
Open Access, Volume 10
Treatment of giant diaphragmatic hernia in adults with transabdominal hernia ring orthopedic suture and continuous negative pressure suction of hernia sac cavity
Qin Xia; Mingtao Chang; Qiaozhi Feng; Chen Jianfa*
Department of General Surgery, The First Navy Hospital of Southern Theater Command, Zhanjiang 524009, China.
Chen Jianfa
Department of General Surgery, The First Navy Hospital of Southern Theater Command, Zhanjiang 524009,
China.
Email: 18573673658@163.com
Received : Mar 05, 2024,
Accepted : Apr 05, 2024
Published : Apr 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Background and objective: Although diaphragmatic hernia in adults is rare, its acute attack may be lifethreatening. By far, there are few clinical management guidelines and expert consensus for this disease. Because the application of mesh may still lead to infection and other complications or even hernia recurrence, the surgical methods remains controversial. For better efficacy and safety of the treatment of giant diaphragmatic hernia in adults, a new surgical procedure is investigated.
Methods: The clinical data of 5 adult patients with huge diaphragmatic hernia who underwent hernia ring orthopedic suture and continuous negative pressure suction were retrospectively analyzed. The postoperative hernia recurrence rate, average operation time, average hospital stay, and complications were recorded.
Results: All 5 operations were successfully completed without a combined thoracotomy approach. The average operation time was 155±10.8 min, the average hospitalization time was 7.7±1.2 d, and the average intraoperative blood loss was 65±12.8 ml. There was no injury to the internal organs and blood vessels of hernia, no injury to the heart and lung, no hernia sac rupture or resection. Moreover, there was no wound infection, bleeding, chronic pain, atelectasis and other postoperative complications. All patients were followed up for 6 to 12 months, and no recurrence of hernia was found.
Conclusion: The results of the current study revealed that transabdominal hernia ring orthopedic suture and continuous negative pressure suction of hernia sac cavity is a safe and effective method for the treatment of giant diaphragmatic hernia in adults.
Keywords: Hernia ring orthopedic suture; Hernia sac cavity; Continuous negative pressure suction; Adult giant diaphragmatic hernia.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Jianfa C (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Xia Q, Chang M, Feng Q, Jianfa C. Treatment of giant diaphragmatic hernia in adults with transabdominal hernia ring orthopedic suture and continuous negative pressure suction of hernia sac cavity. Open J Clin Med Case Rep. 2024; 2222.
Introduction
The protrusion of abdominal contents into the thoracic cavity through the diaphragmatic defect is called diaphragmatic hernia. It can be divided into: 1. Congenital Diaphragmatic Hernia (CDH) caused by diaphragmatic hypoplasia or congenital defect, is more common in neonates; 2. Secondary diaphragmatic hernia caused by trauma, surgery or other reasons, is more common in adults. Acute diaphragmatic hernia necessitates immediate intervention because it can lead to incarceration, perforation, or strangulation of abdominal organs, and herniated abdominal contents into the thorax which can compress the heart and lungs and cause respiratory failure or cardiac tamponade [1]. Surgery is the only cure for diaphragmatic hernia, but there is still controversy about the optimal timing of surgery, surgical approach, hernia repair method, and application of mesh [2]. There is no «gold standard» surgical method for diaphragmatic hernia, and postoperative complications such as infection, bleeding, intestinal obstruction, atelectasis, chronic pain may occur, and there is a certain recurrence rate. Due to the rarity of diaphragmatic hernia in adults, there is no clinical management guidelines for this disease at home and abroad, and most of the data are from single-center retrospective studies. For the first time, this study proposes a new surgical approach: transabdominal hernia ring orthopedic suture and continuous negative pressure suction of hernia sac cavity. From January 2022 to June 2023, a total of 5 cases of adult giant diaphragmatic hernia were treated with this approach, with satisfactory results, fewer postoperative complications, and no hernia recurrence.
