
Open Access, Volume 10
Rare form of lipoblastoma: Lipoblastoma of the thigh in older children
Zied Mansi1*; Tounsi Abdelkader1; Mahmoudi Ahmed1; Islem Chneti1; Hedi Rbai1; Wajdi Chermiti2; Ali Haggui3; Bacem Zaidi4; Wael Gazzah5
1Department of Orthopedic Surgery, IBN EL JAZZAR University Hospital, Kairouan, Tunisia.
2Department of Orthopedic Surgery, SAHLOUL University Hospital, Sousse, Tunisia.
3Department of Orthopedic Surgery, Hospital of Kasserine, Kasserine, Tunisia.
4Department of General Surgery, IBN EL JAZZAR University Hospital, Kairouan, Tunisia.
5Department of General Urology, IBN EL JAZZAR University Hospital, Kairouan, Tunisia.
Zied Mansi
Department of Orthopedic Surgery, IBN EL JAZZAR University Hospital, Kairouan, Tunisia.
Email: doc.zm@htmail.fr
Received : Jan 23, 2024,
Accepted : Mar 18, 2024
Published : Mar 20, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Lipoblastoma is a relatively rare benign tumor. It derives from embryonic white fat cells. It almost exclusively affects children less than 3 years of age. We report a case of lipoblastoma of the left thigh detected in an older child (11 years) and a literature review. Diagnosis was based on histology while surgical treatment was based on total resection of the mass. The postoperative course was simple with a follow-up period of 9 months.
Keywords: Lipoblastoma; Badipose tumor; Large child.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Mansi Z (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Mansi Z, Abdelkader T, Ahmed M, Chneti I, Rbai H, Chermiti W, Haggui A, et al. Rare form of lipoblastoma: Lipoblastoma of the thigh in older children. Open J Clin Med Case Rep. 2024; 2213.
Introduction
Lipoblastoma is a rare benign white fat tumor of embryonal origin. It appears almost exclusively in small children (under 3 years old) [1]. There is a slight male predominance. To date, fewer than 200 cases have been reported in the literature [2]. It can present either as a well-demarcated, encapsulated tumor (benign lipoblastoma), or non-encapsulated, infiltrative and diffuse (lipoblastomatosis) [1,2].
Case Presentation
Patient and observation Child aged 11, male, was taken for consultation for a swelling of the left thigh which had been progressively evolving for 7 months. He had no signs of fever or lameness, his general condition was preserved. Clinical examination found a mass measuring 10 cm in long axis on the anterior surface of the proximal 1/3 of the left thigh. It was firm in consistency, painless, without associated inflammatory signs, mobile in relation to the superficial plane and fixed in relation to the deep plane. Elsewhere the somatic examination was normal. The biological assessment was normal. The frontal X-ray of the thigh (Figure 1) showed infiltration of the soft tissues without bone lesions. Ultrasound study of the mass revealed the presence of a well-defined, heterogeneous hyper-echoic formation, crossed by thick and hypervascularized septa on color Doppler. Magnetic Resonance Imaging (MRI) revealed a sub-aponeurotic intermuscular tumor process with a heterogeneous signal with a fatty component in hyper-signal T1 (Figure 2A and B) and T2 (Figure 2C) fading after saturation of the fat. And a tissue component with T1 hypo-signal, intermediate T2 hyper-signal enhancing after Gadolinium injection, without cortical lysis or associated bone signal anomaly. The preoperative biopsy of the mass came back in favor of a lipoblastoma without signs of malignancy (Figure 3A). The indication for tumor excision surgery was retained. The approach was a longitudinal incision extending the old biopsy incision on the anterior surface of the thigh. Surgical exploration found an encapsulated mass very adherent to the different musculoaponeurotic planes which it repressed without invading them (Figure 3B). It was also adherent to the femoral periosteum. The mass was completely resected without capsular opening, following the cleavage planes between it and the muscular planes and removing part of the periosteum. It measured 12 cm in long axis containing several lobules with fatty appearances grouped in clusters (Figure 3C). Histological analysis of the excision specimen confirmed the results of the biopsy by showing an adipose tumor proliferation, made up of regular, large adipocytes whose nuclei are barely visible, suggesting a lipoblastoma without signs of malignancy.

Figure 1: Standard radiograph of the left thigh showing opacity of the
external lateral soft tissues with no bony abnormality adjacent.
