
Open Access, Volume 10
Cytomegalovirus pneumonia in a patient with systemic lupus erythematous on treatment with hydroxychloroquine: A case report
Valentina Morena1*; Lucia Bradanini1; Annacarla Chiesa1; Federico Conti1; Nicole Gemignani1; Chiara Molteni1; Alessandro Pandolfo1; Sara Volpi1; Carola Mauri2; Silvia Tonolo2; Silvia Pontiggia1; Stefania Piconi1
1Infectious Diseases Unit, “Alessandro Manzoni” Hospital, ASST Lecco, Lecco, Italy.
2Microbiology Unit, “Alessandro Manzoni” Hospital, ASST Lecco, Lecco, Italy
Valentina Morena
Infectious Diseases Unit, “Alessandro Manzoni” Hospital, ASST Lecco, Lecco, Italy.
Email: v.morena@asst-lecco.it
Received : Feb 07, 2024,
Accepted : Mar 06, 2024
Published : Mar 11, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Ability of Cytomegalovirus (CMV) to cause invasive disease is dependent on host immune status. Pneumonia, which is generally expression of reactivation of a latent infection, typically affects deeply immunocompromised patients such as transplant recipients.
We present here the case of a primary CMV infection complicated by interstitial pneumonia in a 26-yearsold girl with Systemic Lupus Erythematosus (SLE) on treatment with hydroxychloroquine. She presented to our ER with fever and respiratory failure; chest X-ray showed bilateral interstitial pneumonia. CMV serology was consistent with acute infection (IgG negative 5UI/ml, IgM positive 150UI/ml, low IgG avidity <0.15). CMV-DNA was confirmed positive with Viral Load (VL) of 157960 cp/ml on Bronco-Alveolar Lavage (BAL) and with VL of 66500 cp/ml on serum. We started empiric treatment with ganciclovir with rapid clinical improvement and quick oxygen weaning. After one week serum CMV-DNA VL had dropped to 1630 cp/ml and it was negative after 14 days. The patient was discharged with oral valganciclovir, continued until completion of 21 days of treatment. After 90 days complete seroconversion for CMV was seen (IgG 163 UI/ml, IgM 129 UI/ml, avidity 2.38).
Case series of CMV pneumonia in rheumatological patients undergoing immunosuppressive therapy such as high-dose steroid are described in literature. Patients with SLE, even in absence of immunosuppressive drugs, may have an increased risk of invasive CMV disease due to a primary dysfunction of immune system.
Keywords: Cytomegalovirus, Systemic lupus erythematous; Immunocompromised patients; Hydroxychloroquine; Ganciclovir; Pneumonia
Abbreviations: AIDS: Acquired Immune Deficiency Syndrome; BAL: Broncho-Alveolar Lavage; CMV: Cytomegalovirus; CT: Computed Tomography; ER: Emergency Room; Fig: Figure; PCR: Polymerase Chain Reaction; SLE: Systemic Lupus Erythematous; SpO2 : Peripheral Oxygen Saturation; VL: Viral Load; WBC: White Blood Cells
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Morena V (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Morena V, Bradanini L, Chiesa A, Conti F, Gemignani N, Molteni C, Pandolfo A, et al. Cytomegalovirus pneumonia in a patient with systemic lupus erythematous on treatment with hydroxychloroquine: a case report. Open J Clin Med Case Rep. 2024; 2207.
Introduction
Rheumatic diseases are characterized by several immune function abnormalities. Impaired immune response, together with treatment with immunosuppressive therapy, can increase the frequency of both community-acquired and opportunistic infections [1].
Cytomegalovirus (CMV) is a widespread herpes virus. The seroprevalence of prior CMV infection ranges from 40% to 100% in adults worldwide [2]. A syndrome resembling infectious mononucleosis is the most common presentation of primary symptomatic cytomegalovirus infection in immunocompetent adults; organ-specific complications (gastrointestinal, hepatic, neurologic and pulmonary involvement) are extremely rare and limited to case series and reports [3-5].
After primary infection, CMV remains latent in different cells of the immune system (like CD34+ cells and CD14+ monocytes and macrophages) and it persists for life [6]. CMV reactivation may occur depending on host immune status and can cause a potentially fatal infection in immunocompromised patients. Most common clinical presentations are colitis, retinitis, pneumonia, hepatitis and encephalitis, which are widely described in patients with Acquired Immune Deficiency Syndrome (AIDS) or solid organ and hematopoietic cell transplant recipients [7].
