
Open Access, Volume 10
Severe necrotising pneumonia complicating COVID-19 infection in an adolescent boy
M Van Zanten1*; S Vaassen2; GTJ Van Well3; MAGE Bannier4
1Department of Pediatrics, Maastricht University Medical Centre, Maastricht, The Netherlands.
2Department of Pediatrics, Pediatric Intensive Care Unit, Maastricht University Medical Centre, Maastricht, The Netherlands.
3Department of Pediatrics, Division of Pediatric Infectious Diseases & Immunology & Rheumatology, Maastricht University Medical Centre, Maastricht, The Netherlands.
4Department of Pediatrics, Division of Pediatric Respiratory Medicine, Maastricht University Medical Centre, Maastricht, The Netherlands.
M Van Zanten
Department of Pediatrics, Maastricht University Medical Centre, Maastricht, The Netherlands.
Email: m.van_zanten@lumc.nl
Received : Feb 19, 2024,
Accepted : Mar 19, 2024
Published : Mar 29, 2024,
Archived : www.jclinmedcasereports.com
Abstract
We present a case of an early adolescent boy with respiratory insufficiency due to COVID-19 pneumonia with pulmonary embolisms, treated with corticosteroids, antibiotics, low molecular weight heparin and tocilizumab. His course was complicated by necrotising pneumonia with need for pleural drainage, tracheal cannula placement and antibiotics. We believe immunosuppressive medication potentially played a role in this course of disease.
Keywords: COVID-19; Infection; Necrotising pneumonia; Pediatrics; Drugs and medicines; Intensive care.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Van Zanten M (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Van Zanten M, Vaassen S, Van Well GTJ, Bannier MAGE. Severe necrotising pneumonia complicating COVID-19 infection in an adolescent boy. Open J Clin Med Case Rep. 2024; 2215.
Introduction
COVID-19 infections are a huge health burden, but serious infections are fortunately rare in children. This instructive case describes a severe COVID-19 pneumonia in an adolescent boy. He was treated according to adult guidelines as there were no pediatric guidelines at the time. Even now, adult guidelines are often followed or adult research is used for pediatric guidelines, as there is only little research in children. We believe immunosuppressive medication, including the use of monoclonal antibodies, might have had an impact on the development of necrotising pneumonia in our patient. Therefore, we believe treatment with off-label immunosuppressive medication should not be taken lightly.
Case Presentation
An early adolescent, overweight boy with a history of foetal alcohol syndrome presented with respiratory insufficiency due to COVID-19 pneumonia (Figure 1A for typical ground glass opacities on CT-scan). Prior to this infection, he had not received any vaccine against COVID-19, did not have a history of fungal infections and had not been in contact with tuberculosis to our knowledge. Because of severe tachydyspnea and an O2 saturation of 80%, despite being treated with Continuous Positive Airway Pressure (CPAP), he was intubated and transferred, in prone position, to our Pediatric Intensive Care Unit (PICU) for respiratory support. Laboratory investigations were notable for pCO2 of 6.5 kPa, CRP 105 mg/L and D-dimer level of 35000 mcg/L. He was treated with dexamethasone, ceftriaxone and a single dose of tocilizumab according to adult guidelines at that time as he was in need of respiratory support and therefor in critical condition [1]. His clinical course was complicated by pulmonary embolisms for which he was treated with Low Molecular Weight Heparins (LMWH). The D-dimer level at that time was >10000 mcg/L (Figure 1B for bilateral segmental pulmonary embolisms).
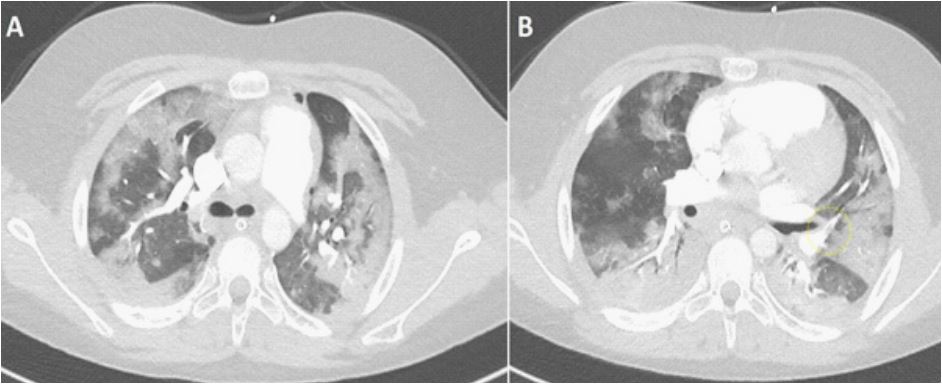
Figure 1: (A,B) CT scan at time of admittance.
