
Open Access, Volume 10
Bilateral uterine arteries methotrexate infusion and embolization: A new approach in patient with caesarean scar pregnancy: Case report and literature review
Massimiliano Natrella1 ; Alessandro Messina2*; Bianca Masturzo2 ; Raphael Thommaset3 ; Raffaele Tinelli4 ; Alessandro Libretti5 ; Livio Leo3
1Department of Radiology, Hopital Parini, AUSL Valleè d’Aoste, Aosta, Italy.
2Department of Gynecology and Obstetrics, Degli Infermi Hospital, University of Turin, Ponderano, Biella, Italy.
3Department of Gynecology and Obstetrics, Hopital Beauregard, AUSL Valleè d’Aoste, Aosta, Italy.
4Department of Obstetrics and Gynecology, «Valle d’Itria» Hospital, Martina Franca, Taranto, Italy.
5Department of Obstetrics and Gynecology, University Hospital Maggiore della Carità, Novara, Italy.
Alessandro Messina
Department of Gynecology and Obstetrics, Degli Infermi Hospital, University of Turin, Ponderano, Biella,
Italy.
Email: alessandro.messina@hotmail.it
Received : Mar 22, 2024,
Accepted : Apr 19, 2024
Published : Apr 30, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Background: Cesarean Scar Pregnancy (CSP) is a rare ectopic pregnancy implanted in the myometrium within the site of a previous Cesarean scar. It is associated with severe complications, such as placental implantation, uterine rupture with uncontrolled hemorrhage, infertility or even death.
Case Presentation: A 38-year-old woman, G3P1, underwent a routine early pregnancy scan in Aosta Beauregard Hospital in October 2022. After a transvaginal ultrasound, she was diagnosed with a cesarean scar pregnancy. We present a review of the literature about CSP and our case, successfully treated with uterine artery Methotrexate (MTX) infusion and embolization.
Discussion: Due to the rarity of CSP, the optimal treatment has not been already established. The surgical approach was considered the only possible treatment of these cases but, as most of these women may wish to conceive again, it may be necessary to found conservative treatment options in order to reserve the nonconservative modality just for cases of uncontrolled bleeding.
Keywords: Scar pregnancy; Uterine artery embolization; Methotrexate infusion.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Messina A (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Natrella M, Messina A, Masturzo B, Thommaset R, Tinelli R, Libretti A, Leo L. Bilateral uterine arteries methotrexate infusion and embolization: A new approach in patient with caesarean scar pregnancy: Case report and literature review. Open J Clin Med Case Rep. 2024; 2230.
Introduction
In recent years, due to the increase in the rate of caesarean sections, there has been a major interest in the study of the complications of hysterotomy, including placentation anomalies, uterine rupture and Caesarean Scar Pregnancy (CSP) [1].
CSP accounts for approximately 6% of all ectopic pregnancies in women who have undergone at least one caesarean section [2].
In caesarean scar pregnancy, the pregnancy is implanted in the myometrium at the site of the previous Cesarean scar. It is associated with severe complications, such as placental implantation, uterine rupture with uncontrolled hemorrhage, infertility or even death [3,4].
CSP is characterized by the presence of a gestational sac in the anterior uterine wall, resulting in a reduction in the thickness of the wall between the gestational sac and the bladder and the presence of an empty uterine cavity.
Due to the serious consequences that can arise from CSP, it is essential to carry out a timely and correct diagnosis and treatment.
The symptomatology of CSP is often not so specific, and this makes its diagnosis even more tricky. Moreover, about a third of patients who present with CSP are actually asymptomatic [5].
For these reasons, it is essential that every woman with a positive pregnancy test and a history of previous caesarean section undergo a transvaginal ultrasound during the first trimester of pregnancy. Among differential diagnosis, it is important to exclude a cervical pregnancy or a missed miscarriage [6].
Due to the rarity of CSP, the optimal treatment has not been already established.
The surgical approach was previously considered the only possible treatment of these cases. Plus, there is no consensus regarding the optimal treatment for women who wish to avoid the surgical procedure and individualized therapy should be performed. Moreover since most of these women may wish to conceive again, it is remarkable the necessity to found conservative treatment options in order to reserve the surgical modality for cases of uncontrolled bleeding [7].
