
Open Access, Volume 10
Cytomegalovirus pericarditis as a triggering factor for macrophage activation syndrome in a patient with systemic lupus erythematosus: Case report and review of the literature
Ticiane Araruna Cruz1; Maria Tayanne Parente Barbosa1; Gilberto Loiola de Vaconcelos1; Daniel Teixeira da Silva1; Lysiane Maria Adeodato Ramos2; Andrea Rocha de Saboia Mont’Alverne3; Carlos Ewerton Maia Rodrigues4*
1Resident in Rheumatology, Hospital Geral de Fortaleza, Ceará, Brazil.
2Master’s in Medical Sciences, Postgraduate Program, University of Fortaleza (Unifor), Fortaleza, Brazil.
3Professor at University of Fortaleza (Unifor), Fortaleza, Brazil.
4Graduate Program in Medical Sciences, Universidade de Fortaleza (Unifor), Fortaleza, Brazil.
Carlos Ewerton Maia Rodrigues
Graduate Program in Medical Sciences, Universidade de Fortaleza (Unifor), Fortaleza, Brazil.
Tel: +55-85-34773846;
Email: carlosewerton@hotmail.com
Received : Jan 24, 2024,
Accepted : Feb 16, 2024
Published : Feb 28, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Macrophage Activation Syndrome (MAS) is a form of lymphohistiocytosis occurring in autoimmune diseases. Viral infections, including Cytomegalovirus (CMV), are major triggers of MAS and require specific treatment. We report a rare case of a 25-year old woman with persistent fever and clinical and lab findings Suggestive of Lupus (SLE). The patient experienced MAS and pericarditis refractory to immunosuppression and was later diagnosed with active CMV infection, identified as a trigger factor. Treatment with ganciclovir and maintenance of immunosuppression led to complete and sustained recovery. Only five other patients with SLE associated with MAS and CMV have been reported in the literature, with information on clinical findings, diagnostic methods and outcomes. The mean age of the reviewed cases was 22-58 years, the female sex was predominant, but only half the cases had a previous diagnosis of SLE. All patients improved with ganciclovir and only one death occurred due to hemorrhagic complications from colon ulcer. These outcomes highlight the importance of screening for CMV in this patient population.
Keywords: Lupus; Hemophagocytosis; CMV
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Rodrigues CEM (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Cruz TA, Barbosa MTP, Vaconcelos GLD, Silva DTD, Ramos LMA, Mont’Alverne ARS, Rodrigues CEM. Cytomegalovirus pericarditis as a triggering factor for macrophage activation syndrome in a patient with systemic lupus erythematosus: Case report and review of the literature. Open J Clin Med Case Rep. 2024; 2201.
Introduction
Systemic Lupus Erythematosus (SLE) is a multisystem disease with alternating periods of activity and remission. In the clinical setting, distinguishing between an exacerbation of SLE and infectious disease requires very careful observation and ample differential diagnosis. This may delay treatment for SLE and expose the patient to unnecessary antibiotic therapies and procedures.
Cytomegalovirus (CMV), a DNA virus of the family Herpesviridae, is associated with a wide spectrum of manifestations, depending on the patient’s immunological profile. In immunocompetent patients, manifestations range from asymptomatic to hepatitis or mononucleosis, while immunocompromised patients are at risk of systemic disease and even death [1]. SLE is also known to be associated with CVM infection or reactivation of latent CMV. For example, in one study, PP65 antigenemia was observed in 36.8% of hospitalized SLE patients with infection of unknown origin [2].
Macrophage Activation Syndrome (MAS) is part of the Lymphohistiocytosis (LH) spectrum. The condition is referred to as MAS when secondary to or associated with autoimmune diseases, such as Still’s disease, vasculitis and SLE [3,4]. MAS is believed to be underdiagnosed, potentially increasing mortality. The most common clinical and laboratory findings are persistent fever, hyperferritinemia, pancytopenia, coagulopathy, liver dysfunction and the proliferation of activated macrophages in hematopoietic organs [5- 7]. Herpesviruses, especially Epstein-Barr Virus (EBV) and CMV, are important triggers of MAS, whether or not the condition is associated with SLE [5].