Data and Methods
Case information: A retrospective analysis was performed on adult patients with giant diaphragmatic hernia who underwent transabdominal hernia ring orthopedic suture and continuous negative pressure suction of hernia sac cavity in our hospital from January 2022 to June 2023. Inclusion criteria: patients with giant congenital or secondary diaphragmatic hernia caused by trauma with diaphragmatic defect ≥5 cm were initially diagnosed by X-ray or thoracoabdominal CT. Exclusion criteria: (1) patients with hiatal hernia; (2) patients with severe dysfunction of heart, lung, liver and kidney; (3) severe coagulation dysfunction; (4) recurrent diaphragmatic hernia. The data collected included patient demographic information (age, gender), clinical symptoms, preoperative evaluation, surgical details, postoperative Intensive Care Unit (ICU) length of stay, total length of hospital stay, and postoperative follow-up results. A total of 5 patients were enrolled, including 4 (80%) males and 1 (20%) female, with an average age of 27.8±15.5 years. All patients had a primary diagnosis of giant diaphragmatic hernia. All diaphragmatic hernia were located on the left side. Informed consent was obtained from the patients and their families, and the protocol was approved by the ethics committee of the First Navy Hospital of Southern Theater Command.
Surgical methods: Gastrointestinal decompression should be performed in time for patients with preoperative intestinal obstruction. Preoperative fasting and fluid replacement were routine. Patients with abdominal or pulmonary infection were treated with antibiotics before operation. All operations were performed under general anesthesia with tracheal intubation and supine position.
The procedure was as follows: (1) an oblique incision under the left costal margin was made, starting from the xiphoid process and ending at the anterior axillary line; (2) Layer by layer into the abdomen the abdominal organs herniated into the thoracic cavity from the left diaphragmatic defect were found by exploration (Figure 1a). (3) The adhesion between the diaphragm and the abdominal viscera was bluntly separated until the hiatus of the hernia was exposed, and the herniated viscera were returned to the abdominal cavity through the hiatus (Figure 1b); (4) After the contents of the hernia were returned, a huge round hole (diameter ≥5 cm) was found in the left diaphragmatic muscle in the lumbocostal triangle, and the hernia sac protruded into the thoracic cavity (Figure 1c) (5) Hernia ring orthopedic suture: Due to the large diameter and circular shape of the hiatus, it was impossible to suture directly, so the diaphragm was cut open for about 5 cm at the 11 o ‘clock position of the hiatus, making the circular hiatus of the diaphragm into an oval shape (Figure 1d). From the left side to the right side, the diaphragmatic hiatus was sutured intermittently with 10-gauge thick silk suture (spacing 1cm, edge distance 1 cm) (Figure 1e). (6) The lung was reexpanded by continuous negative pressure suction of the hernia sac: a 20F negative pressure drainage tube was placed into the hernia sac in the thoracic cavity through the interrupted suture gap of the diaphragmatic hiatus (Figure 1f), which was extracted and fixed from the left lower abdominal wall. The left lung compressed by the hernia contents was gradually reexpanded by continuous negative pressure suction ball. After complete hemostasis and checking the instrument gauze, the abdomen was closed layer by layer.
The gastric tube was removed on the third postoperative day. The negative pressure drainage tube was removed 1 week after the operation when the CT showed that the lung had been fully dilated.
Observation indicators: The primary outcome was the recurrence rate of diaphragmatic hernia within 1 year after surgery. The secondary outcomes included operation time, length of stay in ICU, length of hospital stay, and surgery-related complications. During the follow-up period, each patient underwent thoracoabdominal CT to monitor the recurrence of diaphragmatic hernia and postoperative complications.
