
Open Access, Volume 10
A case of primary total knee arthroplasty revision using CORI system
Guido Bocchino1*; Alessandro Singlitico1 ; Vincenzo Campana2 ; Andrea Donato2 ; Paolo Satta2 ; Pierluigi Rinaldi2 ; Vincenzo De Santis1,2
1Department of Aging, Neurological, Orthopaedic and Head-Neck Sciences, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, Italy.
2Department of Orthopaedic Science Mater Olbia Hospital, Olbia, Italy.
Guido Bocchino
Department of Aging, Orthopedic and Rheumatological Sciences, Fondazione Policlinico Universitario
Agostino Gemelli IRCCS, Largo Agostino Gemelli 8, 00168 Rome, Italy.
Tel: +39 3343103404;
Email: guido.bocchino@hotmail.it
Received : Mar 29, 2024,
Accepted : Apr 22, 2024
Published : Apr 30, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Total Knee Arthroplasty (TKA) is a common surgical procedure used to treat end-stage osteoarthritis of the knee. The increasing adoption of computer-assisted and robotic assisted techniques in total joint arthroplasty has been found to enhance the accuracy of component placement. Short-term studies have indicated improved survival rates in unicompartmental knee arthroplasty with the use of robotic assistance. While robotic technology has proven beneficial in revising procedures like converting unicompartmental knee arthroplasty to TKA, there is limited information on its application in revising primary TKA. This case report details the use of robotic-assisted technology with CORI system in the revision of TKA. The incorporation of robotic assistance during TKA revision surgeries may contribute to better alignment of components and potentially increase the longevity of the prosthetic implant. However, further research is essential to explore the impact of robotic assistance on the overall survival rates and cost-effectiveness of revision TKA procedures.
Keywords: Revision; Knee; Arthroplasty; Robotic-assisted; Computer-assisted; Replacement.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Belli G (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Maietta PL, Belli G, Marini S, Bernardi E, Coppi F, Nasi M, Mattioli AV, et al. Healthy aging with sport: A case-report of an 81 years-old Italian man. Open J Clin Med Case Rep. 2024; 2231.
Introduction
The use of robotic arm assistance is increasingly popular in total joint arthroplasty [1]. Revision Total Knee Arthroplasty (rTKA) often addresses issues such as septic and aseptic loosening as well as periprosthetic fractures, especially among elderly individuals [2]. At our medical center, we employ the robotic arm-assisted CORI (Core of Real Intelligence) technology developed by Smith & Nephew. This advanced system utilizes image-free smart mapping, eliminating the necessity for pre-operative CT scans and minimizing image distortion from previous procedures. With this technology, surgeons can create patient-specific 3D joint models that accurately depict the anatomy profile and bony defects following component extraction. Furthermore, the system facilitates immediate intra-operative gap balancing and precise component placement. We opted for the CORI system over Mako (Stryker, Mahwah, NJ) due to the latter’s reliance on preoperative CT scans and off-label indications for primary joint replacement [3]. This case represents the inaugural use of the CORI system for robotic arm assistance in a revision Total Knee Arthroplasty (rTKA) procedure, necessitated by the failure of the primary TKA.
Case Report
In 2019, a 67-year-old woman underwent Total Knee Arthroplasty (TKA) with kinematic alignment technique at another medical facility due to right knee pain stemming from arthrosis, diagnosed through clinical examination and X-ray imaging (grade 3, Kellgren and Lawrence classification). Post-surgery, she faced challenges with intensive rehabilitation due to persistent anterior knee pain during both active and passive mobilization, resulting in a loss of 35 degrees of extension, swelling, and difficulty in walking. A Knee Society Score (KSS) was administered to her resulting in 20/100.
In 2021, she was diagnosed with patellofemoral malalignment and subsequently underwent patellofemoral arthroplasty to address patellar tracking issues. Unfortunately, she continued to experience discomfort postoperatively, impeding her physiotherapy efforts.
