
Open Access, Volume 10
Panenteritis after colectomy for ulcerative colitis: The first steroid-refractory case report treated with ustekinumab and a systematic literature review
Camilla Gallo1; Giovanni Perricone2*; Marta Stegagnini1; Tommaso Lorenzo Parigi3; Maria Costanza Aquilano4; Vincenzo Villanacci5; Marcello Vangeli2
1Department of Gastroenterology, Hepatology and Gastroenterology Unit, ASST Grande Ospedale Metropolitano Niguarda, Milan, Fondazione IRCCS San Gerardo dei Tintori, University of Milano-Bicocca School of Medicine, Monza, Italy.
2Hepatology and Gastroenterology Unit, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
3Faculty of Medicine, University Vita-Salute San Raffaele, Milan, Italy.
4Department of Hematology, Oncology and Molecular Medicine, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
5Institute of Pathology, ASST Spedali Civili, Brescia, Italy
Giovanni Perricone
Hepatology and Gastroenterology Unit, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
Email: giovanniperricone@gmail.com
Received : Mar 20, 2024,
Accepted : Apr 15, 2024
Published : Apr 19, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Idiopathic Post-Colectomy Pan-Enteritis (PCE) is a rare, often misdiagnosed and potentially life-threatening complication of colectomy for Ulcerative Colitis (UC), characterized by an early-onset diffuse, ulcerative mucosal inflammation, possibly involving the entire small bowel. Therapy is empirically based on corticosteroids and use of anti-TNF, azathioprine and cyclosporine has been reported for steroid-refractory cases. The need for revisional surgery is uncommon.
We present the first case of a severe steroid-refractory PCE successfully treated with Ustekinumab. It is the case of a 77-year-old man who underwent a subtotal colectomy with definitive ileostomy for severe steroid- and Infliximab (IFX)-refractory UC. Immediately after surgery, he developed a severe PCE with high ileostomy fecal output, severe dehydration, and life-threatening hydro-electrolyte imbalance. A new IV steroid course did not achieve any clinical response. Given the patient’s frailty, his recent history of multiple severe infections, and his previous anti-TNF alpha failure, we opted for a rescue therapy with Ustekinumab at standard 6 mg/kg induction and 8 weekly maintenance injections. No adverse events occurred. At fourmonths follow-up, a clinical, radiological, and endoscopic response was obtained.
We performed a systematic research in PubMed, Medline and Embase databases for English-written case reports and series of PCE, with specific focus on the adopted therapeutic strategies. Out of 25 total cases retrieved, 20 were treated with corticosteroids, 4 of which needed a rescue therapy with IFX or cyclosporine. In the remaining 5 cases, IFX or golimumab were preferred, mainly due to a previous history of steroidrefractory UC. Overall, 4 patients underwent revisional surgery to control symptoms, 3 of whom were in the first-line biologic therapy group.
In conclusion, this is the first report of ustekinumab’s safe and effective use for steroid-refractory PCE after colectomy for steroid- and IFX-refractory UC. Further research is required.
Keywords: Ulcerative colitis; Colectomy; Enteritis; Ustekinumab; Case report.
Core tip: Ulcerative colitis-related idiopathic Post-Colectomy Pan-Enteritis (PCE) is an infrequent, often unknown, life-threatening disease, characterized by diffuse, superficial, ulcerative mucosal inflammation of the small bowel. It should be suspected in case of early-after colectomy onset of intractable diarrhea and worsening anemia, but its definite diagnosis is histological. PCE normally responds to corticosteroids, and steroid-refractory cases have been treated with anti-TNF alpha or cyclosporine. We report the first steroidrefractory PCE case successfully treated with ustekinumab, a human anti-IL-12/IL-23 monoclonal antibody which modulates T lymphocyte-mediated immunity, in a fragile patient who underwent a subtotal colectomy with definitive ileostomy for severe steroid-refractory, infliximab non-responsive ulcerative colitis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Perricone G (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Gallo C, Perricone G, Stegagnini M, Parigi TL, Aquilano MC, Villanacci V, Vangeli M. Panenteritis after colectomy for ulcerative colitis: The first steroid-refractory case report treated with Ustekinumab and a systematic literature review. Open J Clin Med Case Rep. 2024; 2227.
Introduction
Ulcerative Colitis (UC) is a chronic inflammatory bowel disease usually characterized by superficial and diffuse inflammation limited to the colon and the rectum. Small bowel involvement in UC is sometimes seen in the terminal ileum in cases of active disease of the right colon, and it is called backwashed ilitis. After colectomy for UC, other possible affections of the small bowels are the pouchitis, the inflammation of the ileal pouch, or the pre-pouch enteritis, mainly confined within the first 50 cm of the ileum proximal to the pouch [1].