The aim of this article is to present a review of the literature about CSP and to report a case of a caesarean scar pregnancy successfully treated with uterine artery Methotrexate (MTX) infusion and embolization.
Case Presentation
A 38-year-old woman, G3P1, underwent a routine early pregnancy scan in Aosta Beauregard Hospital in October 2022. The pregnancy followed a spontaneous conception. The patient underwent a surgically management of termination of pregnancy one year before and a caesarean section for fetal distress four years before. After a transvaginal ultrasound, she was diagnosed with a cesarean scar pregnancy.
At the time of the visit, the serum free-β-Human Chorionic Gonadotropin (β-hCG) values were elevated as in normal pregnancy and there were no signs or symptoms of an ectopic pregnancy.
A transvaginal ultrasound was performed, with the findings of a six weeks’ gestational age vital embryo with a Crown-Rump Length (CRL) of 6 mm. Moreover, it was noted that the gestational sac was implanted at the level of the previous cesarean scar.
The images of pelvis Magnetic Resonance Imaging (MRI) performed during the hospital stay, confirmed the presence of a gestational sac with a diameter of 25 mm, embedded in the anterior lower uterine wall, in close contact with the perimetrium (Figures 1 and 2).
The levels of serum hemoglobin and β-hCG were 13.2 g/dL and 14643 UI/L, respectively. After an adequate counseling of the patient, she agreed for an interventional treatment.
In agreement with the patient, a bilateral uterine arteries methotrexate infusion and embolization was performed. Firstly, catheterization was performed through both right and left femoral arteries in order to reach uterine arteries; then an intra-arterial injection of 50 mg of MTX (first MTX dose), followed by gelatin sponge and non-resorbable microspheres (700-900 micron) for bilateral uterine artery occlusion were administrated. After the procedure, the uterus appeared de-vascularized. No side effects nor complications were noted.
Later on, three doses of MTX were administrated intramuscularly every following days (days 3, 5, 7).
During the in-hospital follow-up period, the patient underwent repeated measurements of β-hCG (on days 5, 7 and 9) and was closely monitored for symptoms and clinical or sonographic signs of pregnancy rupture or hemodynamic instability.
The day after the embolization, a transvaginal scan showed a 14.4 mm sized gestational sac implanted at the level of the previous cesarean scar. The fetal heart activity was absent.
Serum β-hCG declined to a level of 7858 UI/L on the fourth post-procedure day, and 5655 UI/L on the sixth day.
One week after the embolization, another transvaginal scan was performed showing no differences in the gestational sac size. Although this, the sac was noted as closer to the cervical canal. Poor vaginal bleeding was recorded. At this point, vaginal prostaglandin (3 doses of Gemeprost every four hours) ws administrated. After 3 administrations, an ultrasound guided dilatation and curettage was performed without further complications. The post-procedure transvaginal scan showed no more gestational material within the endometrial cavity.
The patient was discharged after 24 hours of follow-up without complications; the β-hCG level was 4247 UI/L.
Summarily, the hospitalized period was 9 days.
Seven days after the discharge, β-hCG was declined to a level of 989 UI/L and a month after the embolization it was 24.9 UI/L.
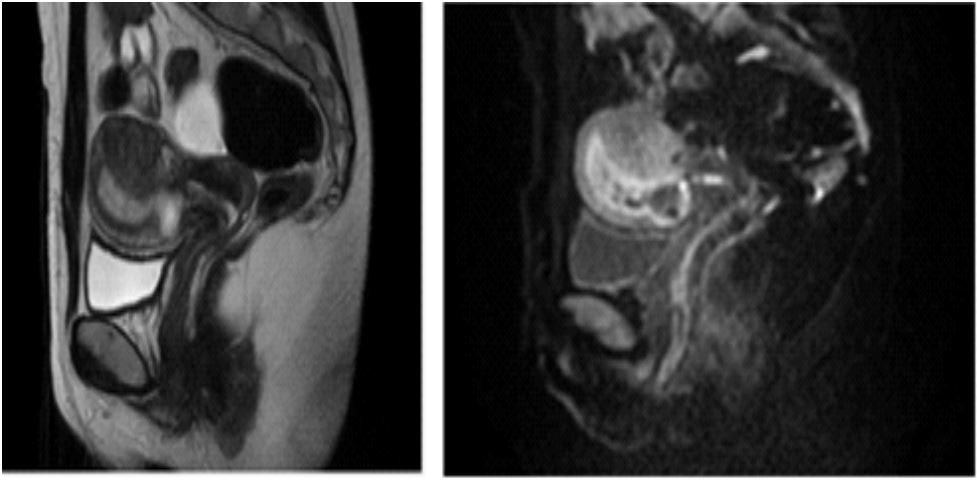
Figure 1 and 2: Pelvic Magnetic Resonance Imaging (MRI) performed before the procedure confirming the presence of
a gestational sac with a diameter of 25 mm, embedded in the anterior lower uterus in close contact with the perimetrium.