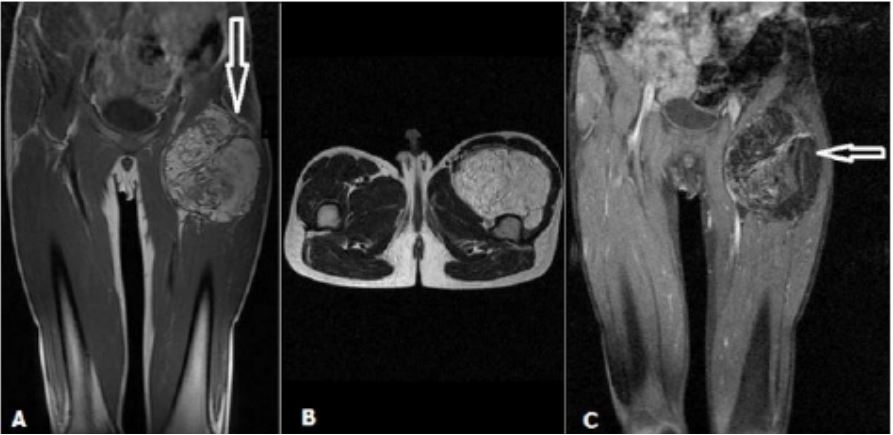
Figure 2: MRI: T1-weighted sequences without (Figure A and B) and with FATSAT injected (C), T2-weighted sequence showing a large mass of the left thigh heterogeneous T1 and T2 hyper-signal enhanced
weakly after contrast and disappearing after saturation of the fat.

Figure 3: Preoperative biopsy showing adipose proliferation consisting of regular adipocytes, arranged in
nodules of variable sizes whose nuclei are barely visible; we also find numerous small stellate cells. The
latter are arranged on a myxoid background between the adipocytes: (A) they do not show signs of malignancy; (B) intraoperative view showing a well encapsulated mass pushing back the different muscular
planes; (C) voluminous well-encapsulated adipose mass.
Discussion
Lipoblastoma is a benign fatty tumor of embryonal origin [1]. It is relatively rare, currently less than 200 cases have been reported in the literature [1]. It occurs almost exclusively in young children under 3 years old with an average age of 12 months [1,2]. This tumor rarely appears after the age of 10; we found only one description in a 12-year-old child who had a retroperitoneal location [1,3]. Our case appears to be one of the rare cases known in the literature occurring after the age of 11 years. Clinically, lipoblastoma presents as a tumor of variable size and growth, most often small and asymptomatic. It can become symptomatic in certain locations due to compression of neighboring structures: dyspnea, hypoxia, stridor (thoracic location) and edema of the lower limbs (retroperitoneal location) [1]. Location at the extremities is by far the most common [1,4,5]. This tumor presents in two forms: A well-defined, encapsulated tumor (benign lipoblastoma), or non-encapsulated, infiltrative and diffuse (lipoblastomatosis) [1-3,6-8]. In our patient, the tumor was deep, well defined and encapsulated, which is also a rare description. In most cases preoperative diagnosis is not possible. The biological assessment is not of much benefit. Standard radiography shows no calcifications or bone lysis. Ultrasound can reveal a mass of heterogeneous, lobulated echostructure that may contain cystic formations within it. Computed Tomography (CT) or better Magnetic Resonance Imaging (MRI) makes it possible to specify the location, size, relationships as well as the lobulated and lipomatous character [1,4]. All of these above-described characteristics were found in our patient. The definitive diagnosis is histopathological through a surgical biopsy, making it possible to eliminate a malignant tumor at the same time. Treatment is surgical with total excision of the lesion. Incomplete excision is a potential source of tumor recurrence. The surgical aftermath is generally simple. The prognosis is good.
Conclusion
Lipoblastoma is a rare, well-encapsulated benign tumor almost exclusively described in children under 3 years of age. The clinic is non-specific. Magnetic resonance imaging helps guide the diagnosis, which can only be confirmed by histopathological examination. The treatment is surgical with total excision. The prognosis is good. Through this article, we reported the case of an atypical lipoblastoma of the left thigh, occurring in a large child (aged over 11 years) and of deep location.
References
- Harrer J, Hammon G, Wagner T, Bolkenius M. Lipoblastoma and Lipoblastomatosis: A report of two cases and review of the literature. Eur J Pediatr Surg. 2001; 11(5): 342-9.
- Miller GG, Yanchar NL, Magee JF, Blair GK. Lipoblastoma and liposarcoma in children: An analysis of 9 cases and a review of the literature. Can J Surg. 1998 Dec; 41(6): 455- 8.
- Jimenez JF. Lipoblastoma in infancy and childhood. J Surg Oncol. 1986; 32(4): 238-44.
- Yada K, Ishibashi H, Mori H, Shimada M. Intrascrotal lipoblastoma: Report of a case and the review of literature. Surg Case Rep. 2016; 2(1): 34.
- Beebe MM, Smith MD. Omental lipoblastoma. J Pediatr Surg. 1993; 28(12): 1626-7.
- Crozier F, Jouve JL, Zattara-Cannoni H, Bouvier C, Jaoua S, et al. Lipoblastoma of the buttock. J Radiol. 2002; 83(7-8): 983-5.
- Stock N. Adipose tumors. Ann Pathol. 2015; 35(1): 41-53.
- Papillard-Maréchal S, Brisse HJ, Pannier S, Ilharreborde B, Philippe-Chomette P, et al. Tumor-like soft tissue masses in children and adolescents. Arch Pediatr. 2015; 22(1): 14-23.