To our knowledge, only five other patients with SLE associated with MAS and CMV have been reported in the literature [1,5,8,9,11]. In one case, a patient with prolonged fever, pericarditis, pneumonia, clinical criteria for SLE and seropositivity for CMV was admitted and treated with corticoids and ganciclovir, followed by rapid clinical improvement [8]. In this paper we report a similar case of SLE with MAS and CMV-induced pericarditis and review the literature on this rare association.
Material and Methods
Case report: Descriptive, cross-sectional study of the medical record of a female patient treated at Hospital Geral de Fortaleza between December 2022 and January 2023.
Review of the literature: A non-date-filtered search was conducted on the platforms Capes, Ebsco, Pubmed, BVS, Science Direct, Scielo and Google Scholar, using the key words ‘cytomegalovirus’, ‘hemophagocytic syndrome’, ‘macrophage activation syndrome’ and ‘systemic lupus erythematosus’. Five reports were identified which describe the association of SLE, CMV and MAS, along with information on clinical manifestations, patient profile, previous immunosuppression, method of CMV diagnosis, MAS diagnosis, treatment administered, and clinical outcome.
Case presentation: A 26-year old female patient with no known comorbidities was admitted to Hospital Geral de Fortaleza in December 2022. Starting in July 2022, the early symptoms included adynamia, hyporexia, allopecia, and weight loss (10 kg). Upon a medical examination in October 2022, normocytic and normochromic anemia was observed (hemoglobin: 11.1 g/d), but the patient was prescribed iron sulfate and discharged. In November 2022, new symptoms developed, including paleness, tachycardia, moderate ice pick headache, nausea, vomiting, three fever spells (39°C) per week, and inflammatory joint pain in the hands. Lab testing showed a worsening of the anemia. Presenting fever, tachycardia and tachypnea, the patient was hospitalized for investigation in December 2022. Pneumonia was diagnosed and the patient was started on ceftriaxone and azithromycin (subsequently replaced with Cefepime). Lab testing for anemia suggested hemolytic anemia (Table 1, Column 1). Pulse therapy with methylprednisolone (1 g/day) was administered from 15 to 17 December, followed by prednisone at 40 mg/day. The chest tomography showed signs of congestion, slight pericardial effusion, and cardiomegaly. The abdominal tomography revealed multiple enlarged lymph nodes (up to 2x1.8 cm) in the peri-aorthocaval, iliac and inguinal regions, in addition to mild hepatosplenomegaly. The finding of cardiomegaly, tachycardia and congestion raised suspicion of myocarditis. After five days in the ICU for respiratory management, the patient was transferred to the rheumatology service for further diagnostic investigation.
On 18 December, the patient was admitted to our service, without fever and having completed the prescribed regime of antibiotics. Lab testing supported the diagnosis of SLE (Table 1, Column 2), with normal ECG findings, but tachycardia persisted despite the good overall condition and the absence of symptoms. No muscle weakness was detected on physical examination, but electroneuromyography was performed to investigate the high level of Creatine Phosphokinase (CPK), revealing mild to moderate proximal myopathic involvement, with signs of spontaneous activity, including in the paravertebral muscles. To rule out lymphoproliferative disease, a lymph node biopsy was done suggestive of SLE-related lymphadenitis. Immunosuppressive therapy with cyclophosphamide 500 mg was initiated on 24 December 2022, justified by the presence of hematological and renal activity, myopathy and myocarditis.
