
Open Access, Volume 10
Giant osteochondroma of the scapula: Rare localization
Zied Mansi1*; Abdelkader Tounsi1; Aymen Ben Mahmoud1; Mahmoudi Ahmed; Wajdi Chermiti2; Haggui Ali3; Zaidi Bacem4
1Department of Orthopedic Surgery, Ibn El Jazzar University Hospital, Kairouan, Tunisia.
2Department of Orthopedic Surgery, Sahloul University Hospital, Sousse, Tunisia.
3Department of Orthopedic Surgery, Hospital of Kasserine, Kasserine, Tunisia.
4Department of General Surgery, Ibn El Jazzar University Hospital, Kairouan, Tunisia.
Zied Mansi
Department of Orthopaedic Surgery, Ibn El Jazzar Kairouan University Hospital 3100 Kairouan, Tunisia.
Email: doc.zm@htmail.fr
Received : Jan 22, 2024,
Accepted : Feb 07, 2024
Published : Feb 09, 2024,
Archived : www.jclinmedcasereports.com
Abstract
We report the case of an osteochondroma of the scapula with a radiological appearance and an unusual location in a 24-year-old young man who consulted for a deformity of his left shoulder with a posterior bump pushing back his scapula. A standard radiological assessment showed a pedunculated exostosis at the upper part of the scapula. The CT scan was in favor of a large exostosis.
Surgical resection of the tumor and pathological examination confirmed the diagnosis of an osteochondroma. After a follow-up of ten months, the functional results were very good.
Keywords: Scapula; Osteochondromatosis; Bulky.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Zied M (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Mansi Z, Tounsi A, Mahmoud AB, Ahmed M, Chermiti W, et al. Giant osteochondroma of the scapula: Rare localization. Open J Clin Med Case Rep. 2024; 2199.
Introduction
Exostosis, also called osteochondroma, corresponds to a bony outgrowth covered by a cartilaginous cap [1]. It is the most common benign bone tumor and represents approximately 35% of all benign bone tumors. In the majority of cases, it is localized to the epiphyses of the long bones, especially the femur and the humerus. Location on the scapula is rare, particularly on the dorsal side.
Case Report
A 24-year-old young man was presented for consultation for a mass on the dorsal side of the scapula that had been present for 3 years. This mass was hard, non-painful and slightly mobile; the scapula formed a voluminous dorsal hump 12 cm long, 8 cm wide and 5 cm thick (Figure 1). This mass led to fatigability of the shoulder during exercise, a limitation of particularly active shoulder joint movements and great aesthetic discomfort. The standard front x-ray of the scapula revealed heterogeneous bone formation at the spinal edge of the scapula (Figure 2). A CT scan confirmed the presence of the large exostosis, the boundaries of which appear regular and corticalized (Figure 3). The patient underwent surgery, with en bloc resection of the tumor and extraction of the detached fragments (Figure 4). The pathological examination concluded that it was an osteochondroma.
Postoperatively, the patient benefited from a rehabilitation program aimed at achieving pain relief, recovery of joint range of motion and strength of the shoulder muscles. Six months post-operatively, the patient returned to work without incident and no recurrence was noted after 10 months.

Figure 1: Clinical appearance of the tumor pushing the
scapula backward.
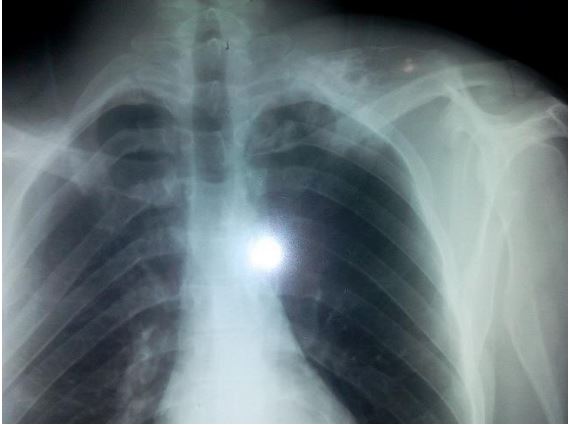
Figure 2: Radiological appearance of pedunculated osteochondroma at the edge spinal of the scapula..
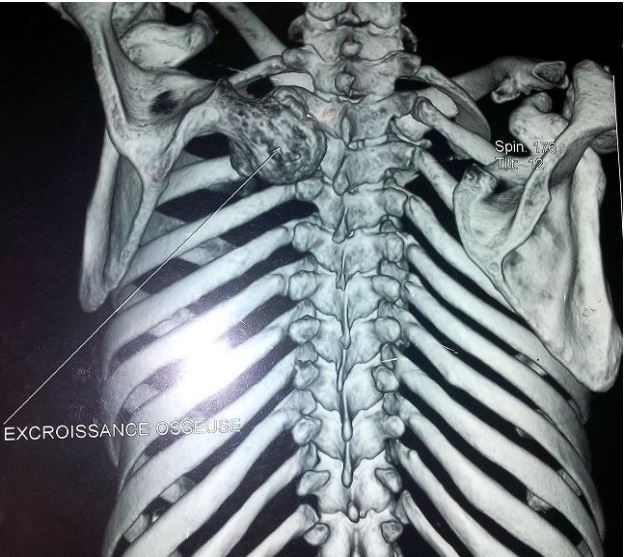
Figure 3: Scannographic appearance of osteochondroma
of the scapula.