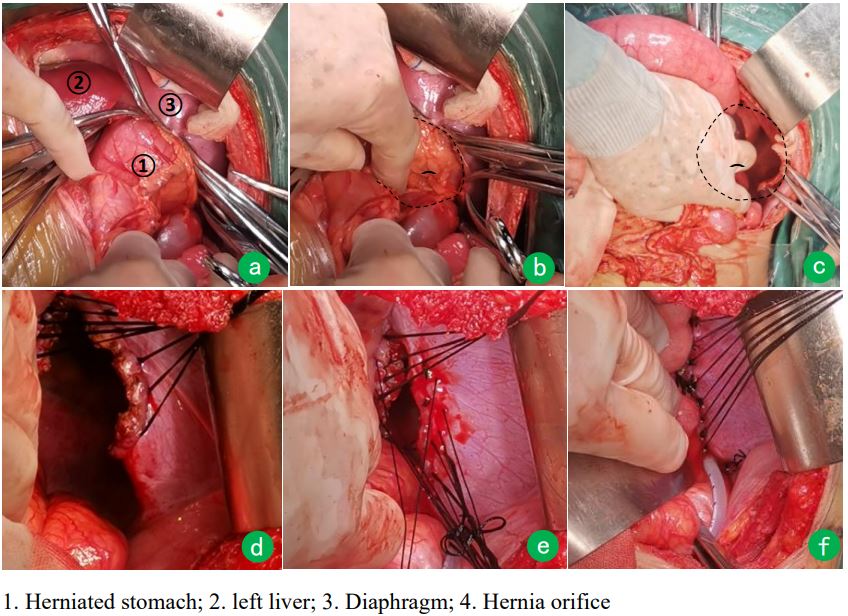
Figure 1: Surgical procedure of transabdominal hernia ring orthopedic suture and continuous negative pressure suction of
hernia sac cavity.
Results
Preoperative evaluation: A total of 5 patients were included in the study, including 4 (80%) males and 1 (20%) female, with an average age of 27.8±15.5 years. There were 1 case of CDH, 1 case of acute Traumatic Diaphragmatic Hernia (TDH), and 3 cases of chronic TDH, all of which were secondary to blunt impact injury. The main symptoms of CDH and chronic TDH were dyspnea, chronic abdominal pain, nausea and vomiting. However, one case of acute TDH presented with sudden severe abdominal pain, abdominal distension, vomiting, and sudden cardiac and respiratory arrest 2 hours after abdominal pain. Respiratory failure caused by acute left diaphragmatic hernia compression of the heart and lung was considered, immediate bedside rescue, fluid resuscitation, tracheal intubation, and ventilator-assisted breathing were performed to restore the patient’s heartbeat and breathing.
All patients underwent chest and abdominal CT examination before operation. Figure 2 shows the preoperative CT images of one patient with chronic TDH (Case 1) and one patient with acute TDH (Case 2).
Surgical situation: All operations were successfully completed without combined thoracotomy or laparoscopic or thoracoscopic approaches. The mean operative time was 155±10.8 min (range, 120-180 min). The mean ICU stay time was 2.4±0.7 days (range, 2-4 days). The mean hospital stay was 7.7±1.2 days (range, 6-9 days). The mean intraoperative blood loss was 65±12.8 ml. There was no injury of stomach, spleen, small intestine and mesentery vessels, no injury of heart, lung, great vessels, phrenic nerve, and no hernia sac breakage or resection. One patient developed paralytic intestinal obstruction and abdominal distension after operation, and the symptoms were significantly improved after the application of gastrointestinal motility drugs and more ambulation. All patients had no postoperative complications such as incision infection, bleeding in the surgical area, and pulmonary infection.
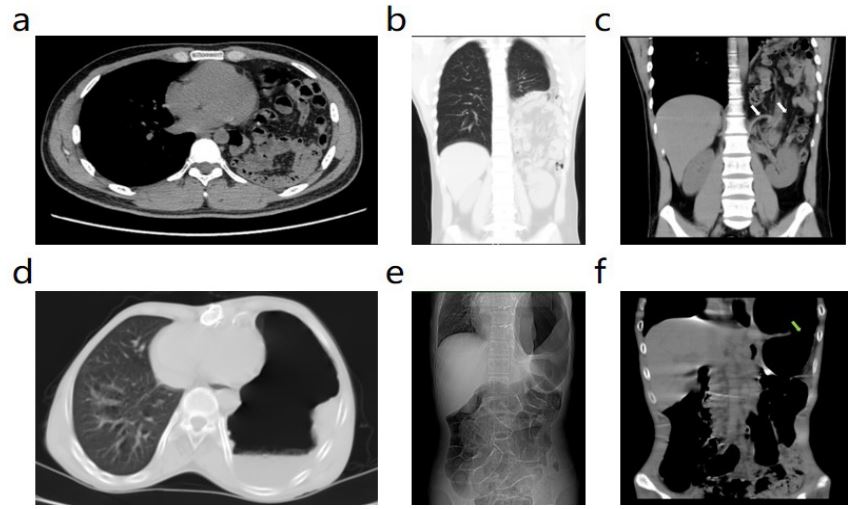
Figure 2: Preoperative CT findings in patients with diaphragmatic hernia. (a-c) In Case 1, part of the small intestine, transverse colon, and mesentery vessels herniated into the left thoracic cavity and compressed the left lung. The white arrow
showed displacement of the left diaphragmatic crus and a huge diaphragmatic defect. (d-f) In Case 2, most of the gastric
cavity herniated into the left thoracic cavity; Part of the intestinal tube in the abdominal cavity was obviously dilated and
pneumatoid, which was considered as intestinal obstruction. The green arrow showed the hernia tight rib gastric body.
