
Open Access, Volume 10
A case of granulomatosis with polyangiitis presenting as cerebritis
Burce Isik1,2*; Matthew G Davey2; Alwin Sebastian1,2; Alexander Fraser1,2
1University of Limerick School of Medicine, Co. Limerick, Republic of Ireland.
2University Hospitals Limerick, Co. Limerick, Republic of Ireland.
Burce Isik
University of Limerick School of Medicine, Co. Limerick, Republic of Ireland.
Email: 21149747@studentmail.ul.ie
Received : Mar 21, 2024,
Accepted : Apr 17, 2024
Published : Apr 19, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Background: Isolated Central Nervous System (CNS) involvement in Granulomatosis with Polyangiitis (GPA) is rare. There are limited accounts of such a presentation in the literature.
Case presentation: A 61-year-old gentleman presented with right upper limb and lower limb weakness, slurred speech and confusion following two instances of mechanical falls while at home. A cerebrovascular event was suspected. He underwent Computed Tomography (CT) brain and Magnetic Resonance Imaging (MRI) brain which demonstrated leptomeningeal thickening of left frontal region with vasogenic oedema. The differential diagnosis included malignancy, infection and contusion. He initially commenced on Dexamethasone 8 mg, Keppra 250 mg and a combination of Ceftriaxone, Linezolid, Metronidazole to treat vasogenic edema and possible infectious cerebritis, respectively. His vasculitis screen demonstrated a positive p-ANCA, positive for high titer PR3-ANCA. He was diagnosed with cerebral vasculitis secondary to GPA and commenced on immunosuppressant treatment.
Conclusion: GPA with isolated CNS involvement can mimic the presentations of acute stroke, cerebritis, malignancy, and traumatic brain injury due to ambiguous symptoms. In the absence of other symptoms of GPA, isolated cerebral vasculitis often leads to delayed presentation, diagnosis, and treatment of this rare disease.
Keywords: Granulomatosis with polyangiitis; Cerebral vasculitis; Vasculitis; P-ANCA; PR3-ANCA.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Isik B (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Isik B, Davey MG, Sebastian A, Fraser A. A case of granulomatosis with polyangiitis presenting as cerebritis. Open J Clin Med Case Rep. 2024; 2228.
Introduction
Granulomatosis with Polyangiitis (GPA) is a rare systemic autoimmune disease, with an incidence rate of 0.4-11.9 cases per 1 million person-years P1]. GPA tends to be characterized by necrotizing and granulomatous inflammation of small and medium sized vessels at biopsy, with a propensity to affect the upper airway, pulmonary and renal organs [1]. Notwithstanding this, less common manifestations of GPA include the Central Nervous System (CNS), gastrointestinal tract, and breast parenchyma [2], rendering diagnosis often challenging to the clinician which leads to later diagnosis and initiation of the appropriate management. GPA is strongly associated with ANCA and PR3-ANCA positivity [1]. However, the ANCA positivity alone is not sufficient to diagnose this type of vasculitis [3]. Herein, we report a case of GPA with an uncommon initial presentation of perinuclear-ANCA (p-ANCA) and Proteinase 3 (PR3) positive isolated cerebral vasculitis.
Case Report
A 61-year-old gentleman with no previous medical background was presented to Emergency Department (ED) following an unwitnessed collapse on two separate occasions in a 7-day period, with the second fall leading to a head injury due to loss of consciousness. He had associated right upper limb and lower limb weakness, mixed aphasia, with poor recollection of the events, however his presentation was delayed. He also has ongoing intermittent epistaxis and did not report any history of headaches. He was self-medicated with 600 mg of Aspirin after the collapse and did not seek medical attention until after 2 days later, when there was no improvement in his symptoms. He was an active smoker of a pack a day and he consumed an average of 10 units of alcohol a day.