Table 1:
| Column 1 | Column 2 | Column 3 | |
|---|---|---|---|
| Hemoglobin | 5.3 g/d | 6.5 g/d | 6.0 g/d |
| Leukocytes | 16,500/mm³ | 18,600/mm³ | 3,900/mm³ |
| Neutrophils | 14,136/mm³ | 2,714/mm³ | |
| Lymphocytes | 3,348/mm³ | 742/mm³ | |
| Platelets | 293,000/mm³ | 333,000 mm³ | 319,000/mm³ |
| Urea | 22 mg/dL | 71 mg/dL | 66 mg/dL |
| Creatinine | 1.1 mg/dL | 0.77 mg/dL | 2.03 mg/dL |
| AST | 419 U/L | 308 U/L | 722 U/L |
| ALT | 126 U/L | 213 U/L | |
| CPK | 4708 U/L | 7374 U/L | |
| ESR | 150 | ||
| Troponin | 340 ng/L | ||
| Direct Coombs test | Positive | Positive | |
| Haptoglobin | 7.25 mg/dL | ||
| Bilirubin total / direct / indirect | 0.62 / 0.14 / 0.48 mg/dL | ||
| Reticulocytes | 228,600/mm³ | ||
| Antinuclear factor | 1/640 fine speckled nuclear pattern | ||
| C3 | 30.2 | ||
| C4 | 1.88 | ||
| Proteinuria 24 h | 2,646 mg/24 h | ||
| Urinalysis | Proteins 2+, 25 RBCs, 10 leukocytes | ||
| Anti-DNA | Reactive | ||
| Anti-SM | 106 | ||
| Anticardiolipin IGM/IGG | 43.5/133 | ||
| Lupus anticoagulant | Negative | ||
| Ferritin | 2,818 ng/mL | >15,000 ng/mL | |
| Triglycerides | 615 mg/dL | 491 mg/dL | |
| LDH | 3,115 U/L | 1,638 U/L | 3,404 U/L |
| Fibrinogen | 215 mg/dL | ||
| Anti-HIV | Non-reactive | ||
| VDRL | ¼ | ||
| Anti-HCV | Non-reactive | ||
| HbsAg | Non-reactive | ||
| EBV IGM/IGG | Non-reactive/Reactive | ||
| CMV IGM/IGG | Non-reactive/Reactive |
One day after the cyclophosphamide pulse, the pattern of daily fever spells resumed, at short intervals. The patient was initially asymptomatic and much effort was made to identify a possible source of infection. Hemoculture and uroculture were negative and the transthoracic ECG showed normal ventricular function, although a mild to moderate pericardial effusion without vegetations was observed. After two weeks of daily fever, without clinical complaints, and despite treatment with meropenem and vancomycin, the patient’s overall condition worsened, with changes in renal function and need for supplemental nasal oxygen therapy. The bone marrow fluid showed signs of hemophagocytosis, but was negative for parasites and neoplastic cells (Figure 1). A new series of laboratory tests (Table 1, Column 3), along with the findings of hepatosplenomegaly and hemophagocytosis, suggested a diagnosis of MAS. The patient also experienced precordial pain on effort, aggravated by movement, and the ECG displayed diffuse ST segment elevation and PR segment depression in D2 (Figure 2) compatible with pericarditis, despite the use of prednisone 40 mg/day for one month and immunosuppression with cyclophosphamide for 15 days. At this point, another 3-day pulse therapy with methylprednisolone 500 mg was administered. Some clinical improvement was observed, but the fever and tachycardia persisted.
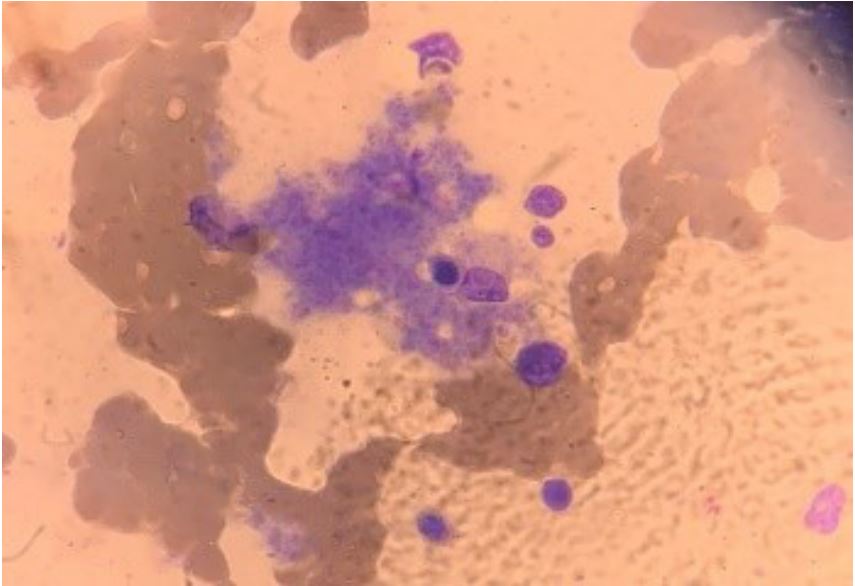
Figure 1: Aspired bone marrow fluid with signs of hemophagocytic
activity.