Postoperative follow-up: The patients were followed up for 6-12 months, with an average of 8.5 months. During the follow-up period, no recurrence of diaphragmatic hernia was found by chest and abdominal CT (Figure 3), and no chronic postoperative pain, intestinal adhesion, or pulmonary atelectasis occurred.
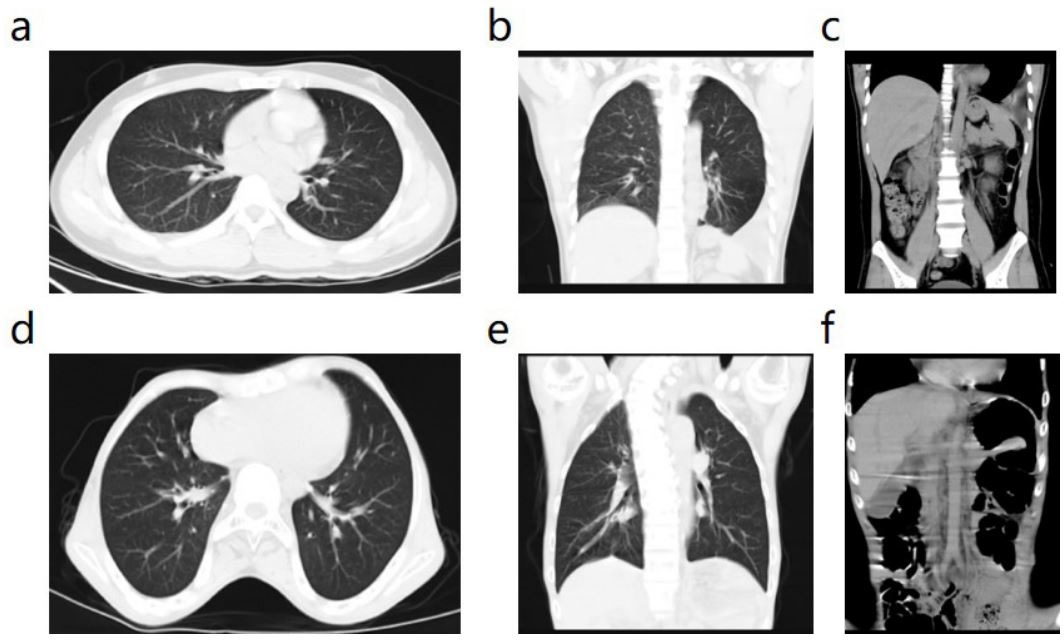
Figure 3: Postoperative follow-up CT findings in patients with diaphragmatic hernia. (a-c) Follow-up CT of Case 1 1 month
after surgery showed good lung recruitment and no recurrence of diaphragmatic hernia. (d-f) The follow-up CT of Case 2 at
6 months after operation showed that the left lung was fully re-expanded, and there was no diaphragmatic defect or recurrence
Discussion
The diaphragm is formed by the fusion of the septum transversum, pleuroperitoneal membranes, dorsal mesentery of the esophagus, and the body wall musculature [3]. The central part of the diaphragm is the central tendon, and the peripheral part is the muscle fiber. Divided into sternum, ribs, and waist based on the different starting points of muscle fibers. There is an absence of muscle fibers between the starting points of each part, which often constructs intermuscular cleft, including the sternocostal triangle and the lumbocostal triangle, covered only by diaphragmatic fascia and pleura peritoneum, which is the weak area of the diaphragm. Abdominal organs may enter the thoracic cavity through the deltoid process to form diaphragmatic hernia. CDH is rare in adults and usually occurs on the left side of the diaphragm (80%), and it is mainly caused by congenital thoracoabdominal hiatal hernia (Bochdalek hernia, embryonic abnormal development of the lumbocostal triangle) and congenital parasternal hernia (Morgagni hernia, embryonic abnormal development of the sternocostal triangle) [1]. More than 90% of cases, TDH is caused by blunt impact or penetrating injury to the chest and abdomen and occurs on the left side, but the right diaphragm is usually protected by the liver and the incidence of TDH is low [4]. Most TDH has been reported to occur posterolateral to the diaphragm due to its relative weakness [5].
