
Open Access, Volume 10
Lymphoma’s last therapeutic option: Freeze it!
Giulia Bassi1,3; Maria Beatrice Ferrari1,3; Angelo Vanzulli2; Silvia Cantoni1; Roberto Cairoli1,3*
1Hematology Division ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
2Radiology Division, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
3Medicine Department, Milano Bicocca University, Milan, Italy.
Roberto Cairoli
Hematology Division ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
Email: roberto.cairoli@ospedaleniguarda.it
Received : Jan 31, 2024,
Accepted : Feb 20, 2024
Published : Feb 28, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Cryoablation has been used for removal of solid cancers in selected settings. We describe its application in a patient who was diagnosed with diffuse large cell lymphoma. A residual lymphoma lesion involving the right adrenal gland, still PET-positive after multiple lines of chemotherapy, was eradicated with the use of cryoablation. The patient is alive and in complete response at last follow-up, over 4 years from the procedure. Our data suggest that cryoablation may have a role also in the setting of lymphoma.
Keywords: Diffuse large B cell lymphoma; Cryoablation; Rescue therapy; Abdominal lymphoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Cairoli R (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Bassi G, Ferrari MB, Vanzulli A, Cantoni S, Cairoli R. Lymphoma’s last therapeutic option: Freeze it!. Open J Clin Med Case Rep. 2024; 2202.
Introduction
Use of cryoablation has been proposed as a cancer removal option in selected settings such as removal of small, unresectable lesions and in patients unfit for invasive surgical options [1,2]. Its application spans over a wide range of solid neoplasms such as liver, prostate, breast, skin and renal cancers [1,2]. We report on a patient with Diffuse Large B Cell Lymphoma (DLBCL) in whom cryoablation was used to eradicate residual disease involving the right adrenal gland.
Case Presentation
This female patient was diagnosed with DLBCL GC-type in February 2018, at the age of 71 years. At diagnosis, imaging was consistent with stage IV-EA disease involving thoracic and abdominal lymph nodes, spleen, right kidney with adrenal gland infiltrate and bone marrow. She received 6 courses of R-CHOP (rituximab-Cyclophosphamide, Adriamycin, Vincristine, Prednisone) as first line chemotherapy and central nervous system prophylaxis by lumbar puncture. In August 2018 imaging revaluation showed persistent disease involving the right kidney and she received 2 courses R-DHAP (RTX, Cysplatin, Cytarabine, Dexamethasone) as second line treatment. PBSC were also collected. In October 2018 progression of pathological right adrenal tissue was documented and in November 2018 she underwent Autologous Stem Cells Transplant (ACST) with Beam conditioning regimen (Carmustine, Etoposide, Cytarabine, Melphalan).
PET imaging after ACST showed residual, albeit significantly reduced, pathological tissue solely localized to the right adrenal gland and in January 2019 the patient received 30 Gy involved field radiotherapy. Nevertheless, the adrenal gland involvement was still visible at control PET evaluation in March 2019.
Therapeutic options were considered. Additional radiotherapy was not considered feasible, and use of radiofrequency was not applicable since the residual pathological tissue was too close to vessels which could have been damaged by the procedure (Figures 1-3).
Therefore, a tentative trial with cryoablation was carried out. The patient underwent the procedure in May 2019 and no immediate or late complications were recorded. First re-evaluation was in July 2019, two months after the procedure, which showed a consistent decrease of the known pathological residual tissue. Follow up imaging confirmed remission. The patient is alive and well still in complete remission at last follow-up as of November 2023.
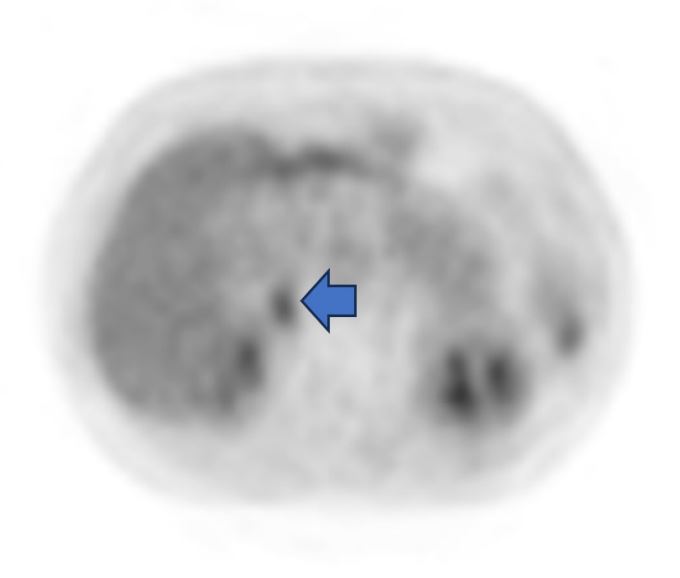
Figure 1: FDG–PET scan before treatment: The arrow
shows the lesion in the right adrenal gland.

