
Open Access, Volume 10
Irreducible traumatic pure hip dislocation by the entrapment of the lateral rotator muscle group of the hip: A case report
Zied Mansi1; Firas Saybi1 ; Abdelkader Tounsi1; Aymen Ben Mahmoud1; Wajdi Chermiti2; Haggui Ali3 ; Zaidi Bacem4; Gazzah Wael5
1Department of Orthopedic Surgery, Ibn El Jazzar University Hospital, Kairouan, Tunisia.
2Department of Orthopedic Surgery, Sahloul University Hospital, Sousse, Tunisia.
3Department of Orthopedic Surgery, Hospital of Kasserine, Kasserine, Tunisia.
4Department of General Surgery, Ibn El Jazzar University Hospital, Kairouan, Tunisia.
5Department of Urology, Ibn El Jazzar University Hospital, Kairouan, Tunisia.
Zied Mansi
Department of Orthopaedic Surgery, Ibn El Jazzar Kairouan University Hospital 3100 Kairouan, Tunisia.
Email: doc.zm@htmail.fr
Received : Jan 22, 2024,
Accepted : Feb 07, 2024
Published : Feb 09, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Irreducibility is a rare complication of pure posterior hip dislocation requiring surgical intervention.
Case report: We present a case of a 22-year-old female with posterior hip dislocation following a motor vehicle accident. Despite unsuccessful closed reduction attempts, open surgical reduction successfully released the incarcerated muscles and achieved reduction. Follow-up examinations showed excellent functional outcomes without complications.
Clinical discussion: Irreducibility remains a rare complication of traumatic posterior hip dislocation. Three possible entities can cause soft tissue incarceration: labral buttonholing, intra-articular osteochondral bodies, and entrapment of the piriformis muscle. The posterior-lateral approach provides excellent exposure of the posterior hip structures, but it carries the risk of injury to the medial circumflex artery. After successfully reducing the dislocation, it is essential to perform a Computed Tomography (CT) scan to detect any osteochondral lesions, including femoral head impaction. Functional outcomes are better with early mobilization and prompt resumption of weight-bearing. However, femoral head osteonecrosis complicates 52.9% of hip dislocations reduced beyond 6 hours, whereas it occurs in only 4.8% of dislocations reduced within this timeframe.
Conclusion: This case underscores the importance of prompt recognition and appropriate surgical intervention for irreducible hip dislocations to prevent further complications and optimize patient outcomes.
Keywords: Hip; Lateral rotator muscle; Dislocation.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Zied M (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Mansi Z, Saybi F, Tounsi A, Mahmoud AB, Chermiti W, et al. Irreducible traumatic pure hip dislocation by the entrapment of the lateral rotator muscle group of the hip: A case report. Open J Clin Med Case Rep. 2024; 2198.
Introduction
Traumatic pure hip dislocation is a traumatological emergency that requires reduction as promptly as possible to avoid serious complications. which can be obtained by closed maneuvers in the majority of cases. However Approximately 3 to 4% of these dislocations are irreducible and necessitate an open surgical treatment, where the possibility of soft tissue incarceration, such as capsuloligamentous or, less commonly, muscular structures, must be considered. The aim of this study was to highlight the existence of this rare entity.
Case Report
We present the case of a 22-year-old female patient with no significant medical history who was involved in a motor vehicle accident resulting in a closed trauma to the right hip without other associated injuries.
On the ER physical examination vital signs were stable, with no signs of hemodynamic instability.
The patient appeared in pain and the right hip exhibited a fixed posture of flexion and internal rotation, with evident deformity and visibly shortened right limb compared to the left side.
No open wounds or external injuries were observed on the skin overlying the hip. Range of motion of the right hip was significantly limited, with severe pain upon any attempted movement.
Neurovascular examination showed intact sensation and normal distal pulses in the affected limb.
Radiological assessment confirmed a pure posterior right iliac hip dislocation (Figure 1).
The patient was promptly taken to the operating room within a 2-hour timeframe for closed reduction under general anesthesia.