CMV infection can also present in patients with rheumatic diseases and it is generally related to use of immunosuppressive treatments such as corticosteroids [8]. Incidence, clinical characteristics and prognosis of CMV infection complications in rheumatic diseases have not been clarified [9]. Here, we present the case of a 26-years-old girl affected with juvenile Systemic Lupus Erythematous (SLE), in remission and in therapy with hydroxychloroquine, who presented to our Clinic with a CMV primary infection that led to pulmonary involvement with respiratory failure.
Case Report
Our patient is a 26-years-old Italian teacher who worked at nursery school. She had a history of juvenile SLE which was diagnosed when she was 4 years old (diagnosis made because of presence of antiDNA and anti-RO52 antibodies, of anti-phospholipids antibodies and of lupus anticoagulant). She had been treated with corticosteroids since diagnosis until December 2020. She was started with 50 mg of prednisone daily (2.5 mg daily from 05/2019 to 12/2020) and substituted with hydroxychloroquine (started in 06/2020). At the time of admission to our hospital, she was on hydroxychloroquine 200 mg daily and SLE was in remission.
On March 1st, 2021, she started complaining shortness of breath and low-grade fever (37.3°C). Chest x-ray showed interstitial abnormalities and bilateral peripheral infiltrates of the lung basis (Figure 1); a Sars-Cov2 molecular smear was negative. Her General Practitioner started levofloxacin 500 mg daily due to know amoxicillin allergy.
On March 8th the patient went to our Emergency Department because of worsening of symptoms. She presented with dry cough, shore throat, low grade fever (temperature 37.8°C) and shortness of breath. Blood tests showed leukocytosis (WBC 12900/µl – of which 20% were neutrophils and 65% lymphocytes) with atypical lymphocytes and liver function abnormalities (aspartate aminotransferase level 249 UI/L, alanine aminotransferase level 288 UI/L, lactate dehydrogenases 360 mg/dl). C-reactive protein was unremarkable (1 mg/l; reference interval 0-0.5 mg/l). A blood gas analyses showed respiratory failure (pO2 62, pCo2 34). Sars-Cov2 smear was repeated and confirmed negative. A CT-scan was also performed and showed bilateral small random nodules without a particular topographic distribution and associated with air space consolidation in posterior basal lung segments (Figure 2).
The patient was transferred to our Infectious Diseases Unit. At the time of admission, she was afebrile and her peripheral oxygen saturation (SpO2 ) was 97% with 4l/min of oxygen support with nasal cannula. Considering her anamnesis and blood tests, CMV serology was performed and turned out consistent with acute infection: IgG negative (5 UI/ml – considered positive when, 14 UI/ml), IgM positive (150 UI/ ml – positive 22 UI/ml), low IgG avidity (<0.15 – high when, 0.25). A bedside bronchoscopy was performed and Broncho-Alveolar Lavage (BAL) fluid was sent for culture tests for fungi, bacteria and mycobacteria; CMV-DNA PCR, SarsCov2 RNA PCR, and other opportunistic infections (Pneumocystis jirovecii DNA PCR, Galactomannan-antigen, Mycobacterium tuberculosis DNA PCR). CMV-DNA PCR was also performed on serum. Chlamydophila pneumoniae and Mycoplasma pneumoniae antibodies assays were negative. Urinary antigens for Legionella and Streptococcus pneumoniae were negative. Blood cultures were negative for bacteria and fungi. HIV 1-2 antibodies/antigen assay was negative but CD4+ count was decreased with an inversion of CD4/CD8 ratio (CD4 576 cell/µl, CD8 2574 cell/µl, CD4/CD8=0.22).
Considering the clinical suspicion and the serology, we decided to start 5 mg/kg of EV ganciclovir two-times daily while we waited for CMV-DNA PCR. A retinitis was excluded performing a fundus-oculi exam. The patient showed a rapid clinical improvement with quick oxygen weaning and resolution of shortness of breath. CMV-DNA PCR on BAL resulted positive with a Viral Load (VL) of 157960 cp/ml while serum CMV- was positive with VL of 66500 cp/ml. All other microbiological tests resulted negative. Laboratory tests showed a progressive decrease in liver function tests and normalization of WBC. An abdomen ultrasound was performed and showed marked splenomegaly (anterior-posterior diameter of 16 cm) without hepatic abnormalities. After one week of treatment, we repeated serum CMV-DNA and we observed a significant decrease of VL (1630 cp/ml). A chest x-ray was performed on March 17th, which showed resolution of interstitial abnormalities and consistent reduction of bilateral infiltrates (Figure 3). After 10 days IV ganciclovir was switched to oral valganciclovir. On the 14th day of antiviral treatment CMV-DNA PCR on serum was tested negative. We discharged the patient after 15 days of hospitalization. She repeated blood tests as an outpatient. We completed 21 days of antiviral therapy and then we checked blood tests every two weeks till April 30th, 2021, in order to confirm stable negativity of CMV-DNA PCR and normalization of liver function tests.