The key to diaphragmatic hernia surgery is the restatement of hernia contents and the closure of the hernia ring [6]. Compared with the thoracic approach, the abdominal approach enables exploration of the entire abdominal cavity and timely detection of complications such as rupture and perforation of the gastrointestinal tract, strangulation necrosis, and splenic pedicle laceration and bleeding caused by hernia entrapment [7]. Due to less postoperative pain and lower incidence of incision complications, most studies favor laparoscopic surgery in hemodynamically stable patients who are amenable to elective surgery [4,8-9]. However, for patients with hemodynamic instability, respiratory instability, acute obstruction or strangulation, open surgery is still the main method. At the same time, patients with CDH or chronic TDH with a longer course of disease are likely to have extensive and tight adhesion between the diaphragm and herniated organs, making it difficult to restate the organs under laparoscopy, and gastrointestinal injury or bleeding may occur [10]. In this study, 1 patient with CDH and 3 patients with chronic TDH were found to have obvious adhesion between the diaphragm and herniated organs during the operation. To fully separate the adhesion between the viscera and the upper part of the diaphragm, which could not be accomplished by laparoscopic surgery, the surgeons needed to extend the finger into the thoracic cavity along the circumference of the herniated viscera through the hernia fissure.
In terms of the closure of the hernia ring, many studies have suggested that the diameter of the hernia ring less than 5 cm can be primary sutured. When the ring is 5-10 cm in diameter and the tension of direct closure is too great, a biologic mesh is recommended because of its greater resistance to infection, lower risk for migration, less adhesion formation, and lower hernia recurrence rate [11,12]. For the treatment of hernia rings >10 cm in diameter, a pedicled muscle flap has been proposed to be cut in the anterior abdominal wall close to the hernia ring, then flipped over to cover and fix the defect [6]. In emergency diaphragmatic hernia repair, especially in cases of contamination such as gastrointestinal strangulated necrosis, absorbable mesh is not appropriate due to high postoperative infection rates [7,13]. This study innovatively proposes the use of hernia ring orthopedic suture for adult giant diaphragmatic hernias (diameter >10cm): the circular hiatus was extended to make it an oval shape, the tension on both sides of the hiatus was reduced, and then the diaphragmatic hiatus was closed from left to right with nonresorbable 10-thickness silk intermittent mattress suture.
There is no need to free the hernia sac during the operation. The negative pressure suction is placed into the hernia sac cavity, so that the hernia sac in the thoracic cavity is closely attached to the surface of the closed hernia ring, which is equivalent to the role of autologous mesh reinforcing the weak area, significantly reducing the recurrence, and avoiding the side effects of synthetic or biological mesh such as infection, displacement, and corrosion. It is of great significance to reduce the recurrence and complications after operation of diaphragmatic hernia. Moreover, continuous negative pressure suction of the hernia sac reexpand the left lung compressed by the contents of the hernia gradually and avoid lung edema caused by the rapid expansion after the closure of the hernia ring. During anesthesia induction in diaphragmatic hernia repair, double-lumen endotracheal intubation catheter and one-lung ventilation are commonly used to prevent the movement of the affected diaphragm, facilitate the suture of the diaphragm, and reduce cardiopulmonary complications [10]. However, there may still be adverse consequences such as pulmonary edema and atelectasis after suturation of the affected lung. Therefore, continuous negative pressure suction of the hernia sac was used to reexpand the lung slowly. At the same time, there is no need to open the hernia sac, enter the chest cavity and place negative pressure drainage tube into the thoracic cavity, which can avoid injury of thoracic organs and blood vessels and nerves and promote the postoperative recovery.