In September 2023, the patient presented to our institution with stiffness and severe knee pain, significantly limiting her daily activities. She reported a Visual Analogue Score (VAS) pain rating of 8/10 and was taking anti-inflammatory medication. Her knee Range of Motion (ROM) was restricted to 35°-85° due to mechanical blockage, indicating potential issues with the implant. To rule out a prosthetic joint infection, we conducted laboratory tests based on the 2018 MSIS criteria, including erythrocyte sedimentation rate, C-reactive protein, procalcitonin, blood count with formula and joint aspiration, all of which yielded negative results [4].
The CT scan showed no signs of loosening but there was evidence of an oversized femoral component in both mediolateral and anteroposterior planes leading to a patellofemoral overstuffing, according to methods of quantifying Patello-Femoral Joint (PFJ) overstuffing produced by Kemp et al. [5]. PFJ overstuffing has been shown to potentially affect the lever arm provided by the quadriceps mechanism in the knee stretching the patellar tendon, altering the contact forces between the implants, and thus leading to a decreased strength, limitated range of motion and giving pain. The anteroposterior PFJ size is given by a combination of parameters such as Anterior Patellar Displacement (APD), Anterior-Posterior Femur Diameter (APFD), Anterior Femoral Offset (AFO), and Posterior Femoral Offset (PFO) and consequently a modification of these parameters alters the patello-femoral tracking. In facts, restoring the anatomic dimensions of the PFJ is recommended, keeping the surgeon within a safe margin of error [6]. Furthermore, mediolateral oversizing is a factor considered to be predictable of poor results in TKA despite it is difficult to obtain optimal fit between the implant and bone [7].
After a lengthy discussion, we decided to proceed in right rTKA with CORI robotic assistance using Smith & Nephew revision knee system.
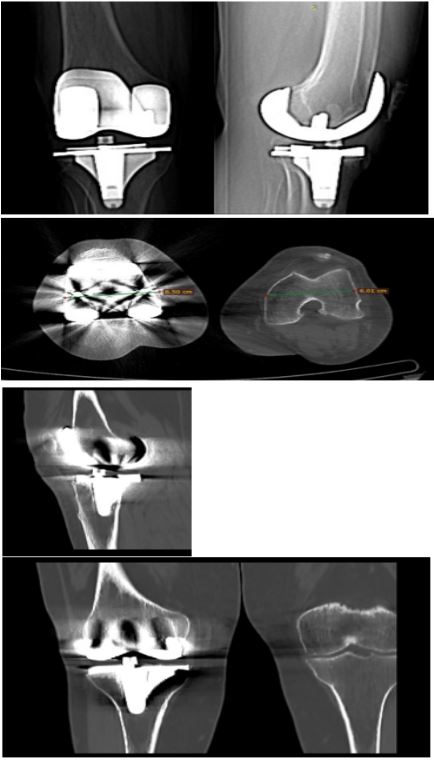
Figure 1 and 2: Pre-operative implants XR and CT scan.

Figure 3: Intra-operative mapping directly on the current implants.
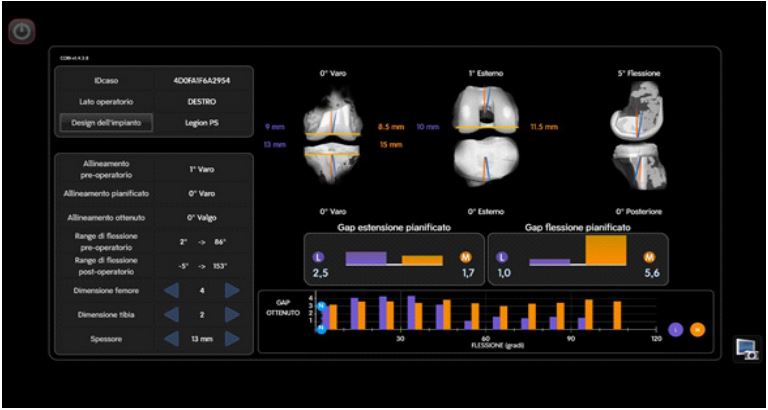
Figure 4: Post-operative mapping directly on the current implants.