Figure 1: Interstitial abnormalities and bilateral peripheral infiltrates of the lung basis at chest x-ray

Figure 2: Bilateral small random nodules associated
with air space consolidation in posterior basal lung seen
at CT scan
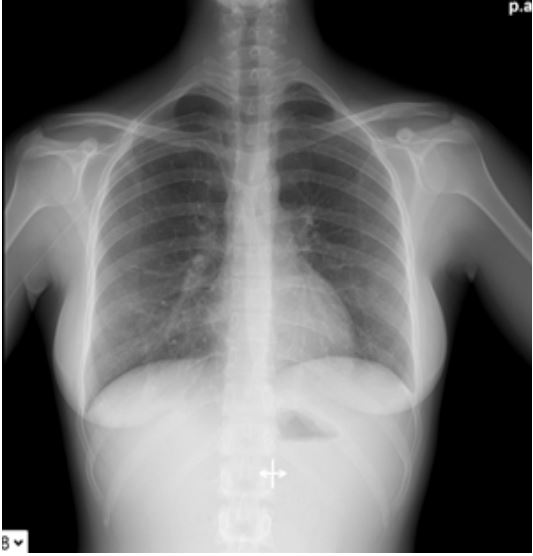
Figure 3: Resolution of interstitial abnormalities and
consistent reduction of bilateral infiltrates
After 90 days (08/07/21) complete seroconversion for CMV was seen (IgG 163 UI/ml, IgM 129 UI/ ml, avidity 2.38). Despite that, CD4:CD8 ratio was still inverted (CD4 591 cell/mmc; CD8 1791 cell/mmc; CD4: CD8 0.33). The patient feels very well and is still working as a teacher
Discussion
The spectrum of human illness caused by cytomegalovirus is diverse and mostly dependent on the host’s immune status. Primary infection occurs when an individual with no immunity against this virus becomes infected for the first time. Afterwards, the virus establishes latency from which it may reactivate [10]. Tissue-invasive CMV diseases is usually expression of CMV reactivation, which occurs mostly in immunocompromised patients like solid organ and hematopoietic cell transplant recipients, HIV-infected people, and those who are treated with immunomodulating drugs [6,8]. Pneumonia is the most common presentation of invasive CMV disease in lung transplant recipients [11]. CMV pneumonia is also described in patients with rheumatic diseases, generally due to a compromised immune function caused by high-dose corticosteroids or other immunosuppressive agents. Xue et al. described the characteristics of 73 cases of CMV pneumonia in patients with rheumatic diseases, mostly SLE and dermatomyositis, all receiving corticosteroid therapy together with other immunosuppressant drugs (cyclophosphamide, azathioprine cyclosporine, leflunomide, mycophenolate mofetil and methotrexate) [8]. Lai et al. described bronchoalveolar lavage fluid analysis in 21 SLE patients with pneumonia, finding CMV in 7 patients; also in this series, patients had been treated with prednisolone (equivalent to a median dosage of 15 mg/day) and immunosuppressive drugs (azathioprine, mycophenolate, calcineurin inhibitors) [12].
CMV pneumonia is rarely seen both in immunocompetent hosts and as manifestation of acute infection. In a literature review, Grilli et al. found 13 cases of CMV pneumonia in immunocompetent patients [5]. Gonçalves et al. described the case of a 29-year-old patient who developed interstitial pneumonia as a complication of CMV primary infection. He was treated successfully with ganciclovir. In this case, the direct role of CMV was inferred from detection of CMV by PCR in the blood and bronchoalveolar specimens and the resolution of clinical symptoms, hypoxemia, and pulmonary infiltrates following the institution of CMVspecific therapy [13].
In immunocompetent hosts, T cells play an important role in controlling viral replication and disease. Specific cytomegalovirus CD4+ and CD8+ T cell responses have been demonstrated [14]. Patients with SLE show numerous immune defects, of which etiology remains unclear. The ones who are not taking immunosuppressive drugs have a primary B-cells disorder and a dis-regulation of T-cells activity. Treatment with steroids or other immunosuppressant is mandatory to restore immunotolerance to self-antigens but increases the susceptibility to opportunistic infections [15,16].