The results of this study showed that the transabdominal hernia ring orthopedic suture and continuous negative pressure suction of hernia sac cavity has the characteristics of short operation time, less injury and no need into the thoracic cavity, lower recurrence rate, fewer postoperative complications and better postoperative recovery. This surgical method is a safe and effective method for the treatment of giant diaphragmatic hernia in adults.
Declarations
Acknowledgements: The authors declare no acknowledgements.
Funding: Not applicable.
Availability of data and materials: The data and materials analyzed in this study available from the corresponding author on request.
Ethics approval and consent to participate: The Ethics Committee of The First Navy Hospital of Southern Theater Command approved the study.
Conflict of interest: The authors declare no conflict of interest.
References
- Mario Giuffrida, Gennaro Perrone, Fikri Abu-Zidan. Management of complicated diaphragmatic hernia in the acute setting: A WSES position paper. World J Emerg Surg. 2023; 18(1): 43.
- María-Carmen Fernández-Moreno, María-Eugenia Barrios Carvajal, Fernando López Mozos. When laparoscopic repair is feasible for diaphragmatic hernia in adults? A retrospective study and literature review. Surg Endosc. 2022; 36(5): 3347-3355.
- Roberto Torres-Aguiar, Victor Cabrera-Bou, Luis F Serrano. Laparoscopic Repair of a Congenital Diaphragmatic Hernia Presenting with a Small Bowel Obstruction. CRSLS. 2023; 10(1): e2022.00091.
- Héloïse Tessely, Stéphane Journé, Alexis Therasse. A case of colon necrosis resulting from a delayed traumatic diaphragmatic hernia. J Surg Case Rep. 2020; 2020(6): rjaa101.
- Rim H Charara, Rana Ibrahim, Rana Zaarour. Laparoscopic Repair of Acute Traumatic Diaphragmatic Hernia: A Case Report. Cureus. 2023;15(6): e40959.
- Qiaonan Liu, Li Luan, Guangyong Zhang. Treatment of Chronic Traumatic Diaphragmatic Hernia Based on Laparoscopic Repair: Experiences From 23 Cases. Front Surg. 2021; 8: 706824.
- Filipa Campos Costa, Vasco Cardoso, Ana Maria Monteiro. Laparoscopic Repair of an Acute Traumatic Diaphragmatic Hernia: Clinical Case. Cureus. 2020; 12(10): e11082.
- Junsheng Li, Chenchen Guo, Xiangyu Shao. Another type of diaphragmatic hernia to remember: parahiatal hernia. ANZ J Surg. 2020; 90(11): 2180-2186.
- O Basol, H Bilge. Our surgical experience in traumatic and congenital diaphragmatic hernia: Single-center study. Niger J Clin Pract. 2022; 25(4): 391-394.
- Saki Nishikawa, Masashi Miguchi, Hideki Nakahara. Laparoscopic repair of traumatic diaphragmatic hernia with colon incarceration: A case report. Asian J Endosc Surg. 2021; 14(2): 258-261.
- Satoshi Higuchi, Tsuyoshi Takahashi, Yukinori Kurokawa. Laparoscopic repair of a traumatic diaphragmatic hernia with repeated colon incarcerations 7 years after injury: A case report. Surg Case Rep. 2023; 9(1): 212.
- Manuel Gielis, Nicolás Bruera, Agustín Pinsak. Laparoscopic repair of acute traumatic diaphragmatic hernia with mesh reinforcement: A case report. Int J Surg Case Rep. 2022: 93: 106910.
- Tommaso Panici Tonucci, Emanuele Asti, Andrea Sironi. Safety and Efficacy of Crura Augmentation with Phasix ST Mesh for Large Hiatal Hernia: 3-Year Single-Center Experience. J Laparoendosc Adv Surg Tech A. 2020; 30(4): 369-372.
