
Open Access, Volume 10
Predictive value of BALF IL-6, Serum IL-6, CRP and SSA on pleural effusion in children with MPP
Yishuai Ren; Xinquan Sang; Xue Liu; Fenglian Zhu*
Department of Pediatrics, The First Affiliated Hospital of Xinxiang Medical College, No. 88, Health Road, Xinxiang City, 453100, Henan Province, China.
Fenglian Zhu
Department of Pediatrics, The First Affiliated Hospital of Xinxiang Medical College, No. 88, Health Road, Xinxiang City, 453100,
Henan Province, China.
Email: picu3390@126.com
Received : Mar 22, 2024,
Accepted : Apr 17, 2024
Published : Apr 19, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Objective: This study aimed to analyze the clinical characteristics of children with Mycoplasma Pneumoniae Pneumonia (MPP) and assess the predictive value of Balf IL-6, serum IL-6, CRP and SSA for pleural effusion in pediatric MPP cases.
Methods: Between May 17, 2020, and February 24, 2024, 77 patients admitted to The First Clinical College of Xinxiang Medical University who underwent Bronchoalveolar Lavage (BAL) treatment were categorized into groups based on the presence or absence of pleural effusion. Clinical data was collected and analyzed using Pearson correlation to investigate the relationship between inflammatory factors and clinical manifestations. Additionally, ROC curve analysis was performed to determine the predictive capability of inflammatory factors for pleural effusion
Results: The presence of IL-6 in bronchoalveolar lavage fluid showed a significant positive correlation with fever days, duration of fever, levels of CRP, WBC count, and length of hospital stay post-antibiotic treatment. The ROC curve analysis indicated that the AUC for serum IL-6 was 0.77 with a cut-off value of 0.5, sensitivity of 71.43%, specificity of 77.57%, and a 95% confidence interval of 0.652-0.888. Similarly, the AUC for lavage IL-6 was 0.693 with a sensitivity of 66.67%, specificity of 69.64%, and a 95% confidence interval of 0.562-0.823. Additionally, the AUC for serum amyloid A was 0.648, with a 95% confidence interval of 0.517- 0.78, a cut-off value of 0.3452, sensitivity of 95.24%, and specificity of 39.29%. The AUC for hypersensitive C-reactive protein was 0.689, with a 95% confidence interval of 0.547-0.831, a cut-off value of 0.3869, sensitivity of 61.9%, and specificity of 76.79%.
Conclusion: Serum and lavage fluid IL-6, SSA, and CRP are good predictors of pleural effusion.
Keywords: Mycoplasma pneumoniae pneumonia; Pleural effusion; Inflammatory factors; Predictive value.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Zhu F (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Ren Y, Sang X, Liu X, Zhu F. Predictive value of BALF IL-6, Serum IL-6, CRP and SSA on pleural effusion in children with MPP. Open J Clin Med Case Rep. 2024; 2229.
Introduction
Mycoplasma Pneumoniae Pneumonia (MPP) is a frequent cause of Community-Acquired Pneumonia (CAP) in school-age children [1], with an incidence rate ranging from 10% to 40%. The absence of children from school and parents not only impacts academic progress and future development but can also lead to decreased family income, exacerbating the economic burden. MPP can be challenging to diagnose early on and progresses rapidly [2]. Without prompt and effective treatment, serious pulmonary complications like bronchiectasis, atelectasis, pulmonary abscess, necrotising pneumonia, pleural effusion, and even pulmonary embolism can occur [3].
IL-6 plays a key role in pneumonia by promoting inflammatory and immune responses, leading to the recruitment of neutrophils that release enzymes and oxygen radicals to combat pathogens, potentially causing lung tissue damage [4]. Acute phase reactants like SAA, protein, and C-reactive protein are crucial markers that significantly increase in serum levels following trauma, infection, and other stimuli [5,6].
This study aims to analyze the clinical characteristics of children with MPP and investigate the predictive value of IL-6, CRP, and SSA for pleural effusion in children with MPP. The goal is to offer a more precise and effective foundation for early identification and treatment of pleural effusion in children with MPP.