Figure 2: CT scan during the cryoablation procedure.
The needle tip is placed within the lesion.
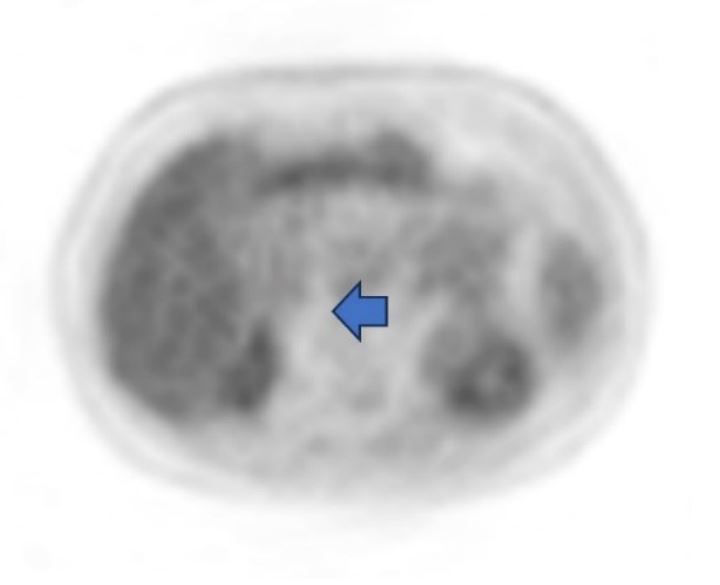
Figure 3: FDG–PET scan after treatment: The arrow shows absence of
FDG uptake in the right adrenal gland.
Discussion
The term cryoablation refers to the application of exceedingly low temperatures to the target tumor site with the aim of selectively damaging the malignant cells while sparing as much normal surrounding tissue as possible.Its efficacy exploits the use of high pressured gas, such as Argon. This process consists in the application of the Joules-Thompson effect: the gas medium flows high-pressured through a small opening, forcing the rapid expansion of the gas. This in turn results in heat absorption from the cancer invaded tissue, decreasing its temperature below -140°C, and consequently causing the formation of ice crystals inside and outside the tumor cells. The technique is usually performed percutaneously [1].
Cell death is achieved through multiple mechanisms. The main one exploits the mechanically induced cell membrane disruption caused by ice crystal formation within the cell. Additionally, the freezing-thawing process leads to the occlusion of micro vessels which results in the stress-based mitochondrial response that triggers apoptosis [2]. To our knowledge, cryoablation has not been previously used in patients with lymphoma. However, it proved to be safe and effective in bringing about complete and long-lasting remission in this multi refractory patient. Compared to other existing modalities (e.g. radiofrequency), cryoablation has several advantages: imaging-oriented control of the ablation zone, sharpness in edge definition, pain relief properties [3].
Moreover, cell necrosis - with exposure of intracellular tumor antigens - has the potential to trigger the autologous antitumor immune response which may have an additive role in residual tumor cell clearance [4]. As for other cancers, cryoablation may have a role in eradicating residual disease in specific settings also in patients with lymphoma.
References
- Chen Z, Meng L, Zhang J, Zhang X. Progress in the cryoablation and cryoimmunotherapy for tumor. Front Immunol. 2023; 14: 1094009.
- Kwak K, Yu B, Lewandowski RJ, Kim DH. Recent progress in cryoablation cancer therapy and nanoparticles mediated cryoablation. Theranostics. 2022; 12(5): 2175-2204.
- Yan S, Yang W, Zhu CM, Yan PM, Wang ZC. Comparison among cryoablation, radiofrequency ablation, and partial nephrectomy for renal cell carcinomas sized smaller than 2 cm or sized 2-4 cm. Medicine (Baltimore). 2019; 98(21): e15610.
- Simmons RM, Ballman K V, Cox C, et al. A Phase II Trial Exploring the Success of Cryoablation Therapy in the Treatment of Invasive Breast Carcinoma: Results from ACOSOG (Alliance) Z1072. Ann Surg Oncol. 2016; 23(8): 2438-2445.