UC-related Post-Colectomy pan-Enteritis (PCE) is a very rare, idiopathic, distinct entity characterized by diffuse, superficial, ulcerative mucosal inflammation of the small bowel, with a typical onset shortly after colectomy for UC [2]. By definition, PCE can involve the entire post-colectomy residual small intestine, although cases of isolated involvement of the duodenum are rare [3].
To date, only a few dozen cases have been described. The pathogenesis of PCE is not completely known, but it is hypothesized that a massive T-cell (mainly CD4+ Th2 and CD8+) and cytokine-mediated inflammatory response may continue even after colectomy, with infiltration of the small bowel [4]. Additionally, post-surgical ischemia and changes in fecal stream after ileostomy may play a role [5]. PCE should be suspected in case of previous colectomy for UC, consistent symptoms, and continuous and superficial mucosal inflammation of extended tracts of small bowel at radiological imaging and endoscopy [6]. The presenting symptoms include nausea, vomiting, abdominal pain, and especially a high ileostomy output with subsequent dehydration, hypovolemia, and electrolytes disorders, which can be even fatal. PCE diagnosis requires the exclusion of other causes of pan-enteritis and the histological confirmation of presence of abundant lymphocytes intraepithelial infiltrate [4].
PCE represents a separate entity from High Output Syndrome (HOS) after ileostomy [7]; the latter, in fact, is the result of a usually transient and self-resolutive impairment in the mechanical and functional adaption mechanisms to water absorption reduction of the remaining gastrointestinal tract after colon-excluding stomas [8,9]. HOS is not sustained by an immune-mediated inflammation of the intestinal mucosa and, therefore, it does not require the use of immunomodulators, being usually treated with hydroelectrolyte and nutritional supportive therapies that are often not long-term [10].
Patients usually rapidly respond to Intravenous (IV) corticosteroids [3,11,12]. Azathioprine, tacrolimus, and anti-Tumor Necrosis Factor (TNF) alpha agents (mainly infliximab- IFX and golimumab) have been described as effective therapeutic options [2,13]. Nevertheless, available data regarding the therapeutic management of PCE are not yet sufficient to suggest solid clinical practice protocols, but considering the etiopathogenesis and chronicity of the disease, it is thought that long-term or even maintenance therapy is needed, as in cases of UC.
In this report, we describe the first case of a severe steroid-refractory PCE successfully treated with ustekinumab, an anti-IL-12/IL-23 monoclonal antibody, which modulates T lymphocyte-mediated immunity [14].
We prepared and revised the present manuscript according to a detailed reading of the CARE Checklist (2016).
Case Presentation
Chief complaints
In February 2022, a 77-year-old man was admitted to our Unit for severe acute UC.
History of present illness
He was diagnosed with ulcerative proctitis at the age of 72 (2018) and he was initially managed at another Center. From diagnosis to 2021, he had been on oral mesalazine at maintenance dose (2.4 gr daily) in stable clinical remission (1 or 2 bowel movements per day, with no visible blood nor urgency). In December 2021, the disease flared requiring admission in another Center; a colonoscopy observed extension of the disease to the whole colon. High-dose intravenous IV corticosteroids were started, with initial clinical response and consequent switch to oral corticosteroids, but in February 2022 he was referred to our Unit for disease relapse after steroid tapering. At referral, he reported the following symptoms: hematic diarrhea, abdominal pain, fecal urgency, tenesmus, severe sarcopenia, anemia, systemic inflammatory activation, and general malnutrition (BMI at referral 15,1 kg/m2 ). Baseline calprotectin at the admission was 6140 ug/g. Toxic megacolon was excluded through abdominal X-ray, and stool cultures, stool parasite assay and serologic tests were negative for infections. The Rectosigmoidoscopy (RSS) showed a Mayo 3 UC, with spontaneous bleeding mucosa and large ulcerations; biopsies were taken and CMV-related infection was excluded. Abdominal Computed Tomography (CT) scan showed diffuse wall thickening and tubulization of the colon and rectum; no involvement of small intestine was detected. High-dose IV methylprednisolone (40 mg/day) was started. Due to failure, after eight days, rescue therapy with IV IFX (5 mg/kg) was started. The patient received two infusions of IFX two weeks apart, during this time multiple severe intercurrent urinary tract infections occurred, complicated by bacteremias and sepsis requiring broad-spectrum antibiotic treatment (a 7-day course of piperacillin/tazobactam, two courses of about 8-10 days of vancomycin, an 8-day course of meropenem and a 5-day course of caspofungin). No improvement was observed after two administrations of IFX and after broad-spectrum antibiotic therapy, thusfore, after 40 days from the admission, the patient underwent a Videolaparoscopic (VLS) subtotal colectomy with definitive terminal ileostomy. Pathology examination of the surgical specimen highlighted a severe ulcerative pancolitis, with no involvement of the small intestine.