On review in the ED, his Glasgow Coma Scale (GCS) was 15/15, however he demonstrated right upper and lower limb weakness (recorded as 3.5 out of 5 by the reviewing doctor), marked slurring of speech, as well as ecchymosis to upper lip at the trauma site. This gentleman had no recollection of precipitating events, however fortunately he had no signs of major head trauma or cranial fracture. On admission he underwent Computed Tomography (CT) of the brain with contrast which demonstrated thickening of the cortex in the left frontal region, with associated vasogenic edema and enhancement extending into the sulci, with local mass effect but no evidence of intracranial hemorrhage or ischemia nor herniation (Figure 1). There was mucosal opacification of left ethmoid and maxillary paranasal sinuses with slight nasal septum deviation to the right on CT brain consistent with the history of epistaxis.
He commenced on Dexamethasone 8mg orally (PO) and Keppra 250mg. A subsequent magnetic resonance imaging (MRI) of the brain demonstrated vasogenic oedema and abnormal leptomeningeal enhancement in left frontal lobe with evidence of subarachnoid blood (Figure 2).
At this time, the clinical and radiological differentials included infectious meningitis (with underlying evolving cerebritis), neoplastic process, or left frontal post-traumatic Subarachnoid Haemorrhage (SAH) with an underlying contusion, albeit less likely. A CT of the thorax, abdomen and pelvis was performed to determine whether there was a primary source for the indeterminant left frontal lobe lesion. This investigation yielded no causative pathology. He subsequently commenced on Ceftriaxone 2 g Intravenously (IV), Linezolid 600 mg IV, and Metronidazole 500 mg IV. This case was discussed at this time with the local neurosurgical services who recommended a repeat MRI brain performed a week after the initial presentation.
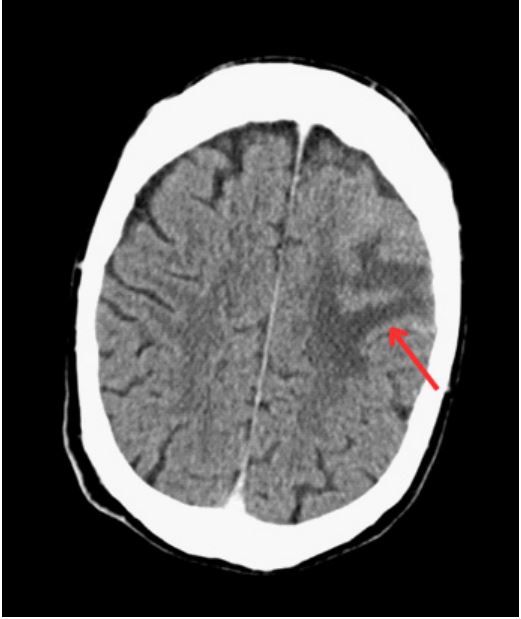
Figure 1: CT Brain with contrast demonstrated thickening of the cortex in the left frontoparietal region, with associated vasogenic edema and enhancement extending into the sulci, with localised mass effect but no herniation.