Discussion
Caesarean scar pregnancy represents 6,1% of all ectopic pregnancies after cesarean deliveries [3,4]. The incidence varies from 1/1800 to 1/2226, occurring in 1,15% of women with previous cesarean deliveries [3,4]
Few cases of cesarean scar pregnancies are reported within the living literature, although an increase in the caesarean section rate during the last years [3,4].
Caesarean incisions usually heal without any complications. In the past several years, some authors described cesarean scar defects on transvaginal ultrasonography as a wedge-shaped anechoic area suggesting possible impaired healing [2]. The prevalence of cesarean scar defects in a random population of women is up to 84% and is usually asymptomatic [2]. Some authors evaluated the histopathology of uterine wound healing and found different thicknesses of the myometrium along the scar with disordered muscular fibers and elastosis [2]. Althought the mechanism is not clear, it seems that impaired healing of the cesarean incision predisposes to the development of CSP. Factors predisposing to poor wound healing include inadequate closure of the uterine incision, postoperative infections, impaired health conditions such as diabetes or collagen disturbances. Decreased blood flow to the affected tissues predispose to incomplete or delayed healing. Nevertheless, it remains unclear if the technique of the uterine closure during cesarean section (either single or double uterine closure) correlates with the occurrence of CSP [2].
It is difficult to identify the optimal management in individual cases.
If an expectant attitude is assumed, CSP will probably transform into a pregnancy with placenta percreta in the scar and in the lower segment. Considering the possible consequences, early diagnosis and treatment offer much better prognosis.
When making a decision about the management in CSP, the following must be considered: size of pregnancy, presence or absence of uterine continuity, β-hCG level, wish to remain fertile and patient’s hemodynamic state [8,9].
A conservative treatment should be offered to women who wish to conceive again.
The conservative treatment options can be categorized as: reduction of blood supply, systemic chemotherapy, and local chemotherapy or feticide [10]. The most commons methods are systemic MTX (33,9%), uterine artery embolization (21,9%), dilatation and curettage (14,1%), hysterotomy (10,6%) and hysteroscopy (6,7%). Combined treatment methods are applied more rarely: TA US or TV US + local MTX treatment in 6,6% of cases, TV US + gestational sac aspiration in 3,7% of cases, TV US or TA US + local injection of vasopressin or potassium chloride in 1% of cases and bilateral hypogastric artery ligation in 0,1% of cases.
Dilatation and curettage with subsequent intrauterine Foley catheter insertion may be recommended, but only due to its availability, simplicity and relatively high efficacy. However, bearing in mind significant risk of hemorrhage and high risk of secondary hysterectomy and fertility loss, this form of treatment should only be used in selected cases of early diagnosed CSP [11,12].
Conservative treatment with systemic Methotrexate (MTX) alone has shown favorable results in non-tubal ectopic pregnancies, although the effectiveness of this treatment decreased dramatically in high (>10,000 IU/L)levels of beta-Human Chorionic Gonadotropin (b-HCG) or in cases with fetal cardiac activity [6,10,13]. The failure rates of monotherapy with MTX, in fact, is approximately 57% in CS scar pregnancies [14].