History of past illness
No particular comorbidities were reported in past illnesses history of the patient.
Personal and family history
The patient denied any family history of inflammatory bowel disease or other immune-mediated diseases.
Physical examination
The postoperative course was complicated by the persistence of abdominal pain and anorexia. At post-operative day 9, high fecal output from the ileostomy (>2000 mL/day) was reported, and discrasic declivous edemas and abdominal, pleural, and pericardial transudate progressively appeared, figuring a protein-losing enteropathy-like condition.
Laboratory examinations
Inflammatory indexes (leucocytes, C-reactive protein, and calprotectin) were persistently elevated. Severe hydro-electrolyte imbalance due to high fecal output and dehydration was highlighted and it could hardly be corrected with abundant IV supplementation. Nutritional values kept on worsening even after surgery. Renal and cardiac function test were stably normal.
Imaging examinations
Two weeks after surgery, contrast-enhanced CT scan, and subsequent Enterography Magnetic Resonance Imaging (E-MRI) showed a diffuse ileitis, extending for more than 1 meter from the ileostomy, with continuous hyperenhanced thickening of the mucosa and submucosa layers up to 6-7 mm, and several lymphadenopathies. An initial loss of the clear stratification of the intestinal wall, with a greater hyperechoic submucosal component was detected at intestinal ultrasound (Figure 1, panels A-C).
Further diagnostic work-up
Ileoscopy showed an ileitis extending to all the explored segments, more severe in the peri-stomal area, characterized by hyperemic mucosa with almost complete disappearance of the villi and various ulcers with fibrin bottom deposits (Figure 2, panel A). Pathology of ileal biopsies highlighted chronic active erosive inflammation of the mucosa, with a chronic lymphoplasmacytic and eosinophilic infiltrate limited to the lamina propria in all specimens.
Final diagnosis
The aforementioned findings were incompatible with Crohn’s disease, autoimmune enteropathy, or systemic vasculitis, but consistent with idiopathic PCE (Figure 3, panels A-B).
Multidisciplinary expert consultation and treatment
A therapeutic assay with IV metilprednisolone (1 mg/Kg/day) was started, with no clinical benefits. Given the patient’s frailty, the recent multiple severe infections, and his previous anti-TNF alpha failure, we opted for a rescue therapy with ustekinumab (6 mg/Kg).
Outcome and follow-up
Subsequently, a progressive improvement in terms of general clinical condition, fecal output, and nutritional status was observed in the 3-4 weeks following the first administration of Ustekinumab. Imaging showed a complete resolution of abdominal and pleural effusion, and the patient was thus discharged with a therapeutic maintenance strategy of Subcutaneous (SC) Ustekinumab (90 mg/8 weeks).
After about four months from the beginning of the treatment with Ustekinumab, an overall re-evaluation of the patient was performed. An almost complete disappearance of abdominal symptoms and an improvement in nutritional status with weight gain was noted. Regression of the systemic and bowel-specific inflammatory activation was revealed (last fecal calprotectin 204 ug/g).
Table 1 summarizes patient’s clinical and biochemical examinations through recent medical history.
E-MRI showed a significant improvement of the previous pan-enteritis (Figure 1, panel D). Endoscopy showed the persistency of solely erythematous patches and microulcerations limited to the distal ileal tract (Figure 2, panel B). A persistent moderate inflammatory infiltrate in the lamina propria and pseudoatrophy of the villi was highlighted at the pathological re-evaluation (Figure 3, panels C-D). Given the good response, maintenance treatment was continued with SC ustekinumab (90 mg/8 weeks).
Clinical, radiological, and endoscopic re-evaluation about 1 year after induction with ustekinumab confirmed disease remission.
Discussion
PCE is a relatively rare complication of colectomy for UC, generally represented by an early postcolectomy diffusion to the entire small bowel of the typical radiological, endoscopic, and histological characteristics of UC. It can be explained by the persistent activation of a massive T-cell and cytokine-mediated inflammatory response even after colectomy, which infiltrates the small bowel. Bacterial overgrowth and dysbiosis caused by altered fecal stream, together with post-surgical ischemia, and delayed morphological and functional adaptation of the small intestine after colectomy are other mechanisms involved in the complex etiopathogenesis of PCE [5].