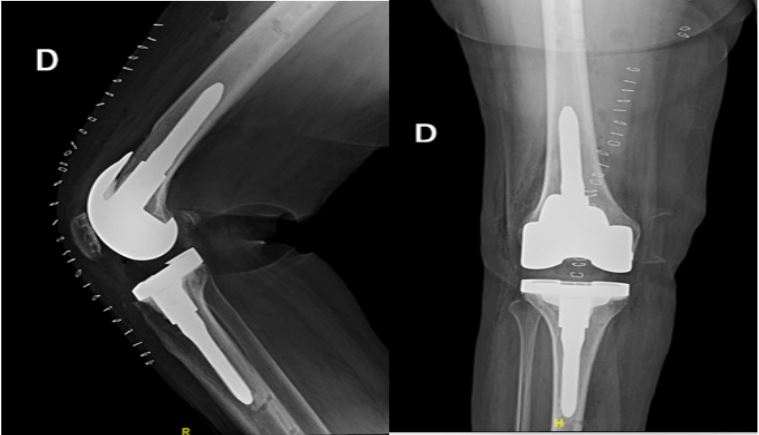
Figure 5: Post-operative implants XR.
The patient underwent spinal anesthesia and a tourniquet was applied. A midline incision over the previous scar was made, followed by a medial arthrotomy. On inspection, the femoral component was oversized, but well-aligned. The patellofemoral button was of appropriate size, but the patellar thickness was inadequate, potentially explaining the knee pain and extensor mechanism stiffness.
The knee was tight in flexion and somewhat loose in extension. After removing the 9 mm polyethylene, femoral and tibial checkpoints, along with CORI array pins, were secured. Real-time intra-operative gap balance and a 3D model of the rTKA were planned. The femoral and tibial components were carefully removed, without significant bone loss. The patellar button was well-fixed and left intact.
Using the operative plan, the CORI robotic arm with a saw attachment made minimal fresh cuts to the femur and tibia. Trial components were implanted, resulting in a well-balanced knee with a 13 mm trial polyethylene insert. Osteophytes around the patella were removed and the joint was irrigated. Femoral and tibial components were cemented and implanted (femur size 4 PS, femoral stem 12 mm X 120 mm, tibial size 2, tibial stem 10 mm X 120 mm), with a 13 mm polyethylene PS insert. Intra-operative tests showed smooth and centered patellar tracking, with knee ROM ranging from -5 to 110 degrees. The operative time was 172 min, a significant increase as compared with our standard (96±23 minutes).
Discussion
Following the surgery, she embarked on a three-week rehabilitation program at our institution’s Rehabilitation Department, commencing five days post-surgery, and achieved a Range of Motion (ROM) of 0-95°.
The patient followed up at 2 weeks, 1, 3 and 6 months, participating in 3 months of outpatient physical therapy to improve ROM and strength.
Her VAS pain scores decreased at each visit, reaching 2/10 at 6 weeks, with no pain medication. The patient displayed excellent clinical progress, reporting no knee pain, instability, or stiffness.
At the latest follow-up, she could ambulate without assistance, with knee ROM of 0-100 degrees and slightly less strength compared to the other leg.
The field of Revision Total Knee Arthroplasty (RATKA) has seen continual advancements aimed at enhancing bone cutting precision, improving component placement accuracy, and ensuring surgical safety [8]. Research suggests that these advancements contribute to reduced complications, preservation of soft tissues [9], increased patient satisfaction, and improved clinical outcomes [10,11].
Despite the considerable focus on Robotic-Assisted Total Knee Arthroplasty (RATKA), there is a scarcity of literature regarding the use of robotics in revision knee arthroplasty, particularly in converting Unicompartmental Knee Arthroplasty (UKA) to Total Knee Arthroplasty (TKA).
One notable case report describes the off-label use of the MAKO robot for revising a failed primary TKA due to aseptic loosening, which resulted in acceptable radiographic outcomes and excellent clinical results [12]. The success of such cases prompts speculation about potential future approvals for similar applications.
The CORI System, announced in 2022, has been identified as suitable for revision knee replacement, combining robotics technology with the Legion Revision Knee System.
This case report marks the first documented instance of utilizing the CORI System for revising a failed primary TKA. The patient exhibited satisfactory radiographic outcomes as evaluated by postoperative X-rays.
With continuous advancements in robotic technology and software capabilities, there is promise for improved surgical outcomes and the expansion of robotic applications across various orthopedic procedures.