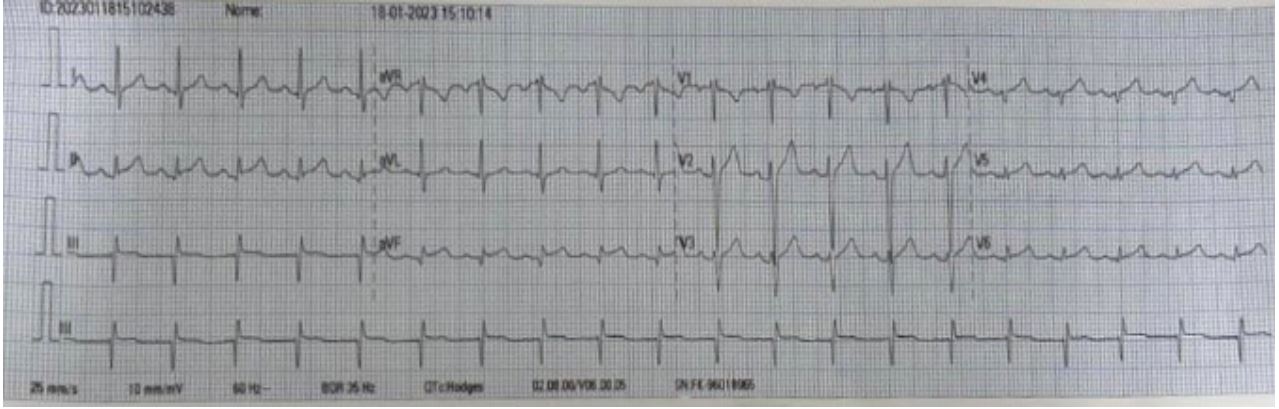
Figure 2: ECG showing diffuse ST segment elevation and PR segment depression in D2, compatible with pericarditis.
When MAS and pericarditis manifest during immunosuppression, the triggering factors should be carefully investigated. We therefore decided to measure the viral load, despite IGM seronegativity for CMV. The result (88,000 copies) pointed to CMV-induced pericarditis. Esophagogastroduodenoscopy and fundus examination yielded no signs of CMV infection, so the patient was started on a 21-day regime of ganciclovir which resolved the fever. Four weeks later, another course of cyclophosphamide pulse therapy was administered. The patient was subsequently discharged with considerable improvement of laboratory findings and recovered renal function. At the time of writing (one month of follow-up), no clinical complaints have come to our knowledge.
Results
Our review of the literature only identified five other patients with SLE associated with MAS and CMV, reported between 2002 and 2023. All the search results were eligible, indicating that the present review is representative of the literature. The clinical and laboratory findings of all known cases are shown in Table 2.
The patients described in Table 2 were aged 22-58 years, with a clear predominance of the female sex (80%), as expected for SLE patients. In three cases, SLE had not been previously diagnosed, thus no immunosuppression therapy had been administered. In one case with previously diagnosed SLE, no information was provided on immunosuppression. The remaining two cases used corticosteroids combined with azathioprine (n=1) or cyclophosphamide (n=1).