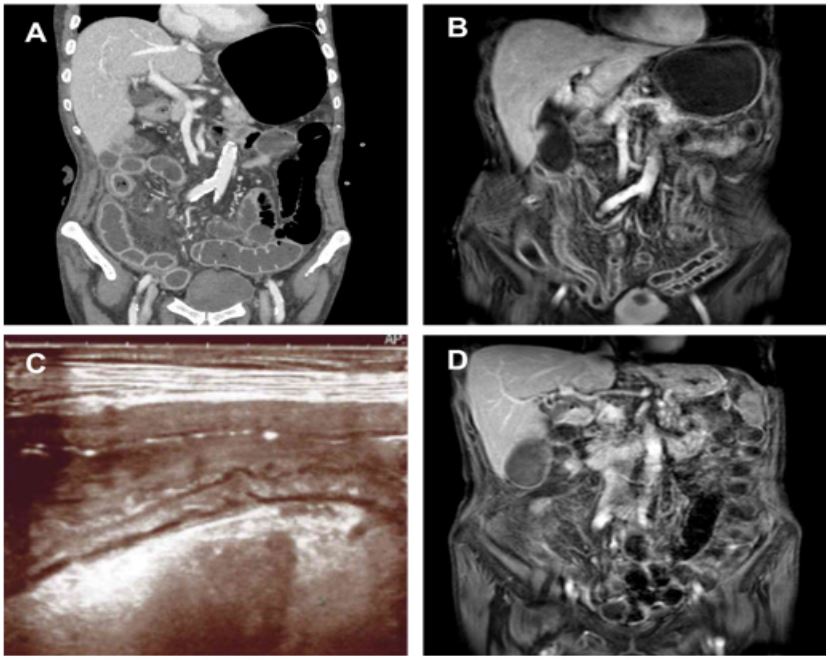
Figure 1: Panel A, B and C before ustekinumab, panel D after 2 administrations of ustekinumab. Thickening and hyperenhancement of the luminal layers and several lymphadenopathies in the arterial phase at the abdominal CE-CT scan (panel A). Thickening and hyperintensity of the small bowel walls in the THRIVE MRI sequences (panel B). Intestinal ultrasound
with evidence of greater representation of the hyperechoic submucosal layer and initial loss of the normal stratification of
the intestinal wall (panel C). Reduced thickening and intensity of the small bowel walls in the THRIVE MRI sequences (panel D). CE-CT: Contrast-Enhanced Computed Tomography scan; MRI: Magnetic Resonance Imaging.
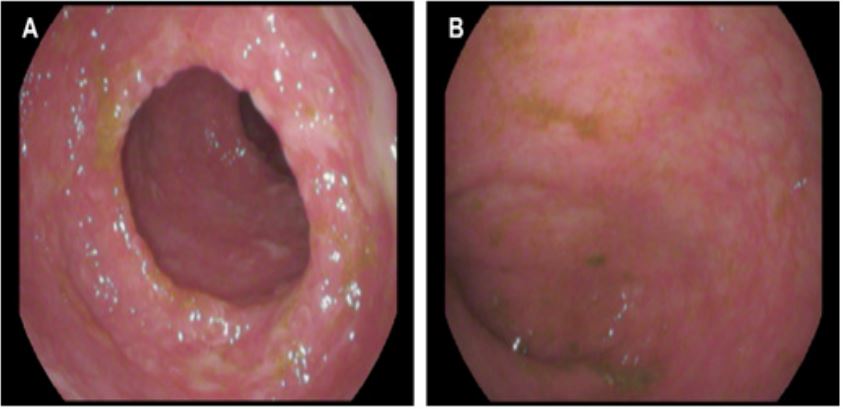
Figure 2: lIleoscopy with evidence, before ustekinumab, of hyperemic mucosa, almost complete disappearance of villi and
ulcers with fibrin bottom deposits, extended to all the explored segments (panel A). Residual erythematous patches and
microulcerations in a limited distal tract of the ileum at the endoscopic reassessment after 2 administrations of ustekinumab
(panel B).