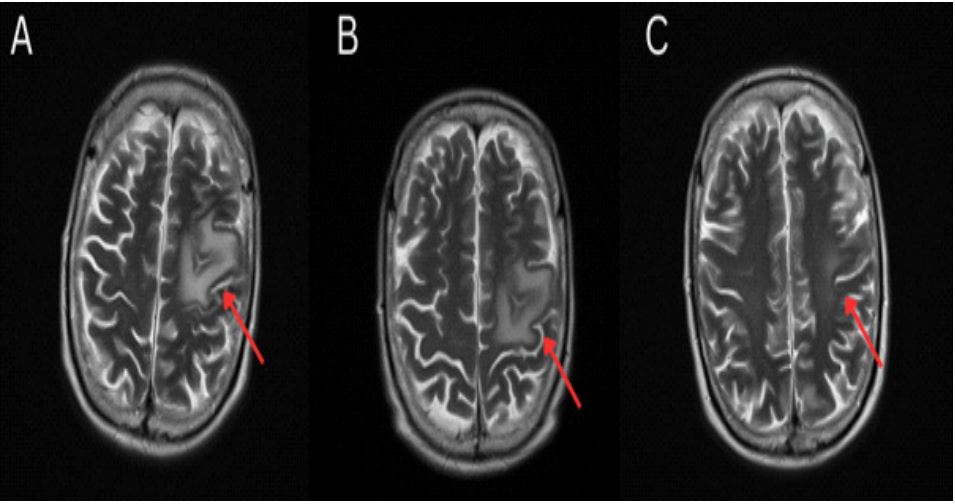
Figure 2: (A) MRI brain demonstrated vasogenic oedema and abnormal leptomeningeal enhancement in left frontal lobe
with evidence of subarachnoid blood; (B) MRI brain one week later demonstrated ongoing vasogenic oedema, with interval
decrease in leptomeningeal enhancement and stable leptomeningeal hemosiderin deposits, with no frank subarachnoid haemorrhage; (C) MRI brain on treatment demonstrating resolution of leptomeningeal thickening and vasogenic edema.
Clinically, the patient remained stable, with some improvement with time. A lumbar puncture was performed which provided clear cerebrospinal fluid with no leukocytes detected. The MRI brain was repeated a week later, which demonstrated ongoing vasogenic oedema, with interval decrease in leptomeningeal enhancement and stable leptomeningeal hemosiderin deposits, with no frank SAH.
At this time, it was felt that there was limited premise in support of an infective, neoplastic, or traumatic cause for these symptoms, making an inflammatory cause the most likely etiology. Thereafter, rheumatology and otolaryngology consultations were sought, and subsequent vasculitis screen elicited a positive p-ANCA and an elevated proteinase-3 (PR-3) of 105 relative units/ml. On closer questioning the patient admitted to a 3-month history of dry crusting of his nose. He commenced on methylprednisolone IV for three days, before being commenced on prednisolone 60 mg PO initially (reducing slowly). The patient was then commenced on low dose oral Methotrexate (20 mg PO weekly) and IV Cyclophosphamide (Bermingham protocol). The MRI brain was repeated 1 month after treatment, which demonstrated the complete resolution of leptomeningeal thickening and a small focus of vasogenic edema (Figure 4), with a focal defect in the nasal septum, supporting a formal diagnosis of cerebral vasculitis secondary to GPA. At follow up review in clinic at 3 months the patient’s signs and symptoms had completely resolved. He remains well on Prednisolone 10 mg PO daily and Methotrexate 20 mg PO weekly.
Discussion
GPA is an ambiguous systemic autoimmune disease, which is associated with vasculitis of any small and medium sized blood vessels. The inconsistent systemic nature of the presentations and manifestations of GPA can result in atypical presentations and pose a diagnostic challenge to the clinicians. In the current case, an unusual neurological presentation rendered formal diagnosis of GPA challenging, which should be considered by the physician in future.
As described, CNS involvement in GPA is a rare entity. In their series, Nishino et al. reported that 109 out of 324 patients with diagnosed with GPA developed neurological symptoms, however, just 5 of these patients developed cerebritis (1.5%) [4]. Moreover, De Groot et al. reported that 9 out of 128 patients developed CNS symptoms (7.0%), while 112 were positive for c-ANCA (87.5%) and 3 for p-ANCA (2.3%), demonstrating the importance of p-ANCA in the current case [5]. Interestingly, PR3-ANCA is positive in 65- 75% of cases of GPA with upper respiratory tract involvement, making it more common in GPA compared to other types of ANCA-positive vasculitis [1]. Norman et al. previously reported a case of cerebritis secondary to GPA with presenting symptoms of confusion, ataxia and horizontal nystagmus. This patient underwent an MRI brain which showed symmetric parenchymal edema and leptomeningeal thickening, reasonably similar to the current case. The patient also had a history of joint pain, episcleritis, and intermittent epistaxis, with associated positivity for c-ANCA and PR3-ANCA [6]. Interestingly, the patient in this case did not have any of the aforementioned symptoms of systemic vasculitis other than paranasal sinus involvement, epistaxis and septal deviation.