The clinical manifestations varied, but all patients had fever. The second-most prevalent manifestation was pancytopenia (n=4), while pericarditis was observed in only one patient. MAS was diagnosed by myelography except in one case, and ferritin and lactate dehydrogenase levels were significantly increased in all the cases for which this information was available.
CMV was diagnosed by PCR in most cases. A single case was positive on serology and non-reactive on PCR. Response to ganciclovir was invariably good. One death occurred due to bleeding from a sigmoid colon ulcer in a patient otherwise recovering after antiviral therapy. Four of the six cases (4/6) experienced complete recovery, and one died (1/6). The outcome of the sixth case was not reported (Table 2).
Table 2: Six known clinical cases of systemic lupus erythematosus with hemophagocytic syndrome associated with cy- tomegalovirus infection.
|
Clinical manifestations |
Patient profile |
Previous immuno suppression |
Diagnosis of MAS |
Method of CMV diagnosis |
Treatment for CMV | Outcome | |
|---|---|---|---|---|---|---|---|
| Cruz et al. 2023 |
Fever Lymphadenopathy Hepatosplenomegaly Pericarditis |
Female 26 years No previous diagnosis of SLE |
No |
AST 722 U/L, ALT 213 U/L, Ferritin>15,000 ng/mL Triglycerides 615 mg/dL BM: signs of hemophagocytosis, negative for parasites and neoplastic cells |
IgM antibodies negative, IgG antibodies positive PCR for CMV: 88,000 mil copies |
Ganciclovir 21 days Methylprednisolone pulse therapy |
Improvement |
| Kwon et al. 2007 |
Pericarditis Pleural effusion Fever |
Male 25 years No previous diagnosis of SLE |
No |
AST 1,023 U/L, ALT 546
U/L, LDH 409 U/l, triglycerides 120 mg/dL Ferritin 1,410.42 ng/mL BM: histiocytes increased in number (4%) with marrow aspirate showing hemophagocytosis |
IgM and IgG antibodies positive Non-reactive PCR qualitative and pp65 |
Ganciclovir 5 mg/kg Dexamethasone 20 mg/d |
Improvement |
| Tanaka et al. 2008 |
Fever Flu-like symptoms Pancytopenia Splenomegaly Pneumonia |
Female 58 years Previous diagnosis of SLE and APS |
Azathioprine 50 mg/d Methylprednisolone pulse therapy |
LDH 498 UI/L Mild hepatobiliary disorder Ferritin 3,285 ng/m BM: erythrocytes and platelets phagocytized by macrophages |
Antigenemia positive for CMV |
Ganciclovir 500 mg/d for 2 weeks Prednisolone 20 mg/d |
Improvement |
| Awasthi et al. 2020 |
Fever Lymphadenopathy Pneumonia Hepatosplenomegaly Pancytopenia |
Female 50 years Previous diagnosis of SLE and Sjögren |
Not informed |
Increase in liver enzymes Ferritin 5,098 ng/mL ESR 138 LDH 1,116 UI/L CD25 24,885 pg/mL MO: not performed |
PCR CMV >300,000 copies/mL PCR EBV >20,00000 copies/mL |
Ganciclovir High doses of corticoids IVIG Chemoimmunotherapy |
Not informed |
| Sakamoto et al. 2002 |
Fever Pancytopenia Intestinal bleeding |
Female 44 years SLE chronic active hepatitis C |
Prednisolone 30 mg/d Cyclophosphamide 50 mg/d |
Ferritin 2,590 ng/mL LDH 415 UI/L BM: histiocytes with benign appearance scattered in BM, indicating phagocytosis of erythrocytes, erythroblasts, leukocytes and platelets Autopsy with presence of hemophagocytic histiocytes in liver, BM, kidneys, pancreas and colon |
CMV antigen positive Colon biopsy positive for CMV Autopsy showing CMV in liver and pancreas |
Methylprednisolone 1 g/d for 3 days followed by prednisone 60 mg/d Ganciclovir Immunoglobulin for CMV |
Death |
| Amel et al. 2016 |
Skin rash Arthralgia Fever Myalgia Seizure |
Female 22 years No previous diagnosis of SLE |
No |
Pancytopenia Changes in liver function BM: hemophagocytosis |
IgM serology positive Antigenemia positive for CMV |
IVIG Ganciclovir Corticosteroids |
Improvement |
SLE: Systemic Lupus Erythematosus; CD25: Soluble Interleukin-2 Receptor Alpha Chain; AST: Aspartate Transaminase; ALT: Alanine Transaminase; CMV: Cytomegalovirus; BM: Bone Marrow; LDH: Lactate Dehydrogenase; APS: Antiphospholipid Antibody Syndrome; IVIG: Intravenous Human Immunoglobulin.