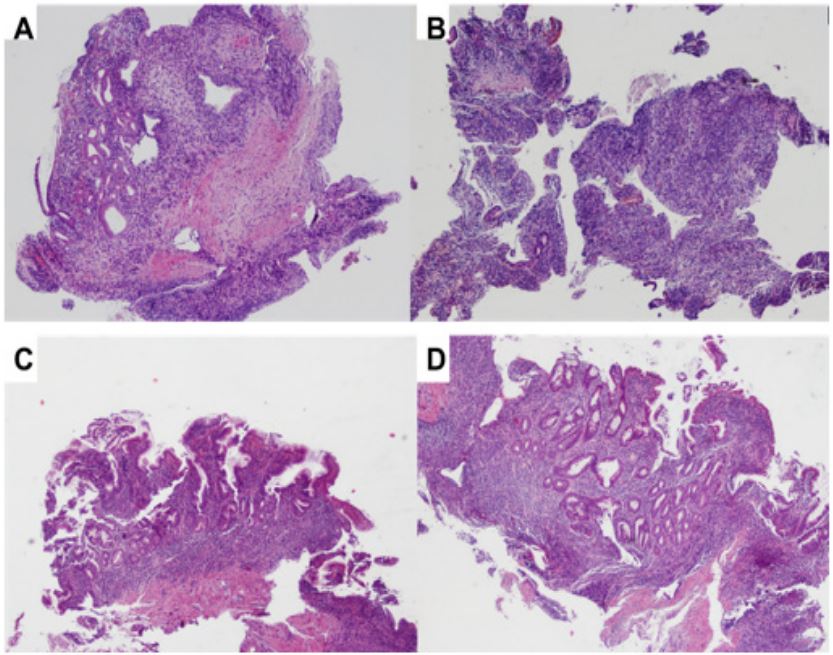
Figure 3: Diffuse Atrophy of the intestinal villi, hyperplastic crypts (panel A). Lamina propria with diffuse inflammation
(panel B) during the active phase of the enteritis. Persistent low-moderate atrophy of the intestinal villi (panel C) and inflammatory infiltrate of the lamina propria (panel D) at histological re-evaluation four months from the beginning of therapy
with Ustekinumab. H&Ex20. H&E: Hematoxylin and Eosin.
Table 1: Patient’s clinical and biochemical examinations through recent medical history.
| Before colectomy | Before ustekinumab | Four months after ustekinumab | |
|---|---|---|---|
| Abdominal pain | ++ | +++ | +/- |
| Faecal output | - | >2000 mL/die | ≈600 mL/die |
| Haemoglobin [14.0-18.0 g/dL] | 6.2 | 7.2 | 10.8 |
| Leucocytes [4.0-10.0 x 10^9/L] | 17.39 | 20.79 | 9.11 |
| Creatinine [0.67-1.17 mg/dL] | 1.44 | 1.62 | 1.16 |
| Albumin [4.02-4.76 g/dL] | 1.87 | 2.37 | 3.87 |
| Prealbumin [23-42 mg/dL] | 15 | 18 | 30 |
| Total IgG [700-1600 mg/dL] | 761 | 909 | 1465 |
| Gamma globulin [0.80-1.35 g/dL] | 0.64 | 0.67 | 1.43 |
| CRP [0.0-0.5 mg/dL] | 5.8 | 2 | 0.9 |
| Lactate [0.6-1.8 mmol/L] | 3.18 | 2.28 | 0.76 |
| Faecal calprotectin [<50 μg/g] | 6140 | 402 | 204 |
| CRP: C-Reactive Protein. | |||
Table 2: PubMed, Medline and Embase published cases of PCE.