There are several hypotheses suggested surrounding the pathophysiology of CNS involvement of GPA: Firstly, there is a perception that granulomatous inflammation of nearby structures (such as sinuses or meninges) cause local involvement of the cerebrum. Secondly, there is a notion that primary cerebral vasculitis induces local haemorrhage, subsequently leading to large volume SAH [7]. Importantly, cerebral vasculitis is even rarer than granulomatous causes of CNS involvement in GPA. Among the two phenotypes of CNS involvement (i.e.: granulomatous and vasculitic) seem to demonstrate obvious differences in their presentations, for example, the current case demonstrated a vasculitic type, where motor symptoms dominate, while granulomatous type exhibits more headaches and MPO-ANCA positivity, as previously described [8].
Although c-ANCA is mainly associated with PR3-ANCA and p-ANCA is mainly associated with MPO [1], our patient expressed positivity for both PR3-ANCA and p-ANCA. Nagashima et al. reported a case of p-ANCA positive GPA with pachymeningitis and listed 4 previous case reports with descriptions of a similar condition [9]. Interestingly, hypertrophic pachymeningitis is a more common radiological finding than leptomeningeal thickening in GPA [7]. Nevertheless, the most common clinical sign of meningeal involvement of GPA is headache, which was absent in the case of our patient. Similarly, Soriano et al. reported a case of a male patient who was c-ANCA positive GPA with sinus and meningeal involvement without headaches [10]. In addition, Dhanhani et al. reported a case of cerebral vasculitis secondary to GPA presenting with leptomeningitis and vasogenic edema with no granuloma present on biopsy and negative ANCA [11]. Moreover, Murphy et al. reported leptomeningeal thickening and enhancement on MRI in just 1 patient out of 19 patients diagnosed with GPA (5.3%) and postulated that vasculitis causing SAH was causative, due to likely endothelial damage [12]. Thus, this patient’s case adds further context to the plausibility of GPA with CNS involvement as an abstract differential for the patient presenting with atypical neurological symptoms and ambiguous radiological results.
In establishing a formal diagnosis of GPA, biopsy combined with ANCA-typing serves as the contemporary ‘gold standard’ [5]. Thereafter, combined imaging and laboratory investigations (i.e.: C-reactive protein, erythrocyte sediment rate, etc.) are utilised to rule out vasculitis mimics, such as infective, neoplastic, and other autoimmune diseases (including and not limited to systemic lupus erythematosus, rheumatoid arteritis and Behcet disease) [3]. As was the case for this patient, biopsy in setting of cerebral vasculitis is usually not a viable option on account of the involvement of small size vessels, rendering formal diagnosis even more challenging [7].
Importantly, there are several ‘red herrings’ adding to the clinical conundrum of this case. Firstly, this patient was presented to the ED after a mechanical fall with symptoms of upper limb weakness, confusion, and slurred speech which was consistent for longer than 24 hours. These symptoms correctly raised suspicion for Cerebrovascular Accident (CVA). Secondly, this patient reported a vague history of an initial fall 2 days prior, with similar symptoms and had self-medicated with aspirin, raising clinical suspicion for intracranial haemorrhage. Subsequently, a non-contrast CT brain was performed to out-rule both acute ischemic stroke and intracranial hemorrhage secondary to fall. Thirdly, a CT brain with contrast and MRI brain were performed given the suspicion of a primary, brain tumor, CNS lymphoma or metastatic disease, given the vasogenic oedema with associated non-specific leptomeningeal enhancement, as well as mucosal opacification of paranasal sinuses and septal deviation, suggestive of an underlying inflammatory process. Fourthly, after radiologically out-ruling infectious and neoplastic causes, this patient underwent review by otolaryngology due to the symptoms of intermittent nasal congestion and epistaxis. A vasculitis screening was performed by the rheumatology service, which showed positive p-ANCA, negative c-ANCA and positive anti-PR3 IgG raised at 105 RU/ml and negative anti-MPO IgG. The formal diagnosis of cerebral vasculitis secondary to GPA was confirmed before the patient commenced immunosuppression treatment.