It has been proposed that simultaneous systemic and local MTX administration for CSP with β-hCG levels above 10,000 mLU/mL may be a very effective method that does not require further interventions. Systemic MTX administration seems to be the most effective for CSP with β-hCG below 5,000 IU/mL, and should be limited to two doses, 1 mg/kg body weight each, to avoid adverse effects. In the case of systemic MTX therapy, serial color Doppler scans are useful for CSP monitoring and seem to correlate well with serum beta hCG [12].
It therefore appears that systemic methotrexate treatment should not be applied on the routine basis due to relatively low efficacy, high risk of hysterectomy and fertility loss, and the risk of various adverse effects. On the other hand, local methotrexate therapy (under ultrasound or hysteroscopy guidance) should be considered a perfect management method as it offers fertility preservation in asymptomatic pregnant patients without concomitant hemodynamic disorders. The most effective CSP treatment is simultaneous application of 2-3 techniques [11,12].
Uterine Artery Embolization (UAE) is currently used in obstetrics and gynecology as a treatment modality for uterine fibroids or to control obstetric hemorrhage. Recently, this modality was considered when treating non-tubal ectopic pregnancies [15-17], particularly in cases when the trophoblasts are deeply embedded in myometrium. Previous reports, however, had a relatively small sample size [8], or used it in combination with other surgical procedures (e.g. dilation and curettage) to control bleeding and in many cases, an emergency surgical procedure and even hysterectomy were unavoidable [8,9,17]. The MTX infusion during the UAE allows to further decrease blood HCG level.
Since monotherapy with either systemic MTX or UAE has shown only moderate success rates, some studies analyzed the effectiveness and safety of uterine artery MTX infusion and embolization combined with systemic MTX for treatment of non-tubal ectopic pregnancy in women who wish fertility preservation and desire to avoid surgical treatment [18]. The conservative treatment protocol applied in this case report included a total of 4 MTX doses. The first one was administered during the percutaneous catheterization of the femoral artery by intra-arterial injection of 50 mg of MTX, just before injecting gelatin sponge and nonresorbable microspheres (700-900 micron) for bilateral uterine artery occlusion. The remaining 3 doses were given intramuscularly every other day.
The rationale for this treatment protocol, as underlined by Krissi et al. [18], was to increase the success rate of conservative treatment by combining two modalities, each with moderate effectiveness.
The hospital stay period was 9 days, in accordance with previous studies [19].
Conclusion
This case report seems to confirm that the combination therapy of uterine artery methotrexate infusion and embolization together with systemic MTX can be considered as a safe and effective treatment of cesarean-scar pregnancies.
Declarations
Authors contributions: M.N Conceptualization and Writing-original draft; A.M Writing-original draft; B.M Supervision and Writing-review & editing; R.T Data curation, Formal Analysis, R.T Methodology; L.L Supervision, Writing-review & editing; A.L. supervision, review & editing
Funding: None.
Disclosure of interests: None declared.
Ethical approval: Informed consent: Informed consent was obtained from the patient for data recovery for research purposes, explaining the purpose of the article and the importance of the clinical data used for the scientific community
Data sharing: Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
References
- O’Neill SM, Khashan AS, Kenny LC, Greene RA, Henriksen TB, et al. Caesarean section and subsequent ectopic pregnancy: Asystematic review and meta-analysis. BJOG. 2013; 120(6): 671-80. doi: 10.1111/1471-0528.12165.
- Gonzalez N, Tulandi T. Cesarean Scar Pregnancy: A Systematic Review. J Minim Invasive Gynecol. 2017; 24(5): 731-738. doi: 10.1016/j.jmig.2017.02.020.
- Zhou X, Li H, Fu X. Identifying possible risk factors for cesarean scar pregnancy based on a retrospective study of 291 cases. J Obstet Gynaecol Res. 2020; 46(2): 272-278. doi: 10.1111/jog.14163.
- Rotas MA, Haberman S, Levgur M. Cesarean scar ectopic pregnancies: Etiology, diagnosis, and management. Obstet Gynecol. 2006; 107(6): 1373-81. doi: 10.1097/01.AOG.0000218690.24494.ce.