| Sex |
Age at small bowel involvem ent |
UC Extension ¥ |
Type of surgery for UC |
Time of PCE onset after colectomy (weeks) |
Small intestine involvement extension |
Induction therapy |
Response to steroids |
Maintenance therapy |
Surgery |
Follow- up time (months) |
Outcome | Death for GI cause |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | 23 | E2 |
Total colectomy + IPAA + temporary ileostomy |
2 | Jejunum and ileum |
Prednisone (1 mg/Kg/day) → cyclosporine (1000 mg/day) |
No | None | No | 36 | Complete remission |
No |
| M | 61 | E3 |
Subtotal colectomy + temporary ileostomy (Hartman) |
4 | Pan-enteritis |
Prednisone (1 mg/Kg/day) |
Yes | None | No | 36 |
Two relapses (treated with oral steroids) |
No |
| F | 51 | E3 |
Total colectomy + IPAA |
16 | Pan-enteritis |
Methylpredni solone (0.5 mg/ Kg/day) |
Yes | AZA (50 mg/ day) |
Yes (ileostomy closure) |
19 | Complete remission |
No |
| M | 52 | E3 |
Total colectomy + IPAA + temporary ileostomy |
16 | Pan-enteritis |
Hydrocortis one (400 mg/day)→ prednisone (NM) |
Yes | AZA (250 mg/ day) |
No | 12 | Complete remission |
No |
| F | 29 | E2 |
Total colectomy + IPAA |
72 |
Stomach and duodenum |
Oral mesalazine 1500 mg/day |
NA |
Oral mesalazine 1500 mg/day |
No | NM | Complete remission |
No |
| M | 38 | E3 |
Total colectomy + IPAA + temporary ileostomy |
1 |
Duodenum, jejunum, ileum |
Methylpre dnisolone (1000 mg/day) |
Yes | AZA (NM) | No | 15 | Complete remission |
No |
| F | 30 | E3 |
Total colectomy + IPAA + temporary ileostomy |
28 (imme diately after ileostomy closure) |
Duodenum |
Methylpred nisolone (500 mg/day) |
Yes | None | No | 84 | Complete remission |
No |
| F | 9 | E3 |
Total colectomy + ERPT |
68 | Duodenum and ileum |
Cortico steroids (NM) |
Yes | None | No | 54 | Complete remission |
No |
| F | 20 | E3 |
Subtotal colectomy + ileostomy |
36 | Duodenum and ileum |
Cortic osteroids (NM) |
Yes |
Corticos teroids (NM) |
Yes (1st ERPT with loop ileostomy; 2nd ileostomy closure) |
12 | 2 pouchitis | No |
| F | 62 | E3 |
Partial proctoc olectomy + IPAA |
72 | Duodenum and ileum |
Corticosteroids, cyclosporine, and Azathioprine (NM) |
Yes | NM | No | 22 | Partial remission |
No |
| M | 17 | E3 |
Subtotal colectomy + temporary ileostomy (Hartman) |
1 | Duodenum and ileum |
Corticos teroids (NM) |
Yes | None | No | 19 | Partial remission |
No |
| M | 41 | E3 |
Subtotal colectomy + ileo-rectal anastomosis + temporary ileostomy |
4 | Pan-enteritis |
Methylprednis olone (1 mg/ kg/day) |
No | NA | No | <1 | Persistence | Yes |
| F | 23 | E3 |
Total colectomy + IPAA + temporary ileostomy |
12 | Pan-enteritis |
Methylpredni solone (40 mg/ day) |
Yes | AZA (3 mg/Kg/ day) |
No | 10 | Remission | No |
| F | 29 | E3 |
1st total colectomy + temporary ileostomy, 2nd IPAA and ileostomy takedown. |
12 | Pan-enteritis |
Methylpredni solone (40 mg day) |
Yes (steroid- dependent) |
Prednisone 20 mg/day + AZA (3 mg/Kg/day) →Prendisone 10 mg/day + certolizumab (NM) + MTX (NM) |
No | 57 |
Remission (steroid- dependent) |
No |
| M | 27 | E3 |
Total colectomy + IPAA |
1200 (25 years) |
Pan-enteritis |
Methylpredni solone (40 mg day) |
Yes | AZA (2 mg/Kg/ day) |
No | 43 | Remission | No |
| M | 57 | E3 |
Subtotal colectomy + definitive ileostomy |
96 (2 years) | Pan-enteritis |
Methylpredni solone (40 mg day) |
Yes |
AZA (2.2 mg/ Kg/day) |
No | 6 | Remission | No |
| F | 43 | E3 |
Total colectomy + definitive ileostomy |
12 | Pan-enteritis |
Methylpredni solone (40 mg day) |
Yes |
Tacrolimus (6 mg/day) |
No | 6 | Remission | No |
| M | 19 | E3 |
Total colectomy + IPAA + temporary ileostomy |
1 | Pan-enteritis |
Methylpredni solone (40 mg day) |
Yes |
IFX (5 mg/Kg/8 weeks) |
Yes (perforation suture) |
4 |
Remission (after 2nd surgery) |
No |
| F |
NM (around 20) |
E3 |
Total colectomy + IPAA + temporary ileostomy |
4 | Pan-enteritis |
Methylpredni solone (NM) |
Yes | IFX (NM) | No | 106 | Remission | No |
| F |
NM (around 60) |
E3 |
Total colectomy + IPAA + temporary ileostomy |
13 | Pan-enteritis | IFX (NM) | NA | IFX (NM) |
Yes (ileostomy closure) |
90 | Remission | No |
| M |
NM (around 40) |
E3 |
Total colectomy + IPAA + temporary ileostomy |
35 | Pan-enteritis |
Methylpredni solone (NM) |
No | IFX (NM) | No | 27 |
One relapse (pouchitis - treated with topic steroids) |
No |
| M |
NM (around 50) |
