
Open Access, Volume 10
Case Report: Thigh hidradenoma masquerading as lipoma
Abdullah Alhaqbani*; Homoud Alawfi; Firas Alahmadatea; Sami Almalki
General Surgery Department, King Abdulaziz Medical City, Riyadh, Saudi Arabia.
Abdullah Alhaqbani
General Surgery Department, King Abdulaziz Medical City, Riyadh, Saudi Arabia.
Email: Al78bani@gmail.com
Received : Mar 07, 2024,
Accepted : Apr 10, 2024
Published : Apr 19, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Background: Hidradenomas are benign adnexal neoplasms which were recently been subdivided into two groups: eccrine differentiation (poroid hidradenomas) or apocrine differentiation (clear cell hidradenomas) with the latter being rarer. These types of tumors have been associated with recurrence and malignant transformation, however; recurrence and malignancy are considered very rare. We present a case report of a 35-year-old male who presented with two lumps, clinically representing simple lipomas but one of them turned to be a hidradenoma.
Case presentation: A 35-year-old gentleman not known to have any medical illnesses and surgically free, presented to our general surgery clinic complaining of two slow-growing (over three years) painless lumps, one in the right upper thigh and the other one in the left shoulder. The patient denied any previous history of trauma or infection nor any history of discharge or overlying skin changes, and there were no clinical features that might suggest the presence of malignancy. Upon examination, both lumps were firm, freely mobile, non-tender, intact overlying skin, with no skin changes, and no regional lymphadenopathy. Prior to Excision, our preliminary impression was lipoma for both masses. Surgical excision was carried out with clear margins; each mass was labeled separately, and specimens were sent for histopathology. Histopathological diagnosis of the left shoulder mass was consistent with lipoma, however; the right upper thigh mass turned to be a hidradenoma.
Conclusion: Hidradenomas are uncommon benign neoplasms with varied types. Recurrence and transformation into malignancy have been reported in some cases. Complete surgical excision with negative margins, and further follow up with the patient is crucial to prevent such consequences. Clinical diagnosis can be difficult, however; the management is the same with surgical removal as it will give us the definitive diagnosis with the pathology report.
Keywords: General surgery; Lipoma; Hidradenoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Alhaqbani A (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Alhaqbani A, Alawfi H, Alahmadatea F, Almalki S. Case Report: Thigh hidradenoma masquerading as lipoma. Open J Clin Med Case Rep. 2024; 2225.
Background
Hidradenomas are benign adnexal neoplasms which were recently been subdivided into two groups: eccrine differentiation (poroid hidradenomas) or apocrine differentiation (clear cell hidradenomas) with the latter being rarer [1]. These tumors are considered relatively rare, and they are commonly found in adults, rarely in children, with most cases affecting females more than males [2].
The affected region is usually head and neck, trunk, and extremities, presenting as a firm dermal nodule spanning between 3-30 mm in size, and they grow slowly with occasional overlying skin changes [3,2]. These types of tumors have been associated with recurrence and malignant transformation, however; recurrence and malignancy are considered very rare.
We present a case report of a 35-year-old male who presented with two lumps, clinically representing simple lipomas but one of them turned to be a hidradenoma.
Case Presentation
A 35-year-old gentleman not known to have any medical illnesses and surgically free, presented to our general surgery clinic complaining of two slow-growing (over three years) painless lumps, one in the right upper thigh and the other one in the left shoulder. The patient denied any previous history of trauma or infection nor any history of discharge or overlying skin changes, and there were no clinical features that might suggest the presence of malignancy.
Upon examination, both lumps were firm, freely mobile, non-tender, intact overlying skin, with no skin changes, and no regional lymphadenopathy. Prior to Excision, our preliminary impression was lipoma for both masses. Surgical excision was carried out with clear margins; each mass was labeled separately, and specimens were sent for histopathology.
Histopathological diagnosis of the left shoulder mass was consistent with lipoma, however; the right upper thigh mass turned to be a hidradenoma (Figure 1).
Pathology report
1. The first specimen represents the upper thigh lesion consisting of brown tan soft tissue measuring 1.4 x 0.9 x 0.5 cm consistent with hidradenoma.
2. The second specimen represents the shoulder lesion on the left side, morphologically demonstrating a homogenous fibrofatty soft tissue measuring 5.6 x 3.4 x 1.5 cm consistent with lipoma.