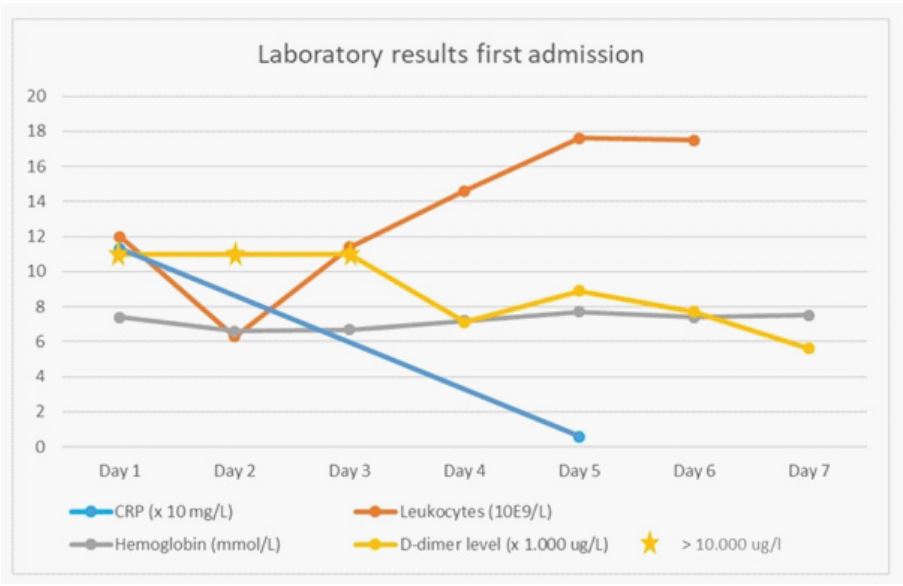
Figure 2: Drawings in 6 to 9 months after UCBC therapy.
COVID-19 was confirmed with a RT-PCR test. Blood cultures and sputum cultures remained negative. On day 6 after hospital admission he was extubated and weaned off supplemental oxygen. On day 10 after admission he was transferred back to the referring hospital. He was re-admitted on day 14 due to respiratory deterioration, tachypnea with a respiratory rate of 30/minute, with need for High Flow Nasal Oxygen (HFNO) therapy 60 l/min and O2 of 60%. Piperacillin-tazobactam was started because of suspected hospital-acquired pneumonia. CRP increased to maximally 344 mg/L (Figure 2 and 3 for the course of the inflammatory parameters for both admissions). Pulmonary CT-scan showed bilateral pleural effusions (Figure 4A). Pre-existent ground glass opacities had now become consolidations with cavitation suggestive of Necrotising Pneumonia (NP) (Figure 4B). The pulmonary embolisms were diminished (Figure 4C).
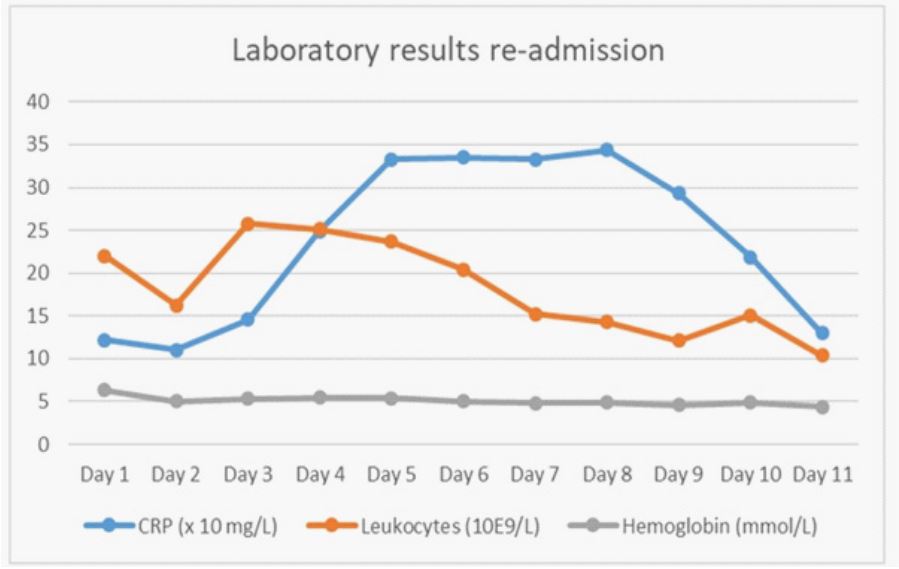
Figure 3: Laboratory results of re-admission.