E3 + CRC |
Total colectomy + IPAA + temporary ileostomy |
2 | Jejunum and ileum |
GLM (NM) | NA | GLM (NM) |
Yes (ileostomy closure) |
12 | Remission | Yes (of CRC) |
| M |
NM (around 20) |
E3 |
Total colectomy + IPAA + temporary ileostomy |
5 | Pan-enteritis |
Methylpredni solone (NM) |
No | IFX (NM) | No | 15 | Remission | No |
| M | E3 |
Total colectomy + IPAA + temporary ileostomy |
5 | Pan-enteritis | GLM (NM) | NA | GLM (NM) | No | 4 | Remission | No | |
| M | E3 |
Total colectomy + temporary ileostomy (Hartman) |
2 | Pan-enteritis | IFX (NM) | NA | IFX (NM) |
Yes (ileostomy closure) |
4 | Remission | No |
UC: Ulcerative Colitis; PCE: Post-Colectomy Enteritis; GI: Gastrointestinal; IPAA: Ileal Pouch-Anal Anastomosis; NM: Not Mentioned; NA: Not Applicable; ERPT: Endorectal Pullthrough; AZA: Azathrioprine; MTX: Methotrexate; IFX: Infliximab; GLM: Golimumab; CRC: Colorectal Cancer. ¥ according to Montreal Classification
Our brief case report is focused on a patient who underwent subtotal colectomy with definitive terminal ileostomy for medical-refractory acute severe UC and who developed severe PCE immediately after colectomy
We performed a systematic research in PubMed, Medline and Embase databases for case reports and case series using the terms ‘ulcerative colitis’ and ‘post-colectomy enteritis’ or ‘pan-enteritis’, and evaluated those with an English written abstract available (Table 2). A total of 25 cases of definite PCE, without small intestine involvement before colectomy, were reported [2,3,11-20]. Regarding therapeutic strategies for PCE, 20 out of 25 cases were treated with corticosteroids as induction therapy, with good response in 15 of them; except an isolated case of fatal PCE, patients initially not responding to steroids reached remission with IFX or, in a single case, with cyclosporine. Among the other 5 reported cases of PCE, biological agents were mainly used as induction therapy (IFX for 2 cases, golimumab for other 2 cases). Four patients underwent revisional surgery, in particular ileostomy closure, to control PCE symptoms.
In our case report, no clinical response was noted after more than a week of high-dose IV corticosteroids. For multiple explained reasons, Ustekinumab was preferred over IFX, golimumab or cyclosporine as the rescue therapy alternative.
Ustekinumab is a human monoclonal antibody which binds to the p40 subunit common to IL-12 and IL-23 and prevents their interaction with the IL-12 receptor β1 subunit, thus modulating lymphocyte Th1 and Th17 function [14]. It is approved by Food and Drug Administration and European Medicine Agency as a 1st line biological therapy for moderate-to-severe UC and as a 2nd line biological therapy for CD after antiTNF alpha agents, but it has never been described as a therapeutic option for PCE so far. The safety profile of ustekinumab is reassuring and generally considered to be safer than anti-TNF agents, while the time to clinical response is similar to anti-TNF [21].
Conclusion
Ours is the first case of steroid-refractory PCE successfully treated with ustekinumab. Ustekinumab proved to be safe and effective in terms of clinical, radiological and endoscopic response after only four months. The effectiveness of this treatment regimen was confirmed at the one-year re-evaluation.
Additional research is required to improve the understanding of PCE and its pathogenesis. Further studies, possibly randomized controlled trials, with larger number of cases and longer follow-up time are needed to confirm the effectiveness of Ustekinumab for this condition.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Authors contributions: C.G. literature search, original draft writing, and radiological and endoscopic imaging editing; G.P. conceptualization, review, and manuscript editing; M.S. case report draft writing; T.L.P. review, and manuscript editing; M.C.A. pathological expert opinion and histological pictures editing; V.V. pathological expert opinion and manuscript editing; M.V. conceptualization, supervision, and expert opinion.
Acknowledgements: None.
Funding: None.
Conflict of interest statement: The authors declare that they have no conflict of interest to disclose.
Availability of data and materials: Data and materials are available for any consultation and re-evaluation.