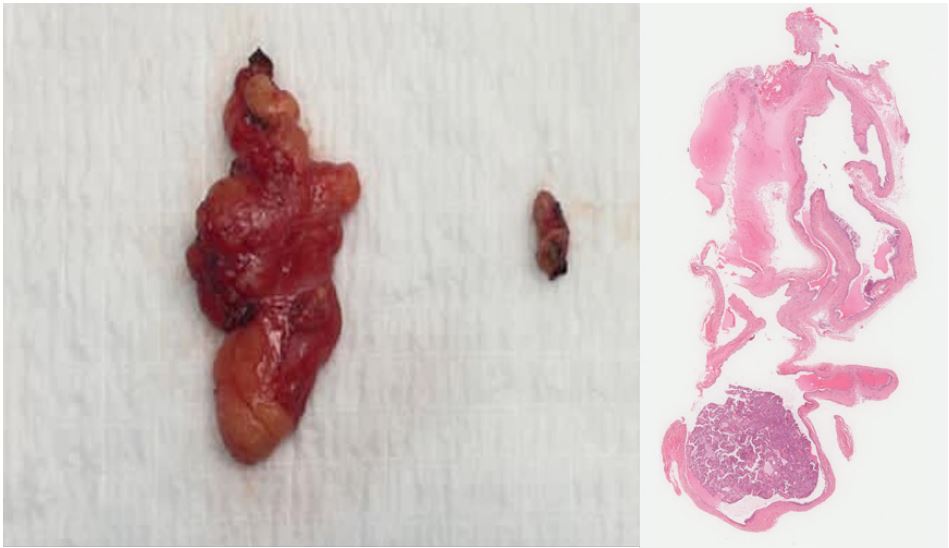
Figure 1: The two masses after surgical excision, along with microscopic slide.
Discussion
Hidradenomas are considered a rare benign adnexal neoplasm of uncertain origin [1]. Most traditionally subdivided into either eccrine (more common) or apocrine (rare) derivation [4]. It commonly affect females more than males, and they usually present in head, neck, and extremities with a size range of 3-30 mm [2,3]. Usually overlying skin is intact upon presentation, but ulceration and discharge (serous) have been described before [4]. The pace of growing is slow, however; rapid growth could represent trauma or malignant changes [4]. Although benign, the malignant transformation has been reported, and it is also associated with recurrence [5,6]. Tumors that are attached to the skin can sometimes be diagnosed clinically, especially if associated with other symptoms like history or serous discharge, on the other hand, ulcerated lesions may raise the suspicion of basal cell carcinoma [6].
In our case report, hidradenoma presented with a clinical picture of lipoma, especially with two lumps which is common in cases of lipoma to present in any part of the body and multiple lipomas can present at the same time. The management in our case was the same, which was surgical excision, and as a routine of any mass without a prior diagnosis, surgical margins were taken to ensure complete resection. Negative margins were ensured with the histopathology report, and further follow up was initiated with the patient to ensure elimination of any recurrence.
As there have been reported cases of recurrence of hidradenoma, monitoring and follow up are necessary to ensure full elimination. The importance of full resection of any mass has been displayed in our case report as without a prior pathology, taking extra precaution is important.
Clinical diagnosis can be difficult in such cases, as the mass was clinically presenting as a lipoma, however; ensuring proper treatment is the key to the management.
Conclusion
Hidradenomas are uncommon benign neoplasms with varied types. Recurrence and transformation into malignancy have reported in some cases. Complete surgical excision with negative margins, and further follow up with the patient is crucial to prevent such consequences. Clinical diagnosis can be difficult, however; the management is the same with surgical removal as it will give us the definitive diagnosis with the pathology report.
Declarations
Ethical approval and consent to participate: The study was approved by the Institutional Review Board at King Abdullah International Medical Research Centre, reference number RYD-23-419812-181006.
Availability of data and materials: All data generated or analyzed during this study are included in this published article and its supplementary information files.
Competing of interest: The authors have no conflict of interest to declare.
Authors’ contributions: Dr. Abdullah Alhaqbani: Data curation, investigation, validation, writing and editing final draft. Dr. Homoud Alawfi: conceptualization, supervision, validation Dr. Firas Alahmadatea: data curation, supervision Dr. Sami Almalki: conceptulalization, project administration, supervision, reviewing final draft.
Acknowledgments: Special thanks to Dr. Ali Assiri, consultant pathology in King Abdulaziz Medical City for providing us with the pathology slides.
References
- Gianotti R, Alessi E. Clear cell hidradenoma associated with the folliculo-sebaceous-apocrine unit: histologic study of five cases. The American journal of dermatopathology. 1997; 19(4): 351-7.
- Shahmoradi Z, Mokhtari F. Clear cell hidradenoma. Advanced Biomedical Research. 2013; 2.
- Bijou W, Laababsi R, Oukessou Y, Rouadi S, Abada R, et al. An unusual presentation of a nodular hidradenoma: A case report and review of the literature. Annals of Medicine and Surgery. 2021; 61: 61-3.
- Nandeesh BN, Rajalakshmi T. A study of histopathologic spectrum of nodular hidradenoma. The American Journal of Dermatopathology. 2012; 34(5): 461-70.
- Will R, Coldiron B. Recurrent clear cell hidradenoma of the foot. Dermatologic surgery. 2000; 26(7): 685-6.
- Keasbey LE, Hadley GG. Clear‐cell hidradenoma. Report of three cases with widespread metastases. Cancer. 1954; 7(5): 934-52.