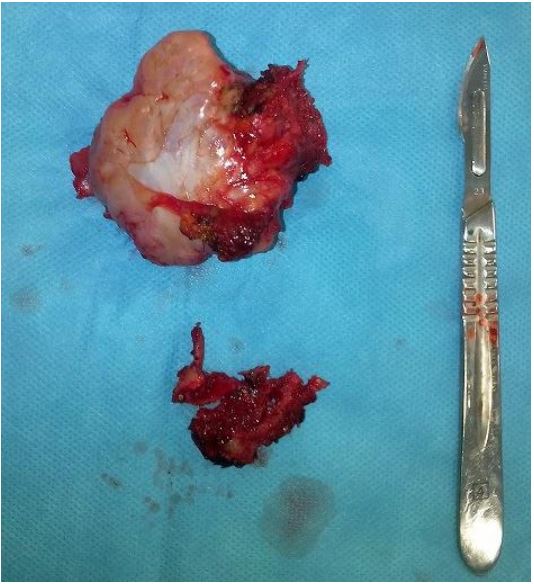
Figure 4: Macroscopic appearance of osteochondroma.
Discussion
Osteochondroma constitutes 35% of benign bone tumors and 8.5% of all bone tumors [2]. They often occur in adolescents and rarely in newborns. We know two clinical forms: solitary exostoses and the disease exostosis [3,4]. For solitary exostosis, there is no difference between the two sexes. On the other hand, exostosing disease affects men more frequently. It most often affects the metaphyses of the long bones (femur, humerus and tibia). These areas have the most bone growth activity. Localization to flat bones is possible, but remains very rare. At the level of the scapula, osteochondroma is the most common primary tumor common, with an incidence of 4.6%. It is most often located on the anterior surface of the bone, which leads to mechanical complications [5]. Thus H; Tomo et al. Reported a case of deformation of the rib cage following an osteochondroma of the anterior surface of the scapula [6]. Other complications have been reported in the literature: the most frequently cited is bursitis, which is manifested by pain and reduced mobility of the shoulder [7]. The diagnosis of osteochondroma is easy to make, because standard radiological imaging data are sufficient to confirm the diagnosis. However, in rare cases, due to the location, volume or atypical radiological appearance of the tumor, the use of CT scanning, or even a biopsy, proves necessary. In our patient, the volume and radiological appearance of the tumor as well as the young age justified a surgical biopsy before total excision of the tumor. Surgical treatment is indicated in cases of symptomatic osteochondroma, which is aesthetically bothersome, or in cases of suspected malignancy. The excision must be carried out as completely as possible while preserving as much as possible the integrity of the bone, the site of the lesion. The risk of degeneration is 1-2% in solitary exostosis [8] and 10-20% in exostotic disease [9]. The risk of malignant transformation is very low in the event of a single lesion (1 to 2% of cases). This risk is 5 to 25% in the event of multiple lesions. In the majority of cases, the prognosis after surgery is excellent, with rapid disappearance of symptoms. The appearance of certain signs should make us fear a malignant transformation, namely the increase in the size of the tumor; the appearance of osteolysis; the blurred appearance of the edges of the exostosis; the presence of calcifications outside the main ossification; erosion of the supporting bone or neighboring bone; a thickness of more than 1 cm of the cartilage cap and scintigraphic hyperuptake in adults. The presence of only one of these signs should lead to oncological excision.
Conclusion
Osteochondroma is a common and well-known benign tumor, but, in certain rare cases, it can be misleading due to its atypical location or radiological appearance. The risk of sarcomatous degeneration requires close clinical and radiological monitoring and surgical excision if there is the slightest doubt.
References
- Tomeno B. Benign cartilaginous tumors, in: SOFCOT teaching conferences. Paris Elsevier. 2000; 73.
- Dahlin DC, Unni KK. Bone tumors: General aspects and data on 8,542 cases. Springfield, IL: Charles C Thomas. 1986; 4th ed: 119-40.
- Gouin F, Venet G, Moreau A. Solitary exostoses, exostose diseases and other exostoses-Encyclopé-die Médico Chirurgicale. Treatise on the musculoskeletal system. 2001; 5: 14-724.
- Lee KCY, Davies AM, Cassar-Puillicino VN. Imaging the complications of osteochondroma. Clin Radiol. 2002; 57(1): 18-28.
- Percy EC, Birbrager D, Pitt MJ. Snapping scapula: A review of the literature and presentation of 14 patients. Can J Surg. 1988; 31: 248-50.
- Tomo H, Ito Y, Aono M, Takaoka KD. Chest wall deformity associated with osteochondroma of the scapula: a case report and review of the literature. J Shoulder Elbow Surg. 2005; 14: 103-6.
- Gamanagatti S, Gugalani B, Singh N. Large bursa associated with osteochondroma of ventral surface of scapula. Europ J Radiol. 2004; 51: 103-5.
- Willms R, Hartwig CH, Bohm P, Sell S. Malignant transformation of a multiple cartilaginous exostosis: A case report. Int Orthop. 1997; 21(2): 133-6.
- Poey C, Clement JL. Osteochondroma In: EMC: Radiodiagnosis-Neurology-Musculoskeletal system. Paris: Technical Editions. 1991; 31481 A10: 4p.