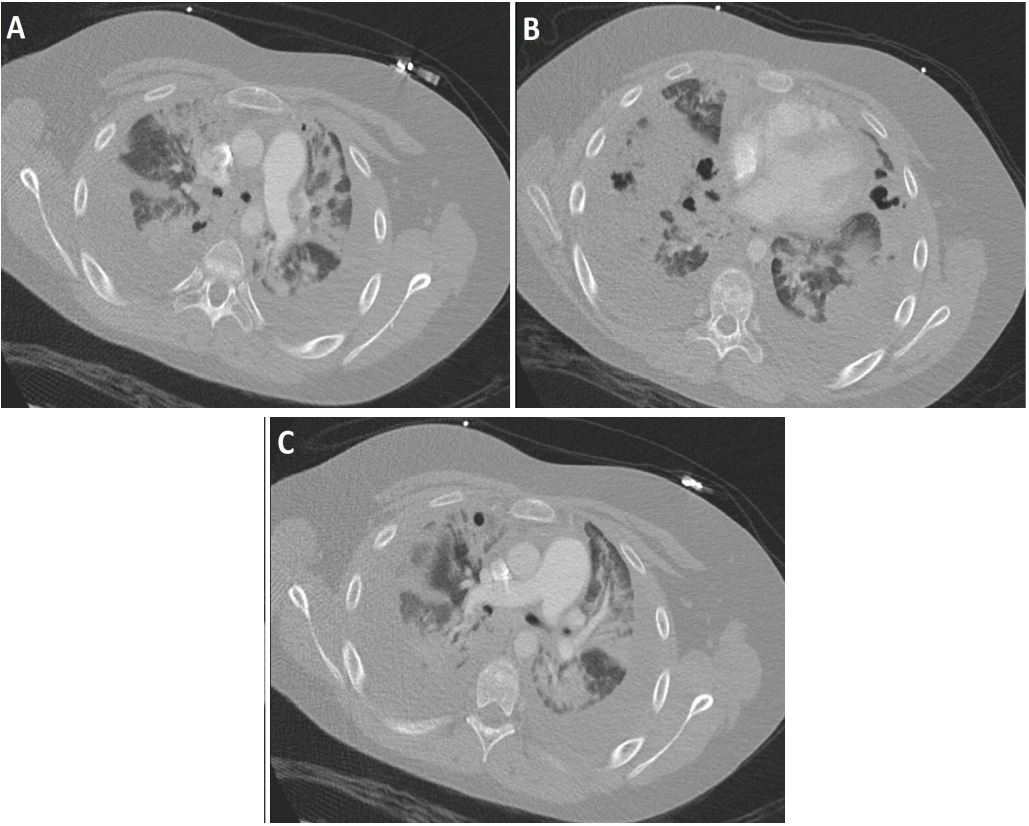
Figure 4: (A-C) CT scan at time of deterioration.
A Broncho-Alveolar Lavage (BAL) was performed for diagnostic purposes, and bilateral pleural drains were inserted. As a result, 1500 ml of serosanguinolent fluid was evacuated, which was biochemically best classified as an empyema (pH 7.21, total protein 43 g/L, LDH 1482 U/L). BAL cultures showed minimal growth of Candida albicans species. Comprehensive microbiological elaboration of obtained BAL and pleural fluids, including bacterial, yeast and fungal cultures, as well as 16-S ribosomal RNA PCR, failed to show a causal pathogen. On day 17 the pleural drains were removed. Because of persistent fever Piperacillin-tazobactam was switched to Meropenem for a total of 7 days. Clindamycin was added for a total of 6 weeks. Because of prolonged need for mechanical ventilation a tracheal cannula was inserted on day 24. On day 45 he was weaned from mechanical ventilation and he was treated with Continuous Positive Airway Pressure (CPAP) during the night. On day 49 after hospital admission he was decannulated, and shortly hereafter discharged to a physical rehabilitation centre. At follow-up 4 months after admission, he was completely recovered.