- Riaz RM, Williams TR, Craig BM, Myers DT. Cesarean scar ectopic pregnancy: Imaging features, current treatment options, and clinical outcomes. Abdom Imaging. 2015; 40(7): 2589-99. doi: 10.1007/s00261-015-0472-2.
- Jurkovic D, Hillaby K, Woelfer B, Lawrence A, Salim R, et al. First-trimester diagnosis and management of pregnancies implanted into the lower uterine segment Cesarean section scar. Ultrasound Obstet Gynecol. 2003; 21(3): 220-7. doi: 10.1002/uog.56.
- Chetty M, Elson J. Treating non-tubal ectopic pregnancy. Best Pract Res Clin Obstet Gynaecol. 2009; 23(4): 529-38. doi: 10.1016/j.bpobgyn.2008.12.011.
- An X, Ming X, Li K, Wang J. The analysis of efficacy and failure factors of uterine artery methotrexate infusion and embolizationin treatment of cesarean scar pregnancy. ScientificWorldJournal. 2013; 2013: 213603. doi: 10.1155/2013/213603.
- Zhang B, Jiang ZB, Huang MS, Guan SH, Zhu KS, et al. Uterine artery embolization combined with methotrexate in the treatment of cesarean scar pregnancy: Results of a case series and review of the literature. J Vasc Interv Radiol. 2012; 23(12): 1582-8. doi: 10.1016/j.jvir.2012.08.013.
- Cassik P, Ofili-Yebovi D, Yazbek J, Lee C, Elson J, et al. Factors influencing the success of conservative treatment of interstitial pregnancy. Ultrasound Obstet Gynecol. 2005; 26(3): 279-82. doi: 10.1002/uog.1961.
- Calì G, Timor-Tritsch IE, Palacios-Jaraquemada J, Monteaugudo A, Buca D, et al. Outcome of Cesarean scar pregnancy managed expectantly: Systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2018; 51(2): 169-175. doi: 10.1002/uog.17568.
- Pędraszewski P, Wlaźlak E, Panek W, Surkont G. Cesarean scar pregnancy - a new challenge for obstetricians. J Ultrason. 2018;18(72): 56-62. doi: 10.15557/JoU.2018.0009.
- Hung TH, Shau WY, Hsieh TT, Hsu JJ, Soong YK, et al. Prognostic factors for an unsatisfactory primary methotrexate treatmentof cervical pregnancy: A quantitative review. Hum Reprod. 1998; 13(9): 2636-42. doi: 10.1093/humrep/13.9.2636.
- Li N, Zhu F, Fu S, Shi X. Transvaginal ultrasound-guided embryo aspiration plus local administration of low-dose methotrexate for caesarean scar pregnancy. Ultrasound Med Biol. 2012; 38(2): 209-13. doi: 10.1016/j.ultrasmedbio.2011.10.012.
- Van Mello NM, Mol F, Ankum WM, Mol BW, van der Veen F, et al. Ectopic pregnancy: How the diagnostic and therapeutic management has changed. Fertil Steril. 2012; 98(5): 1066-73. doi: 10.1016/j.fertnstert.2012.09.040.
- Kung FT, Chang SY. Efficacy of methotrexate treatment in viable and nonviable cervical pregnancies. Am J Obstet Gynecol.1999; 181(6): 1438-44. doi: 10.1016/s0002-9378(99)70389-3.
- Yang XY, Yu H, Li KM, Chu YX, Zheng A. Uterine artery embolisation combined with local methotrexate for treatment of caesarean scar pregnancy. BJOG. 2010; 117(8): 990-6. doi: 10.1111/j.1471-0528.2010.02578.x.
- Krissi H, Hiersch L, Stolovitch N, Nitke S, Wiznitzer A, et al. Outcome, complications and future fertility in women treated with uterine artery embolization and methotrexate for non-tubal ectopic pregnancy. Eur J Obstet Gynecol Reprod Biol. 2014; 182: 172-6. doi: 10.1016/j.ejogrb.2014.09.026.
- Zeng S, Wang Y, Ye P, Xu L, Han W, et al. Comparing the clinical efficacy of three surgical methods for cesarean scar pregnancy.BMC Womens Health. 2023; 23(1): 271. doi: 10.1186/s12905-023-02415-y.