Conclusion
The incorporation of robotic technology in revision TKA subsequent to a failed primary procedure represents an innovative approach deserving further exploration. Nonetheless, this system is accompanied by several limitations. Firstly, its use in revision procedures entails significant costs, limiting accessibility to many surgeons, prolonged of operative time and requiring a steep learning curve. Secondly, despite anticipated advantages, there exists insufficient evidence substantiating substantial enhancements in functional outcomes. Lastly, the surgical planning interface displayed on screens can be intricate, demanding experience for precise and efficient operation [13].
It is crucial to recognize that conclusive evidence demonstrating significant improvements in the functional outcomes of patients through the utilization of robotic systems has yet to be established.
Acknowledgement: We thank our Orthopedic department and Institute of Mater Olbia Hospital which has been constantly supportive and motivating.
References
- Brinkman JC, Christopher ZK, Moore ML, Pollock JR, Haglin JM, et al. Patient Interest in Robotic Total Joint Arthroplasty Is Exponential: A 10-Year Google Trends Analysis. Arthroplast Today. 2022; 15: 13-18. doi: 10.1016/j.artd.2022.02.015.
- Postler A, Lützner C, Beyer F, Tille E, Lützner J. Analysis of total knee arthroplasty revision causes. BMC Musculoskelet Disord. 2018; 19: 55.
- MacAskill M, Blickenstaff B, Caughran A, Bullock M. Revision Total Knee Arthroplasty Using Robotic Arm Technology. Arthroplast Today. 2021; 13: 35-42. doi: 10.1016/j.artd.2021.11.003.
- Parvizi J, Tan TL, Goswami K, Higuera C, Della Valle C, et al. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J Arthroplasty. 2018; 33(5): 1309-1314.e2. doi: 10.1016/j.arth.2018.02.078.
- Kemp MA, Metcalfe AJ, Sayers A, Wylde V, Eldridge JD, et al. Does overstuffing of the patellofemoral joint in total knee arthroplasty have a significant effect on postoperative outcomes? Knee. 2018; 25(5): 874-881. doi: 10.1016/j.knee.2018.05.007.
- Gupton M, Johnson JE, Cummings GR, Deivaraju C. Overstuffing the patellofemoral compartment in total knee arthroplasty: A systematic review. Efort open Rev. 2023; 8(8): 597-605. doi: 10.1530/EOR-22-0107.
- Bonnin MP, Schmidt A, Basiglini L, Bossard N, Dantony E. Mediolateral oversizing influences pain, function, and flexion after TKA. Knee Surg Sports Traumatol Arthrosc. 2013; 21(10): 2314-24. doi: 10.1007/s00167-013-2443-x.
- Khlopas A, Sodhi N, Sultan AA, Chughtai M, Molloy RM, et al. Robotic arm-assisted total knee arthroplasty. J Arthroplasty. 2018; 33: 2002-6.
- Khlopas A, Chughtai M, Hampp EL, Scholl LY, Prieto M, et al. Robotic-arm assisted total knee arthroplasty demonstrated soft tissue protection. Surg Technol Int. 2017; 30: 441-6.
- Marchand RC, Sodhi N, Khlopas A, Sultan AA, Harwin SF, et al. Patient satisfaction outcomes after robotic arm-assisted total knee arthroplasty: A short-term evaluation. J Knee Surg. 2017; 30: 849-53.
- Liow MH, Goh GS, Wong MK, Chin PL, Tay DK, et al. Robotic-assisted total knee arthroplasty may lead to improvement in quality-of-life measures: A 2-year follow-up of a prospective randomized trial. Knee Surg Sports Traumatol Arthrosc. 2017; 25: 2942-51.
- Steelman K, Carlson K, Ketner A. Utilization of Robotic Arm Assistance for Revision of Primary Total Knee Arthroplasty: A Case Report. J Orthop Case Rep. 2021; 11(8): 50-54. doi: 10.13107/jocr.2021.v11.i08.2362.
- Batailler C, Hannouche D, Benazzo F, et al. Concepts and techniques of a new robotically assisted technique for total knee arthroplasty: The rosa knee system. Arch Orthop Trauma Surg. 2021; 141: 2049-2058. https://doi.org/10.1007/s00402-021-04048-y.
