
- Garg G, Shah JP, Kumar S, Bryant CS, Munkarah A, et al. Ovarian and uterine carcinosarcomas: A comparative analysis of prognostic variables and survival outcomes. Int J Gynecol Cancer. 2010; 20(5): 888-94.
- Abu-Rustum N, Yashar C, Arend R, Barber E, Bradley K, et al. Uterine Neoplasms, Version 1.2023, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2023; 21(2): 181-209.
- Carreiro A, Frias L, Miguel A, Rocha M, Carneiro V, et al. Unusual late lung metastasis from leiomyosarcoma of the uterus. Rev Port Pneumol. 2014; 20(4): 223-4.
- Anderson TM, McMahon JJ, Nwogu CE, Pombo MW, Urschel JD, et al. Pulmonary resection in metastatic uterine and cervical malignancies. Gynecol Oncol. 2001; 83(3): 472-6.
- Braman SS, Whitcomb ME. Endobronchial metastasis. Arch. Intern. Med. 1975; 135: 543-547.
- Marchioni A, Lasagni A, Busca A, Cavazza A, Agostini L, et al. Endobronchial metastasis: An epidemiologic and clinicopathologic study of 174 consecutive cases. Lung Cancer. 2014; 84(3): 222-8.
- Heitmiller RF, Marasco WJ, Hruban RH, Marsh BR. Endobronchial metastasis. The Journal of Thoracic and Cardiovascular Surgery. 1993; 106(3): 537-42.
- Pagès PB, Mordant P, Renaud S, Brouchet L, Thomas PA, et al. Sleeve lobectomy may provide better outcomes than pneumonectomy for non-small cell lung cancer. A decade in a nationwide study. J Thorac Cardiovasc Surg. 2017; 153(1): 184-195.e3.
- Deslauriers J, Grégoire J, Jacques LF, Piraux M, Guojin L, et al. Sleeve lobectomy versus pneumonectomy for lung cancer: A comparative analysis of survival and sites or recurrences. Ann Thorac Surg. 2004; 77(4): 1152-6.
- Berry MF, Worni M, Wang X, Harpole DH, D’Amico TA, et al. Sleeve lobectomy for non-small cell lung cancer with N1 nodal disease does not compromise survival. Ann Thorac Surg. 2014; 97(1): 230-5.
- Kim AW, Liptay MJ, Saclarides TJ, Warren WH. Endobronchial colorectal metastasis versus primary lung cancer: A tale of two sleeve right upper lobectomies. Interact Cardiovasc Thorac Surg. 2009; 9(2): 379-81.
- Warren WH, Bleck P, Kittle CF, Faber LP. Surgical management of pulmonary metastatic leiomyosarcoma with gross endobronchial extension. The Annals of Thoracic Surgery. 1990; 50(5): 739-42.
- Kiryu T, Hoshi H, Matsui E, Iwata H, Kokubo M, et al. Endotracheal/endobronchial metastases: Clinicopathologic study with special reference to developmental modes. Chest. 2001; 119(3): 768-75.
- Larson B, Silfverswärd C, Nilsson B, Pettersson F. Prognostic Factors in Uterine Leiomyosarcoma: A Clinical and Histopathological Study of 143 Cases the Radiumhemmet Series 1936-1981. Acta Oncologica. 1990; 29(2): 185-91.
- Ogawa M, Hara M, Ozawa Y, Moriyama S, Yano M, Shimizu S, et al. Benign metastasizing leiomyoma of the lung with malignant transformation mimicking mediastinal tumor. Clin Imaging. 2011; 35(5): 401-4.
- Song KS, Keum DY, Hwang IS. Malignant Transformation of Pulmonary Benign Metastasizing Leiomyoma. Korean J Thorac Cardiovasc Surg. 2017; 50(1): 59-63.
- Pacheco-Rodriguez G, Taveira-DaSilva AM, Moss J. Benign Metastasizing Leiomyoma. Clin Chest Med. 2016; 37(3): 589-95.
- Anraku M, Yokoi K, Nakagawa K, Fujisawa T, Nakajima J, et al. Pulmonary metastases from uterine malignancies: results of surgical resection in 133 patients. J Thorac Cardiovasc Surg. 2004; 127(4): 1107-12.
- Levenback C, Rubin SC, McCormack PM, Hoskins WJ, Atkinson EN, et al. Resection of pulmonary metastases from uterine sarcomas. Gynecol Oncol. 1992; 45(2): 202-5.
- Kim SJ, Kim J, Park JH, Lee AR, Lee JK, et al. Adjuvant treatment of proper endobronchial management in leiomyosarcoma. Tuberc Respir Dis (Seoul). 2013; 75(6): 250-5.
- Maki RG, Wathen JK, Patel SR, Priebat DA, Okuno SH, et al. Randomized phase II study of gemcitabine and docetaxel compared with gemcitabine alone in patients with metastatic soft tissue sarcomas: Results of sarcoma alliance for research through collaboration study 002 [corrected]. J Clin Oncol. 2007; 25(19): 2755-63.
- Hensley ML, Miller A, O’Malley DM, Mannel RS, Behbakht K, et al. Randomized phase III trial of gemcitabine plus docetaxel plus bevacizumab or placebo as first-line treatment for metastatic uterine leiomyosarcoma: an NRG Oncology/Gynecologic Oncology Group study. J Clin Oncol. 2015; 33(10): 1180-5.
- Hensley ML, Patel SR, von Mehren M, Ganjoo K, Jones RL, et al. Efficacy and safety of trabectedin or dacarbazine in patients with advanced uterine leiomyosarcoma after failure of anthracycline-based chemotherapy: Subgroup analysis of a phase 3, randomized clinical trial. Gynecol Oncol. 2017; 146(3): 531-7.