Discussion
We report a case of MAS in an SLE patient with CMV infection. The diagnosis was challenging since, due to clinical similarities, the infection was masked by the activity of the recently discovered SLE. To our knowledge, only five other cases have been reported in the literature, suggesting the condition is very rare and/or difficult to diagnose.
LH is defined as the activation of histiocytes, with prominent hemophagocytosis in the bone marrow and other reticuloendothelial systems [7]. The primary form is the most common, affecting preferentially children, with a strong genetic component. The secondary form is associated with malignancy, infection and autoinflammatory or autoimmune diseases. When associated with the latter, LH is referered to as MAS [3,4]. The prevalence of MAS in SLE patients is between 0.9% and 9%, nearly half of which (46%) is observed concomitantly with the first flare of the disease [3].
The physiopathology of MAS involves immune system deregulation, with compromised interaction between natural killer cells, cytotoxic T cells and their targets. Changes in the mechanism of target cell degradation and the inability of the organism to neutralize the antigen trigger an increase in the recruitment of cytotoxic cells and cytokines, leading to the activation of macrophages and hemophagocytosis and an exacerbated inflammatory response. Innate immune dysfunction involving IL-1 appears to be central to the development of MAS [3].
Infections are often associated with LH, whether as primary cause or as a trigger along with other pathologies. Herpesviruses are important triggers of hemophagocytosis and should screened for when diagnosing a disease of undetermined origin. EBV is the most frequently associated infection, but CMV is a major trigger as well [5]. In patients with MAS, trigger factors are variable, but infections are very common [4].
CMV infection is known to be highly prevalent in SLE patients but is often only diagnosed after the appearance of unfavorable outcomes. This may be due to the unavailability of diagnostic methods and/or similarities between the clinical manifestations of CMV infection and SLE during flares [2,5].
In the case reported here, diagnosis and treatment of CMV were delayed due to a negative serology for IgM. However, CMV was reconsidered when the fever persisted and pericarditis was refractory to immunosuppression. Only one other case in the literature reported a discrepancy between diagnostic tests (positive on serology and non-reactive on PCR). This was attributed by the author to the initial stage of the infection and a possible host defense mechanism. No such difficulty was reported in any of the remaining cases [8].
CMV infection may be detected by serology, culture, antigenemia, histopathology and PCR techniques. In immunocompromised patients, the latter appear to be reliable and to correlate well with severity and treatment response [2,10]. Antigenemia detects the CMV pp65 antigen in circulating leukocytes of fresh anticoagulated blood or spinal fluid during the initial period of CMV replication, but interpretation is subjective and the method requires leukocyte-rich samples, making it unsuitable for patients with neutropenia [10]. It should be stressed that a negative serology does not rule out a diagnosis of CMV.
In immunocompromised patients, clinical manifestations of CMV can reach the level of systemic disease (including hepatitis, interstitial pneumonia, encefalitis, retinitis and enteritis), not infrequently resulting in death [1]. In two of the patients in Table 2, pneumonia led to the suspicion of CMV [5,9]. Though not a commonly reported manifestation of CMV, pericarditis was observed in two cases (one of which our own), representing 40% of the reported cases of MAS in SLE patients infected with CMV [8].