Consent to treatment: Informed written consent was obtained from the patient whose case has been here reported for the treatment he underwent to.
References
- Haboubi N. Small bowel inflammation in ulcerative colitis. Colorectal Dis Off J Assoc Coloproctology G B Irel. 2006; 8: 373-374.
- Gooding IR, Springall R, Talbot IC, et al. Idiopathic small-intestinal inflammation after colectomy for ulcerative colitis. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2008; 6: 707-709.
- Terashima S, Hoshino Y, Kanzaki N, et al. Ulcerative duodenitis accompanying ulcerative colitis. J Clin Gastroenterol. 2001; 32: 172-175.
- Vidali F, Di Sabatino A, Broglia F, et al. Increased CD8+ intraepithelial lymphocyte infiltration and reduced surface area to volume ratio in the duodenum of patients with ulcerative colitis. Scand J Gastroenterol. 2010; 45: 684-689.
- Willis S, Kisielinski K, Klosterhalfen B, et al. Morphological and functional adaptation of the small intestine after colectomy and ileal pouch-anal anastomosis in rats. Int J Colorectal Dis. 2002; 17: 85-91.
- Erden A, Kuru Öz D, Gürsoy Çoruh A, et al. Backwash ileitis in ulcerative colitis: Are there MR enterographic features that distinguish it from Crohn disease? Eur J Radiol 2019; 110: 212-218.
- Tsujinaka S, Suzuki H, Miura T, et al. Obstructive and secretory complications of diverting ileostomy. World J Gastroenterol. 2022; 28: 6732-6742.
- Assaf D, Hazzan D, Ben-Yaacov A, et al. Predisposing factors for high output stoma in patients with a diverting loop ileostomy after colorectal surgeries. Ann Coloproctology. 2023; 39: 168-174.
- Seifarth C, Augustin LN, Lehmann KS, et al. Assessment of Risk Factors for the Occurrence of a High-Output Ileostomy. Front Surg. 2021; 8: 642288.
- Mountford CG, Manas DM, Thompson NP. A practical approach to the management of high-output stoma. Frontline Gastroenterol. 2014; 5: 203-207.
- Hoentjen F, Hanauer SB, Hart J, et al. Long-term treatment of patients with a history of ulcerative colitis who develop gastritis and pan-enteritis after colectomy. J Clin Gastroenterol. 2013; 47: 52-57.
- Corporaal S, Karrenbeld A, van der Linde K, et al. Diffuse enteritis after colectomy for ulcerative colitis: two case reports and review of the literature. Eur J Gastroenterol Hepatol. 2009; 21: 710-715.
- Rush B, Berger L, Rosenfeld G, et al. Tacrolimus Therapy for Ulcerative Colitis-Associated Post-Colectomy Enteritis. ACG Case Rep J. 2014; 2: 33-35.
- Benson JM, Peritt D, Scallon BJ, et al. Discovery and mechanism of Ustekinumab: A human monoclonal antibody targeting interleukin-12 and interleukin-23 for treatment of immune-mediated disorders. MAbs. 2011; 3: 535-545.
- Valdez R, Appelman HD, Bronner MP, et al. Diffuse duodenitis associated with ulcerative colitis. Am J Surg Pathol. 2000; 24: 1407-1413.
- Yang Y, Liu Y, Zheng W, et al. A literature review and case report of severe and refractory post-colectomy enteritis. BMC Gastroenterol. 2019; 19: 61.
- Ikeuchi H, Hori K, Nishigami T, et al. Diffuse gastroduodenitis and pouchitis associated with ulcerative colitis. World J Gastroenterol. 2006; 12: 5913-5915.
- Rubenstein J, Sherif A, Appelman H, et al. Ulcerative colitis associated enteritis: is ulcerative colitis always confined to the colon? J Clin Gastroenterol. 2004; 38: 46-51.
- Annese V, Caruso N, Bisceglia M, et al. Fatal ulcerative panenteritis following colectomy in a patient with ulcerative colitis. Dig Dis Sci. 1999; 44: 1189-1195.
- Uchino M, Ikeuchi H, Bando T, et al. Diffuse gastroduodenitis and enteritis associated with ulcerative colitis and concomitant cytomegalovirus reactivation after total colectomy: Report of a case. Surg Today. 2013; 43: 321-324.
- Sandborn WJ, Feagan BG, Danese S, et al. Safety of Ustekinumab in Inflammatory Bowel Disease: Pooled Safety Analysis of Results from Phase 2/3 Studies. Inflamm Bowel Dis. 2021; 27: 994-1007.