Research Methods
Study subjects
Seventy-seven patients diagnosed with MPP were included in this study, conducted at The First Clinical College of Xinxiang Medical University between 17 May 2020 and 24 February 2024. Approval for this retrospective study was obtained from the Ethics Committee of the First Affiliated Hospital of Xinxiang Medical College (Ethics number EC-024-068). Due to the retrospective nature of the study, informed consent from the children and their guardians was not necessary. Inclusion criteria and exclusion criteria.
(1) Inclusion criteria:
① Age: 3-14years old;
② Multiplex Polymerase Chain Reaction (Polymerase Chain Reaction, PCR) of pharyngeal swabs and alveolar lavage fluid was positive for MP-DNA;
③ Meet the diagnostic criteria for bronchopneumonia [7];
(2) Exclusion criteria:
① Hospital-acquired pneumonia, chronic respiratory diseases (such as asthma, bronchitis, active tuberculosis), other pathogenic infections, malignant tumors, foreign body inhalation, immune deficiency, organ transplantation, congenital genetic metabolic diseases, intolerance to Bronchoalveolar Lavage (BAL);
② Parents or guardians refuse to perform BAL;
③ The information is incomplete.
(3) Guidelines for flexible bronchoscopy in China (2018 edition) Indications for fiberoptic bronchoscopic alveolar lavage: Chest imaging indicated pulmonary consolidation, atelectasis, and unknown etiology. BAL obtained the consent of the family members to do the examination and signed the consent form.
General information
Clinical data collected for analysis included age, sex, height, weight, peak body temperature, length of hospital stay, presence of fever before hospitalization, duration of macrolide treatment, number of days with fever, prehospital medical history, Mycoplasma pneumoniae DNA load in Bronchoalveolar Lavage Fluid (BALF) and throat swab, White Blood Cell Count (WBC), Neutrophil ratio (NE), platelet count, C-Reactive Protein (CRP) levels, Procalcitonin (PCT) levels, BALF and serum Interleukin-6 (IL-6) levels, Lactate Dehydrogenase (LDH) levels, D-dimer levels, time of alveolar lavage post admission, and chest Computed Tomography (CT) findings within 24 hours of admission for recording any complications.
Statistical analysis
Non-normally distributed variables were described using the median (IQR), while normally distributed continuous variables were presented as mean ± standard deviation. Categorical variables were reported as percentages and compared using chi-square test, Fisher’s exact test, or continuous corrected chisquare test. Differences between groups were assessed using independent sample t-test or Mann-Whitney U test. Pearson correlation analysis was used to examine the relationship between inflammatory factors, fever, and time to discharge. Receiver Operating Characteristic (ROC) curves were utilized to evaluate their discriminative ability. Statistical significance was defined as a p-value less than 0.05.
Results
Comparison of the clinical phenotype between pleural effusion and the group without pleural effusion
The duration of fever and hospitalization was significantly longer in the pleural effusion group (P <0.05). Additionally, the proportion of neutrophils, CRP, LDH, SSA, D dimer, FDP, serum, and lavage interleukin 6 were significantly higher in this group compared to the other group (P<0.05).
Correlation between inflammatory factors and clinical manifestations
IL-6 levels in Bronchoalveolar Lavage (BAL) were found to be positively correlated with the duration of fever, fever time, C-Reactive Protein (CRP) levels, white blood cell count, and length of hospital stay following antibiotic treatment. Additionally, serum IL-6 levels were positively correlated with fever duration, CRP levels, Lactate Dehydrogenase (LDH) levels, and D-dimer levels following antibiotic treatment. The length of hospital stay showed positive correlations with fever duration, Neutrophil (NE) levels, CRP levels, LDH levels, Soluble Serum Antigen (SSA) levels, and the number of days post antibiotic treatment. NE, CRP, LDH, and SSA levels were all positively correlated with both the length of hospital stay and the duration of fever following antibiotic treatment.