Discussion
We present a case of severe COVID-19 pneumonia in an early adolescent boy, complicated by NP and pleural empyema. In general, the course of COVID-19 in children is mild. Severe COVID-19 infections, including severe COVID-19 pneumonia, are rarely reported in children [2]. Therefore, our case has several key points to share. First, our patient had an unusually severe ARDS due to COVID-19 pneumonia, with a complication ultimately necessitating tracheal cannula placement. Second, NP as a complication of COVID-19 pneumonia is reported only twice before in children [3,4]. Third, our case warrants vigilance in prescribing immunosuppressive treatment in children, which is broadly integrated in national and international COVID-19 guidelines in adults [1].
The incidence of COVID-19 in children is increasing worldwide [5]. The clinical picture in children is different compared to the now well-known clinical picture of severe pneumonia and ARDS in adults. Usually, COVID-19 presents as a mild infection in children. In the Netherlands, approximately 40% of COVID-19 infections in children present with respiratory symptoms [6]. Only a small group of children needs supplemental oxygen therapy, and only in rare cases mechanical ventilation is necessary. Other respiratory complications are rare, especially compared to adults in whom pulmonary embolisms, bacterial superinfections and fungal infections are more common [7]. Beside respiratory presentations and potential complications, children might present with Multisystem Inflammatory Syndrome in Children (MIS-C) associated with COVID-19, a severe disorder characterized by inflammatory dysregulation and multi-organ involvement [6]. As stated before, NP as a complication of COVID-19 pneumonia is reported only twice before in children [3,4]. Whereas in adults, several reports of NP complicating COVID-19 are reported [8-11]. Therefore, the severe respiratory problems in our case are rare and the course seems more comparable to the adult course of severe COVID-19 pneumonia.
Based on the current international WHO guideline for COVID-19 in adults, severely ill patients are treated with tocilizumab [1]. Evidence show that acute lung injury might be caused by a cytokine storm [12]. In severe cases the levels of Interleukins (IL) were raised along with other immunologic factors (Macrophage inflammatory protein 1, tumor necrosis factor-α, monocyte chemoattractant protein, and Interferon gamma-induced protein) [13]. Patients with COVID-19 infections have higher levels of IL-6 in CD4+ T-cells and monocytes, which suggests a prominent role of IL-6 in the inflammatory cytokine storm [13,14]. Based on these raised levels of IL-6, inhibiting IL-6 was proposed as a treatment option to decrease the severity of inflammation and improve prognosis [13]. A meta-analysis of Shankar-Hari et al. showed that administration of IL-6 antagonists in hospitalized patients with COVID-19 was associated with a lower 28-day all-cause mortality [15]. In children, literature on this topic is sparse, although a recent retrospective case series report by Teoh et al. suggests that administration of tocilizumab earlier in the illness course and PICU admission is associated with better outcomes in children and young adults [16]. Charan et al. studied the adverse drug events reported in the WHO database [13]. They showed that 7.8% of the adverse events were infections and infestations [13]. Studies conducted on COVID-19 patients using tocilizumab reported varied rates of bacterial infections and superinfections with a range of 3% up to 50% [13]. These superinfections could be due to suppression of the immune system by blocking the IL-6 pathway, as IL-6 is crucial in antibody synthesis, and therefore studied by several research groups [15,17,18]. Unfortunately, evidence is conflicting. Shankar-Hari et al. described no significant difference in occurrence as 21.9% of patients treated with IL-6 antagonists had an infection compared to 17.6% of patients treated with usual care (OR 0.99; 95% CI, 0.85-1.16) [15]. On the other hand Burmester et al. show that patients who use tocilizumab are more at risk for infections with a risk of 3.1% of developing a serious infection such as pneumonia or abscess [17]. In addition De Benedetti found that patients treated for a longer period of time, had a risk of 11% of a serious infection per year of treatment [18]. Taken together, evidence is conflicting but suggestive for an additional risk of infection when adding IL-6 antagonists to the treatment. In adults, several reports of NP complicating a primary COVID-19 infection were recently reported [8-11] and bacterial or fungal causes were isolated frequently [9]. Unfortunately, in our case no causal microorganisms were isolated despite various cultures and tests of different sources, including bacterial, yeast and fungal cultures, as well as non-tuberculous and tuberculous mycobacterial PCR and Galactomannan tests. However, negative cultures are not uncommon in NP in children, as literature shows that a causative pathogens for NP were identified in only 37.5%-47.6% [2,19,20]. Nevertheless, given the severity of the infection, a bacterial superinfection is still most likely the cause of NP in our patient.