Corticosteroids are considered the first-line therapy for MAS, the specific recommendation being methylprednisolone pulse therapy. If the immediate response is unsatisfactory, anakinra (an IL-1 blocker) may be tried. If, despite the initial treatment, the patient experiences severe disease or central nervous system involvement, etoposide (a chemotherapy drug widely used to treat other forms of LH) is indicated [3,4].
When MAS is triggered by infection, the approach should include treatment of the underlying infection [5]. Ganciclovir is the most frequently cited drug, with good response in all the reviewed cases [1,5,8,9,11]. In addition, immunoglobulin has been used to treat MAS in this population.
MAS is associated with high mortality in patients with autoimmune conditions (5-39%), and high ferritin levels, old age and malignancy are aggravating factors [3]. However, based on our review, when associated with CMV in SLE patients, MAS tends to have a better outcome. In any case, the fact that 80% of the cases discussed experienced complete recovery suggests that early diagnosis of CMV infection favors response to treatment.
Conclusion
CMV infection is an important trigger of a range of disorders and is highly prevalent in SLE, a fact not all physicians are aware of. Thus, we recommend scanning for CMV on PCR in MAS patients with atypical manifestations, considering that treatment with ganciclovir can improve the prognosis and reduce morbidity and mortality in this population.
In the case reported here we believe MAS was triggered by CMV infection since no significant improvement had been achieved with immunosuppression for SLE and in view of the rapid resolution of MAS following the onset of antiviral therapy.
Declarations
Competing interests: The authors have no conflicts of interest to disclose regarding the publication of this paper.
Disclaimer: No part of the manuscript contains text or tables published elsewhere.
Authors’ contributions
All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version submitted for publication. Dr. Rodrigues had full access to all study data and takes responsibility for the integrity of the data.
Study conception and design: TAC and CEMR.
Acquisition of data: TAC, MTPB, GLV, DTS, LMAR, ARSM, CEMR.
Analysis and interpretation of data: TAC, MTPB, GLV, DTS, LMAR, ARSM, CEMR.
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
References
- Sakamoto O, et al. Systemic lupus erythematosus complicated by cytomegalovirus-induced hemophagocytic syndrome and colitis. Internal medicine. 2002; 41: 151-155.
- Lino K, et al. Pp65 antigenemia and cytomegalovirus diagnosis in patients with lupus nephritis: Report os a series. Braz. J. Nephrol. 2018; 40: 44-52.
- Carter S J, et al. Macrophage activation syndrome in adults: Recent advances in pathophysiology, diagnosis and treatment. Rheumatology (Oxford, England). 2019; 58: 5-17.
- La Rosée P, et al. Recommendations for the management of hem phagocytic lymphohistiocytosis in adults. Blood. 2019; 133: 2465-2477.
- Awasthi S, Upretim S. Macrophage activation syndrome in a patient with Systemic Lupus Erythematosus (SLE) and dual viremia, Journal of Community Hospital Internal Medicine Perspectives. 2020; 10: 470-474.
- Castillo JE, et al. Systemic. Lupus Erythematosus and Its Association with Hem phagocytic Syndrome as an Initial Manifestation, Maedica. 2020; 15: 556-560.
- Kumakura S, et al. Autoimmune-associated hem phagocytic syndrome. Modern rheumatology. 2004; 14(3): 205-215.
- Kwon C M, et al. A case of acute pericarditis with hem phagocytic syndrome, cytomegalovirus infection and systemic lupus erythematosus. Rheumatology international.2008; 28: 271-273.
- Tanaka Y, et al. Systemic lupus erythematosus complicated by cytomegalovirus-induced hem phagocytic syndrome and pneumonia. Nihon Rinsho Men’eki Gakkai kaishi=Japanese journal of clinical immunology. 2008; 31: 71-75.
- Razonable, Raymund, et al. Clinical Diagnostic Testing for Human Cytomegalovirus Infections. The Journal of infectious diseases. 2020; 221: S74-S85.
- Amel R, et al. Systemic lupus erythematous revealed by cytomegalovirus infection. The Pan African Medical Journal. 2016; 24: 241.