Table 1: Comparison of clinical phenotypes between pleural effusion and the group without pleural effusion.
| Variable | There was no pleural effusion (n=56) | pleural effussion (n=21) | Z /χ2 | P |
|---|---|---|---|---|
| age | 7.00 (5.27, 9.00) | 7.00 (4.00, 9.00) | 0.287 | 0.774 |
| weight | 24.00(21.00, 33.88) | 24.50(18.00, 29.00) | 0.486 | 0.627 |
| height | 125.00(119.00, 139.50) | 126.00(109.00, 137.50) | 0.309 | 0.757 |
| length of stay | 8.00(7.00, 13.00) | 10.00(9.00, 12.50) | 2.558 | 0.011 |
| thermal spike | 39.30(39.00, 39.68) | 39.60(39.00, 40.00) | 1.708 | 0.088 |
| Fever days | 8.00(6.00, 12.00) | 8.00(6.00, 12.00) | 0.149 | 0.881 |
| Time of fever after antibiotic application | 8.50(7.00, 13.00) | 10.00(9.00, 11.50) | 2.061 | 0.039 |
| MP-DNA copies/mL | 8950000.00(490750.00, 78275000.00) |
20600000.00(1708000.00, 233500000.00) |
0.932 | 0.351 |
| White blood cell value | 7.98(6.49, 10.15) | 8.00(6.25, 10.28) | 0.074 | 0.941 |
| Neutrophil values | 69.70(57.88, 77.43) | 75.40(72.10, 83.45) | 3.02 | 0.003 |
| Platelet number | 286.50(239.00, 385.00) | 265.00(230.00, 328.00) | 0.949 | 0.342 |
| Hypersensitive C-reactive protein | 15.54(5.63, 30.66) | 34.67(15.79, 99.59) | 2.545 | 0.011 |
| lactic dehydrogenase | 270.00(235.00, 316.75) | 408.00(295.00, 558.50) | 3.066 | 0.002 |
| SSA | 131.00(46.30, 316.95) | 161.80(107.20, 417.85) | 1.996 | 0.046 |
| D dimer | 0.96(0.67, 2.06) | 2.13(1.48, 4.83) | 3.958 | < 0.001 |
| FDP | 2.39(1.74, 4.31) | 4.06(3.04, 9.89) | 3.283 | 0.001 |
| The first few days of irrigation | 1.00(1.00, 2.00) | 1.00(1.00, 2.00) | 0.453 | 0.651 |
| Pre-hospital disease course | 7.00(5.00, 10.75) | 6.00(5.50, 9.50) | 0.426 | 0.67 |
| IL-6 | 21.85(16.45, 41.71) | 73.93(36.16, 117.07) | 3.632 | < 0.001 |
| BAL-IL-6 | 41.70(36.65, 85.60) | 91.45(46.87, 136.72) | 2.591 | 0.01 |
| sex | 31(55.40%) | 9(42.90%) | 0.956 | 0.328 |
| consolidation | 53(94.60%) | 20(95.20%) | 0.03 | >0.99 |
| RMPP | 15(26.80%) | 13(61.90%) | 8.14 | 0.004 |
The ROC curve of the predictive value of the inflammatory index on the pleural effusion
ROC curve analysis was conducted to evaluate the predictive value of pleural effusion markers. The Area Under the Curve (AUC) for serum IL-6 was 0.77 with a cut-off value of 0.5, demonstrating a sensitivity of 71.43% and specificity of 77.57% (95% CI: 0.652-0.888). For lavage IL-6, the AUC was calculated to be 0.648 with a cut-off value of 0.3631, showing a sensitivity of 66.67% and specificity of 69.64% (95% CI: 0.562-0.823). Additionally, the AUC for SSA was 0.648 (95% CI: 0.517-0.78) with a cut-off value of 0.3452, yielding a sensitivity of 95.24% and specificity of 39.29%. Lastly, the AUC for hypersensitive C-reactive protein was 0.689 (95% CI: 0.547-0.831) with a cut-off value of 0.3869, showing a sensitivity of 61.9% and specificity of 76.79%.
Table 2: Correlations between inflammatory factors and clinical manifestations.