Theories are proposed why patients with COVID-19 pneumonia might be more susceptible to NP. These include acute and severely high levels of inflammation [11,21] and frequent occurrence of pulmonary embolisms [11], Some suggest an additional risk due to the high prevalence of bacterial coinfections [11,22]. In theory this latter might be due to the need for immunosuppressive drugs. In our case all could be applicable as our patient had a proven COVID-19 pneumonia with a clinically severe ARDS, for which he was treated with the immunosuppressive drugs dexamethasone and tocilizumab. Moreover, he had proven pulmonary embolisms. Of specific interest is the timing of NP development in our case. Our patient was clinically improving, transferred to the referral hospital, and had started a rehabilitation program when he suddenly deteriorated. It therefore seems unlikely that NP was a direct complication of the COVID-19 infection itself. A repeated pulmonary CT scan did not show any new pulmonary embolisms and showed significant improvement of the primary embolisms. Therefore, secondary pneumonia due to pulmonary embolisms also seems an unlikely cause. The influence of immune suppressive medication might be an important factor, as our patient was both treated with dexamethasone for 10 days and a single dose of tocilizumab, which has a half-life of 6-18 days.
In this case we followed current adult guidelines in treating COVID-19 infections in spite of his age, because of the severity of the illness and because he had an adult posture. Besides there were no guidelines for children at that time. Therefore we started dexamethasone and added tocilizumab when there was no improvement, as there was a risk of death without adequate treatment. As described above, studies in adults show that tocilizumab improves the outcome for patients with COVID-19, but prospective studies in children are currently lacking. We thus advise to be vigilant when prescribing off-label immunosuppressive drugs in children and adolescents. More research is needed to assess the safety of monoclonal antibodies during COVID-19 in children and adolescents.
Finally, it should be noted that our patient had not received any vaccine against COVID-19. Recent literature shows that vaccination against COVID-19 has led to a significant decrease in morbidity and mortality in adults [23,24]. In children, COVID-19 vaccination is associated with significantly less development of MIS-C [25]. Therefore, these findings raise the question if the severe complicated course of our patient could have been prevented by adequate COVID-19 vaccination.
Conclusion
We present a rare case of severe COVID-19 pneumonia in an early adolescent boy, complicated by pulmonary embolisms and NP, resulting in a prolonged need of respiratory support and ultimately tracheal cannula placement. Overall, NP is a rare condition in children, and until now only two other paediatric case of NP complicating COVID-19 were reported. Immunosuppressive medication, including the use of monoclonal antibodies, might have had a role in the development of NP in our patient. Therefore, treatment with off-label immunosuppressive medication should not be taken lightly. In addition we believe more research is necessary, especially in children, to evaluate the potential harm versus the benefits when using immunosuppressive medication in COVID-19 infections. We should be vigilant that the remedy is not worse than the disease.
References
- Lamontagne F, Agarwal A, Rochwerg B, et al. A living WHO guideline on drugs for covid-19. BMJ. 2020; 370: m3379.
- Krenke K, Sanocki M, Urbankowska E, et al. Necrotizing Pneumonia and Its Complications in Children. Adv Exp Med Biol. 2015; 857: 9-17.
- Akuamoah Boateng G, Ristagno EH, Levy E, et al. A complicated presentation of pediatric COVID-19 with necrotizing pneumonia and pulmonary artery pseudoaneurysms. Pediatr Pulmonol. 2021; 56(12): 4042-44.
- Brisca G, Buratti S, Basso L, et al. Necrotizing pneumonia and severe COVID-19 in an infant with catheter-related bloodstream infection by methicillin-sensitive Staphylococcus aureus. Pediatr Int. 2023; 65(1): e15401.
- Marks KJ, Whitaker M, Anglin O, et al. Hospitalizations of Children and Adolescents with Laboratory-Confirmed COVID-19 - COVID-NET, 14 States, July 2021-January 2022. MMWR Morb Mortal Wkly Rep. 2022; 71(7): 271-78.