Our case is unusual for some issues. Firstly, CMV pneumonia in immunocompromised people is typically described as an expression of reactivation of latent infection; in this case, it is expression of an acute infection, rarely described both in immunocompetent and immunocompromised patients [5]. Secondly, at the time of CMV infection the patient was not taking any strongly immunosuppressant medication, but only hydroxychloroquine, an immunomodulator which is not associated with an increased risk of infection [16]. In a meta-analysis performed by Yuan et al., administration of hydroxychloroquine resulted as a protective factor against infections in SLE patients [17]. Finally, our patient couldn’t even be considered as an immunocompetent person: she had persistent impaired immune response with an inverted CD4:CD8 ratio which has already been observed in other cases during CMV pneumonia, as an expression of transient or subclinical T-cell abnormality [5]. Previous studies have found either a normal or an increased level of CD8+ T cells and a decrease in CD4+ T cells, with a consequent decrease of the CD4/CD8 ratio, in patients with active SLE [18,19]: this laboratory abnormality could be seen as an expression of a dysregulating immune system even SLE was considered under remission. In our case, this inversion of CD4/CD8 ratio might have contributed to the severity of this acute infection and to the need of antiviral therapy to gain symptoms’ resolution and seroconversion. Inverted CD4/CD8 ratio might be considered as a risk factor for opportunistic infections in patients with rheumatic diseases even in absence of immunosuppressive therapy [20].
In hosts with autoimmune diseases, CMV may precipitate or exacerbate a flare of the rheumatic disorder, so acute CMV infection may result in de novo SLE or more commonly may precipitate a SLE flare [21]. It is quite important to recognize severe and symptomatic acute CMV infection in SLE patients and to start promptly an antiviral treatment to prevent worsening of the underlining disease. That diagnosis could be challenging because patients presenting with CMV and SLE have many overlapping features [22]. Atypical lymphocytes in the peripheral smear are a feature of CMV but not SLE. The liver is regularly involved in CMV infection but usually is spared in SLE. Therefore, the presence of mild to moderately elevated serum transaminases in a patient with SLE should suggest CMV rather than SLE with liver involvement [23].
In immunocompromised patients, importance of antiviral treatment with ganciclovir or valganciclovir at an early stage of virus reactivation has been strongly established [8]. On the other hand, no treatment is currently indicated for CMV infection in immunocompetent people. Some case series and reviews showed however a high fatality rate of untreated severe CMV infection even in previous healthy subjects [24]. Although limited, review of current literature suggests that targeted antiviral therapy with ganciclovir or valganciclovir is appropriate for severe CMV disease in immunocompetent adults [12]; in our case, antiviral treatment also didn’t affect regular seroconversion. In severely immunocompromised subjects who have developed tissue invasive CMV infection, prophylaxis with valganciclovir is prolonged until restoration of immune function [25]. We decided to interrupt antiviral therapy after completion of 21 days, and no prophylaxis was started; it is not possible to predict how a CMV reactivation can occur in our patient, and how to prevent it. More data are needed to establish which is the best way to clinically follow-up patients with rheumatic diseases who have developed a severe CMV primary infection.
Conclusion
In conclusion, CMV is an uncommon causative agent of pneumonitis. CMV pneumonia is more frequently a consequence of CMV reactivation in profoundly immunocompromised patients, such as transplant recipients or patients receiving high-dose corticosteroids. Our case demonstrate that pneumonia may also occur as a complication of CMV acute infection, in patients with immune system alterations due to systemic lupus erythematous. Recognize this unusual but potentially fatal infection is crucial to perform specific diagnostic tests and to start promptly a targeted therapy.
References
- Yuan Q, Xing X, Lu X, Li X. Clinical Characteristics and Risk Factors of Infection in Patients with Systemic Lupus Erythematosus: A Systematic Review and Meta-Analysis of Observational Studies. Semin. Arthritis Rheum. 2020; 50: 1022–1039.
- Krech U. Complement-fixing antibodies against Cytomegalovirus in different parts of the world. Bull World Health Organ. 1973; 49: 103–106.
- Klemola E, Kääriäinen L. Cytomegalovirus as a possible cause of a disease resembling infectious mononucleosis. Br Med J. 1965; 2: 1099.
- Eddleston M, Peacock S, Juniper M, Warrell DA. Severe cytomegalovirus infection in immunocompetent patients. Clin Infect Dis. 1997; 24: 52–56.