Despite 5 attempts using three different external manipulation techniques, reduction was unsuccessful.
A decision was made to proceed with open surgical reduction.
The posterior-external approach (Moore Approach) was chosen to provide better exposure of the posterior structures.
During the procedure, it was observed that the lateral rotator group of muscles were incarcerated (Figure 3), leading to the sectioning of the posterior circumflex artery. Fortunately, there was no involvement of the sciatic nerve.
After successful release of the incarcerated muscles, the reduction was achieved easily (Figure 2).
A CT scan was performed after the open reduction procedure to insure the absence of initial traumatic of an iatrogenic incarceration a bone fragment or an associated non-displaced acetabulum fracture.
The patient was then placed on a functional treatment plan including no-weight-bearing for 6 weeks with early rehabilitation and was then allowed to resume full weight bearing gradually.
At the 4 months follow-up, the patient has returned to the anterior normal life activities. There were no signs of hip instability in the last physical examination and the radiological assessments showed no signs of avascular necrosis of the femoral head which is the main feared complication.
At the 2-year follow-up, the functional outcome was excellent with a Harris score of 100 points and no signs of necrosis or osteoarthritis.

Figure 1: Pure posterior right iliac hip dislocation.
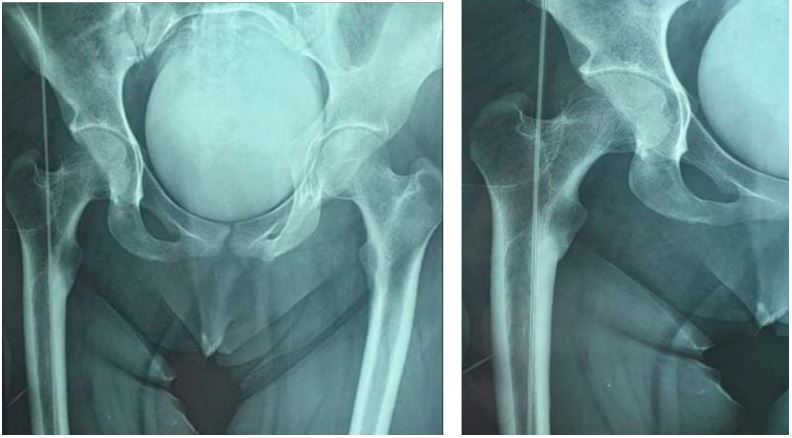
Figure 2: Post-reduction X-rays.
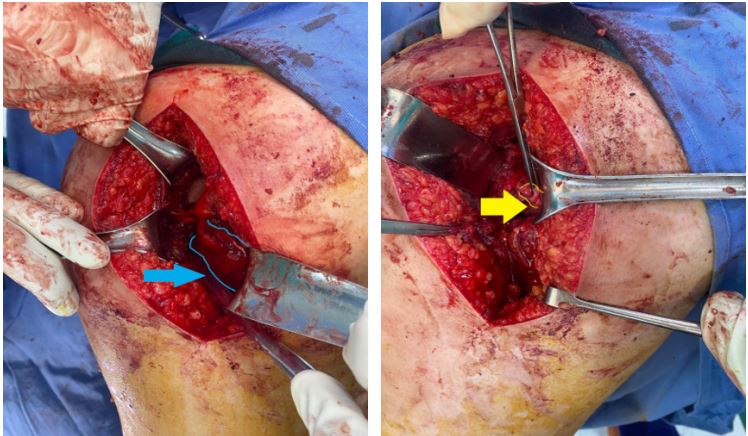
Figure 3: Entrapment of lateral rotator group (blue) section of posterior circumflex (yellow).
Discussion
Irreducibility remains a rare complication of traumatic posterior hip dislocation. It accounts for only 3% [1,2] of cases, and among the various potential causes, soft tissue incarceration is the most frequent etiology
Depending on the position of the hip at the moment of trauma [3,4], three possible entities can cause soft tissue incarceration: Labral buttonholing, intra-articular osteochondral bodies, and entrapment of the piriformis muscle [2,5].