- Dashboard covid in kids The Netherlands. 29.10.2022; Available from: https://www.covidkids.nl/scientific-dashboard/.
- Ludvigsson JF. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020; 109(6): 1088-95.
- Chaudhry B, Alekseyev K, Didenko L, et al. Post COVID-19 MSSA pneumonia. SAGE Open Med Case Rep. 2021; 9: 2050313x211005996.
- Hidron A, Quiceno W, Cardeño JJ, et al. Post-COVID-19 Necrotizing Pneumonia in Patients on Invasive Mechanical Ventilation. Infect Dis Rep. 2021; 13(3): 835-42.
- Peeters K, Mesotten D, Willaert X, et al. Salvage Lobectomy to Treat Necrotizing SARS-CoV-2 Pneumonia Complicated by a Bronchopleural Fistula. Ann Thorac Surg. 2021; 111(4): e241-e43.
- Jung C, Gillmann HJ, Stueber T, et al. Spontaneous massive hemothorax as a complication of necrotizing pneumonia in a patient with severe acute respiratory syndrome coronavirus 2 induced acute respiratory distress syndrome: a case report. J Med Case Rep. 2021; 15(1): 444.
- Hu B, Huang S, Yin L. The cytokine storm and COVID-19. J Med Virol. 2021; 93(1): 250-56.
- Charan J, Dutta S, Kaur R, et al. Tocilizumab in COVID-19: a study of adverse drug events reported in the WHO database. Expert Opin Drug Saf. 2021; 20(9): 1125-36.
- Rizzi M, D’Onghia D, Tonello S, et al. COVID-19 Biomarkers at the Crossroad between Patient Stratification and Targeted Therapy: The Role of Validated and Proposed Parameters. Int J Mol Sci. 2023; 24(8).
- Shankar-Hari M, Vale CL, Godolphin PJ, et al. Association between Administration of IL-6 Antagonists and Mortality among Patients Hospitalized for COVID-19: A Meta-analysis. Jama. 2021; 326(6): 499-518.
- Teoh Z, Danziger-Isakov L, Courter JD, et al. Tocilizumab for Treatment of Children and Young Adults with Severe Acute COVID-19: Experience at a Quaternary-care Children’s Hospital. Pediatr Infect Dis J. 2023; 42(2): 119-21.
- Burmester GR, Feist E, Kellner H, et al. Effectiveness and safety of the interleukin 6-receptor antagonist tocilizumab after 4 and 24 weeks in patients with active rheumatoid arthritis: the first phase IIIb real-life study (TAMARA). Ann Rheum Dis. 2011; 70(5): 755-9.
- De Benedetti F, Brunner HI, Ruperto N, et al. Randomized trial of tocilizumab in systemic juvenile idiopathic arthritis. N Engl J Med. 2012; 367(25): 2385-95.
- Ness-Cochinwala M, Kobaitri K, Totapally BR. Characteristics and Outcomes of Children With Necrotizing Pneumonia. Pediatr Crit Care Med. 2021; 22(12): e640-e43.
- Ramgopal S, Ivan Y, Medsinge A, et al. Pediatric Necrotizing Pneumonia: A Case Report and Review of the Literature. Pediatric Emerg Care. 2017; 33(2): 112-15.
- Long A and Grimaldo F. The authors’ response to A more realistic relationship between covid 19 and hemopneumothorax. Am J Emerg Med. 2020; 38(10): 2219.
- Duployez C, Le Guern R, Tinez C, et al. Panton-Valentine Leukocidin-Secreting Staphylococcus aureus Pneumonia Complicating COVID-19. Emerg Infect Dis. 2020; 26(8): 1939-41.
- Liu Q, Qin C, Liu M, et al. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: a systematic review and metaanalysis. Infect Dis Poverty. 2021; 10(1): 132.
- Moghadas SM, Vilches TN, Zhang K, et al. The Impact of Vaccination on Coronavirus Disease 2019 (COVID-19) Outbreaks in the United States. Clin Infect Dis. 2021; 73(12): 2257-64.
- Hamad Saied M, van der Griend L, van Straalen JW, et al. The protective effect of COVID-19 vaccines on developing multisystem inflammatory syndrome in children (MIS-C): A systematic literature review and meta-analysis. Pediatr Rheumatol Online J. 2023; 21(1): 80.