Conclusion
Therefore, the take-home message from the current report is quite simple: While an unlikely working diagnosis, it is important for the clinician to consider CNS symptoms in isolation as a plausible manifestation of cerebral vasculitis secondary to underlying, undiagnosed GPA, particularly in the absence of obvious upper or lower respiratory tract symptoms or haemorrhage. In such instances, this may expedite earlier treatment of GPA with immunosuppressants, which may facilitate enhanced clinical outcomes, particularly when considering previous cases of GPA with meningeal involvement that has progressed to fatality due to delayed diagnoses [11,12]. Thus, this case reminds clinicians that GPA may have atypical initial presentations which are limited to the CNS in isolation and hopes to trigger clinical acumen which may facilitate earlier diagnoses of atypical GPA for prospective patients.
References
- Kitching AR, Anders HJ, Basu N, Brouwer E, Gordon J, et al. ANCA-associated vasculitis. Nat Rev Dis Primers. 2020; 6(1): 71.
- Travis WD. Common and uncommon manifestations of wegener’s granulomatosis. Cardiovascular Pathology. 1994; 3(3): 217-25.
- Zheng Y, Zhang Y, Cai M, Lai N, Chen Z, Ding M. Central Nervous System Involvement in ANCA-Associated Vasculitis: What Neurologists Need to Know. Front Neurol. 2019; 9: 1166.
- Nishino H, Rubino FA, DeRemee RA, Swanson JW, Parisi JE. Neurological involvement in Wegener’s granulomatosis: An analysis of 324 consecutive patients at the Mayo Clinic. Annals of Neurology. 1993; 33(1): 4-9.
- De Groot K, Schmidt DK, Arlt AC, Gross WL, Reinhold-Keller E. Standardized Neurologic Evaluations of 128 Patients with Wegener Granulomatosis. Arch Neurol. 2001; 58(8): 1215.
- Norman J, Pande I, Taylor T, Gran B. A Presentation of Cerebritis Secondary to Granulomatosis with Polyangiitis (Wegener). Case Reports in Neurological Medicine. 2014; 2014: 1-5.
- Holle JU, Gross WL. Neurological involvement in Wegener’s granulomatosis. Current Opinion in Rheumatology. 2011; 23(1): 7-11.
- De Luna G, Terrier B, Kaminsky P, Le Quellec A, Maurier F, et al. Central nervous system involvement of granulomatosis with polyangiitis: Clinical-radiological presentation distinguishes different outcomes. Rheumatology. 2015; 54(3): 424-32.
- Nagashima T, Maguchi S, Terayama Y, Horimoto M, Nemoto M, et al. P-ANCA-positive Wegener’s granulomatosis presenting with hypertrophic pachymeningitis and multiple cranial neuropathies: Case report and review of literature. Neuropathology. 2000; 20(1): 23-30.
- Soriano A, Vullo ML, Casale M, Quattrocchi CC, Afeltra A. Meningeal Involvement in Wegener Granulomatosis: Case Report and Review of the Literature. Int J Immunopathol Pharmacol. 2012; 25(4): 1137-41.
- Dhanhani AA, MacAULAY R, Maloney B, Hanly JG. Meningeal Involvement in Wegener’s Granulomatosis. The Journal of Rheumatology.
- Murphy JM, Gomez-Anson B, Gillard JH, Antoun NM, Cross J, Elliott JD, et al. Wegener Granulomatosis: MR Imaging Findings in Brain and Meninges. Radiology. 1999; 213(3): 794-9.