| Length of stay | Fever days |
Time of fever after antibiotic application |
||||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| Thermal spike | 0.078 | 0.503 | 0.034 | 0.768 | 0.092 | 0.425 |
| Time of fever after antibiotic application | 0.916** | 0.000 | 0.309** | 0.006 | 1.000 | . |
| The first few days of irrigation | 0.397** | 0.000 | 0.018 | 0.877 | 0.344** | 0.002 |
| Pre-hospital disease course | 0.076 | 0.509 | 0.667** | 0.000 | 0.024 | 0.839 |
| White blood cell ratio | 0.023 | 0.842 | 0.011 | 0.924 | 0.012 | 0.915 |
| NE | 0.328** | 0.004 | 0.097 | 0.400 | 0.309** | 0.006 |
| CRP | 0.362** | 0.001 | 0.008 | 0.947 | 0.278* | 0.014 |
| LDH | 0.334* | 0.003 | 0.220 | 0.055 | 0.285* | 0.012 |
| SSA | 0.459** | 0.000 | 0.108 | 0.348 | 0.365** | 0.001 |
| BALF IL-6 | 0.409** | 0.000 | 0.230* | 0.045 | 0.448** | 0.000 |
| Serum IL-6 | 0.418** | 0.000 | 0.139 | 0.227 | 0.389** | 0.000 |
Table 3: ROC curves of the predictive value of inflammatory indicators on pleural effusion.
| Variable | AUC | P | 95%confidence interval | cutoff value | sensibility | specificity |
|---|---|---|---|---|---|---|
| IL-6 | 0.77 | <0.001 | 0.652-0.888 | 0.5 | 71.43 | 78.57 |
| BALF IL-6 | 0.693 | 0.004 | 0.562-0.823 | 0.3631 | 66.67 | 69.64 |
| SSA | 0.648 | 0.027 | 0.517-0.78 | 0.3452 | 95.24 | 39.29 |
| CRP | 0.689 | 0.009 | 0.547-0.831 | 0.3869 | 61.9 | 76.79 |
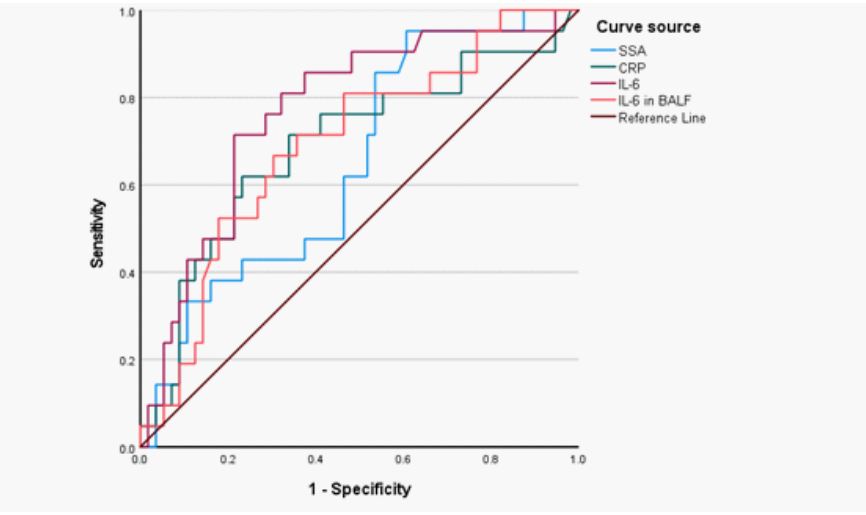
Figure 1: The ROC curve of the predictive value of the inflammatory indicators on the pleural effusion.
Discussion
The study results demonstrated a positive correlation between serum and lavage fluid IL-6, NE, CRP, LDH, SSA, D-dimer, and FDP levels with both length of hospitalization and fever duration following antibiotic treatment. Furthermore, the findings indicated that MPP patients with pleural effusion experienced prolonged fever duration and hospital stay post-antibiotic treatment compared to those without pleural effusion. Additionally, elevated levels of neutrophil proportions, CRP, LDH, SSA, D-dimer, FDP, and IL-6 in serum and lavage fluid were observed in these patients. These results are consistent with existing literature and offer valuable insights into the pathogenesis of pleural effusions in RMPP and their impact on disease progression.
The presence of pleural effusion in patients with Mycoplasma Pneumoniae Pneumonia (MPP) often indicates a worsening of pulmonary inflammation and the progression of pathological damage [8]. This may be linked to the severity of the M. pneumoniae infection and the body’s immune response. Consequently, individuals with pleural effusion typically require an extended treatment duration to eliminate pathogens, manage inflammation, and facilitate tissue repair. As a result, these patients may experience a longer hospital stay and persistent fever post-antibiotic therapy. Studies suggest that MPP patients with pleural effusion exhibit a more intense inflammatory response and greater pathological damage [9]. Furthermore, clinical and imaging parameters, such as prolonged fever, pleural effusion, extrapulmonary complications, and extensive pulmonary consolidation on X-ray, are closely associated with the risk of refractory MPP [10]. Elevated levels of IL-6 in plasma and/or bronchoalveolar fluid have been identified as early indicators of lung injury and predictors of prolonged mechanical ventilation, organ dysfunction, morbidity, and mortality in lung diseases [11].