- Grilli E, Galati V, Bordi L, Taglietti F, Petrosillo N. Cytomegalovirus pneumonia in immunocompetent host: case report and literature review. J Clin Virol. 2012; 55(4): 356-359
- Sinclair J, Sissons P. Latency and Reactivation of Human Cytomegalovirus. J Gen Virol. 2006; 87(7): 1763–1779
- Bennett JE, Dolin R Mandell GL. Mandell, Douglas and Bennett’s principles and practice of infectious diseases. 4th edn. New York: Churchill Livingstone. 1995.
- Shahnaz S, Choksi MT, Tan IJ. Bilateral Cytomegalovirus retinitis in a patient with systemic lupus erythematosus and end-stage renal disease. Mayo Clin Proc. 2003; 78: 1412–1415.
- Xue Y, Jiang L, Wan WG, Chen YM, Zhang J, Zhang ZC. Cytomegalovirus Pneumonia in Patients with Rheumatic Diseases After Immunosuppressive Therapy: A Single Center Study in China. Chin Med J (Engl). 2016; 129(3): 267-273
- Griffiths P, Reeves M. Pathogenesis of human cytomegalovirus in the immunocompromised host. Nat Rev Microbiol. 2021; 19(12): 759-773
- Salomon N, Perlman DC. Cytomegalovirus pneumonia. Semin Respir Infect. 1999; 14(4): 353-358.
- Lai CC, Sun YS, Lin FC, Yang CY, Tsai CY. Bronchoalveolar lavage fluid analysis and mortality risk in systemic lupus erythematosus patients with pneumonia and respiratory failure. J Microbiol Immunol Infect. 2021; 54(6):1048-1055.
- Gonçalves C, Cipriano A, Videira Santos F, Abreu M, Méndez J, Sarmento, et al. Cytomegalovirus acute infection with pulmonary involvement in an immunocompetent patient. IDCases. 2018; 14
- Jackson SE, Mason GM, Wills MR. Human cytomegalovirus immunity and immune evasion. Virus Res. 2011; 157(2): 151-160
- Sekigawa I, Nawata M, Seta N, Yamada M, Iida N, Hashimoto H. Cytomegalovirus infection in patients with systemic lupus erythematosus. Clin Exp Rheumatol. 2002; 20(4): 559-564
- Durcan L, Petri M. Immunomodulators in SLE: Clinical evidence and immunologic actions. J Autoimmun. 2016; 74: 73-84
- Yuan Q, Xing X, Lu Z, Li X. Clinical Characteristics and Risk Factors of Infection in Patients with Systemic Lupus Erythematosus: A Systematic Review and Meta-Analysis of Observational Studies. Semin. Arthritis Rheum. 2020; 50: 1022–1039
- Bakke AC, Kirkland PA, Kitridou RC, Quismorio FP Jr, Rea T, Ehresmann GR, et al. T lymphocyte subsets in systemic lupus erythematosus. Correlations with corticosteroid therapy and disease activity. Arthritis Rheum 1983; 26: 745–750
- Maeda N, Sekigawa I, Iida N, Matsumoto M, Hashimoto H, Hirose S. Relationship between CD4+/CD8+ T cell ratio and T cell activation in systemic lupus erythematosus. Scand J Rheumatol. 1999; 28(3): 166-170
- Qin L, Qiu Z, Hsieh E, Geng T, Zhao J, Zeng X, et al. Association between lymphocyte subsets and cytomegalovirus infection status among patients with systemic lupus erythematosus: A pilot study. Medicine (Baltimore). 2019 Sep;98(39)
- Gugliesi F, Pasquero S, Griffante G, Scutera S, Albano C, Pacheco SFC, et al. Human Cytomegalovirus and Autoimmune Diseases: Where Are We? Viruses. 2021; 13(2): 260
- Doaty S, Agrawal H, Bauer E, Furst DE. Infection and Lupus: Which Causes Which? Curr Rheumatol Rep. 2016; 18(3): 13
- Cunha BA, Gouzhva O, Nausheen S. Severe cytomegalovirus (CMV) community-acquired pneumonia (CAP) precipitating a systemic lupus erythematosus (SLE) flare. Heart Lung. 2009; 38(3): 249-252
- Eddleston M, Peacock S, Juniper M, Warrell DA. Severe cytomegalovirus infection in immunocompetent patients. Clin Infect Dis. 1997; 24: 52–56
- Kotton CN. CMV: Prevention, Diagnosis and Therapy. Am J Transplant. 2013 Feb;13 Suppl 3:24-40.