In the context of M. pneumoniae pneumonia, CRP plays a crucial role in the immune and inflammatory responses, aiding in pathogen clearance and tissue protection. Monitoring CRP levels can also assist in assessing disease severity and treatment efficacy [12]. Research has shown that patients with concurrent pleural effusion MPP exhibit elevated CRP levels compared to those without pleural effusion. Jiang et al. identified SAA, CRP, and PCT as specific markers for early childhood MP infection. SAA expression levels can indicate the severity of bacterial pneumonia, with the combined detection of CRP and PCT offering the highest diagnostic accuracy [13].
Boundedness: This retrospective study is based on data from a single center with a limited sample size, potentially impacting the generalizability and precision of the study findings.
Conclusion
Serum and lavage fluid IL-6, SSA, and CRP are good predictors of pleural effusion and have good clinical applications.
References
- Mendez R, Banerjee S, Bhattacharya SK, et al. Lung inflammation and disease: A perspective on microbial homeostasis and metabolism [J]. IUBMB life. 2019; 71(2): 152-65.
- Neeser OL, Vukajlovic T, Felder L, et al. A high C-reactive protein/procalcitonin ratio predicts Mycoplasma pneumoniae infection [J]. Clin Chem Lab Med. 2019; 57(10): 1638-46.
- Shan L S, Liu X, Kang X Y, et al. Effects of methylprednisolone or immunoglobulin when added to standard treatment with intravenous azithromycin for refractory Mycoplasma pneumoniae pneumonia in children [J]. World J Pediatr. 2017; 13(4): 321-7.
- Khaedir Y, Kartika R. Perspectives on Targeting IL-6 as a Potential Therapeutic Strategy for COVID-19 [J]. Journal of interferon & cytokine research: The official journal of the International Society for Interferon and Cytokine Research. 2021; 41(2): 37-43.
- Jiang Y, Wang W, Zhang Z, et al. Serum amyloid a, C-reactive protein, and procalcitonin levels in children with Mycoplasma pneumoniae infection [J]. Journal of clinical laboratory analysis. 2022; 36(3): e24265.
- Sack G H, Jr. Serum Amyloid A (SAA) Proteins [J]. Sub-cellular biochemistry. 2020; 94: 421-36.
- Nascimento-Carvalho C M. Community-acquired pneumonia among children: The latest evidence for an updated management [J]. J Pediatr (Rio J). 2020; 96(1): 29-38.
- Ling Y, Ning J, Xu Y. Explore the Predictive Value of Peripheral Blood Cell Parameters in Refractory Mycoplasma pneumoniae Pneumonia in Children Over 6 Years Old [J]. Front Pediatr. 2021; 9: 659677.
- Zhang X, Yu Y. Severe pediatric Mycoplasma pneumonia as the cause of diffuse alveolar hemorrhage requiring veno-venous extracorporeal membrane oxygenation: A case report [J]. Front Pediatr. 2022; 10: 925655.
- Gong H, Sun B, Chen Y, et al. The risk factors of children acquiring refractory mycoplasma pneumoniae pneumonia: A metaanalysis [J]. Medicine. 2021; 100(11): e24894.
- McElvaney O J, Curley G F, Rose-John S, et al. Interleukin-6: Obstacles to targeting a complex cytokine in critical illness [J]. The Lancet Respiratory medicine. 2021; 9(6): 643-54.
- Zangari T, Ortigoza M B, Lokken-Toyli K L, et al. Type I Interferon Signaling Is a Common Factor Driving Streptococcus pneumoniae and Influenza A Virus Shedding and Transmission [J]. mBio. 2021; 12(1).
- Su W, Ju L, Hua Q, et al. Values of combined C-reactive protein, procalcitonin and serum amyloid A in differential diagnosis of bacterial and non-bacterial community acquired pneumonia in children [J]. Diagn Microbiol Infect Dis. 2023; 105(2): 115865.