According to Kim et al [4], in hip flexion-adduction, dislocation poses a threat to the posterior portion of the capsule and labrum, creating a buttonhole-like structure that obstructs the femoral head.
However, the neutral rotation of the femoral head at time of trauma dislocates it in a posteriorsuperior direction towards the piriformis muscle, which can become incarcerated within the acetabular cavity following external reduction maneuvers [2,5].
The posterior-lateral approach provides excellent exposure of the posterior hip structures, but it carries the risk of injury to the medial circumflex artery [6,7]. In our case, the patient presented with irreducible hip dislocation due to incarceration of the lateral rotator group of hip muscles. The presence of the incarcerated muscles (Figure 2) and the subsequent sectioning of the posterior circumflex artery (Figure 3) were identified during the surgical procedure. It is important to consider irreducibility and the possibility of soft tissue incarceration in cases of failed closed reduction attempts.
Prompt recognition and appropriate surgical intervention are necessary to achieve successful reduction and prevent further complications. Park, Kyeong Hyeon et al. [8] emphasizes the importance careful examination of plain radiographs and CT images for determining the safest treatment strategy before attempting repeated or forceful closed reduction of irreducible femoral head dislocation injuries which can result in iatrogenic femoral neck fractures with Pipkin type III injuries.
Surgical exploration allows for an initial assessment of the injuries and subsequently enables surgical reduction of the dislocation after removing the obstacle.
After successfully reducing the dislocation, it is essential to perform a Computed Tomography (CT) scan to detect any osteochondral lesions, including femoral head impaction. These injuries have the potential to significantly impact the long-term functional outcome of the hip [9].
Functional outcomes are better with early mobilization and prompt resumption of weight-bearing. However, femoral head osteonecrosis complicates 52.9% of hip dislocations reduced beyond 6 hours, whereas it occurs in only 4.8% of dislocations reduced within this timeframe [10].
Conclusion
Further studies and research are warranted to explore the incidence, etiology, and optimal management strategies for irreducible traumatic hip dislocations with soft tissue incarceration.
Declarations
Conflict of interest: The authors declare that they have no conflict of interest.
Funding: There is no funding source.
Informed consent: Informed consent was obtained from all patient participant in the study.
References
- Canale ST, Manugian AH. Irreducible traumatic dislocations of the hip. Journal of Bone and Joint Surgery - Series A. 1971; 61(1). https://doi.org/10.2106/00004623-197961010-00003
- Slätis P, Latvala A. Irreducible traumatic posterior dislocation of the hip. Injury. 1974; 5(3). https://doi.org/10.1016/S0020-1383(74)80003-3
- Andaloussi YE, Essi FA, Arssi M, Cohen D, Trafen M. Irreducible traumatic dislocation of the hip caused by labral and capsular entrapment with a buttonhole effect. Revue de Chirurgie Orthopedique et Reparatrice de l’Appareil Moteur. 2006; 92(3). https://doi.org/10.1016/s0035-1040(06)75737-3
- Kim YT, Ninomiya S, Tachibana Y, Tanabe T, Yano Y. Acetabular labrum entrapment following traumatic posterior dislocation of the hip. Journal of Orthopaedic Science. 2003; 8(2): 232-235. https://doi.org/10.1007/s007760300039
- Slasky BS, Liebergall M. Irreducible traumatic posterior dislocations of the hip. Emergency Radiology. 1997; 4(2). https://doi.org/10.1007/BF01508038
- Garrett JC, Epstein HC, Harris WH, Harvey JP, Nickel VL. Treatment of unreduced traumatic posterior dislocations of the hip. The Journal of Bone and Joint Surgery. American Volume. 1979; 61(1): 2-6.
- Nepple JJ, Schoenecker PL, Clohisy JC. Treatment of posttraumatic labral interposition with surgical hip dislocation and labral repair. The Iowa Orthopaedic Journal. 2011; 31: 187-192.
- Park KH, Kim JW, Oh CW, Kim JW, Oh JK, et al. A treatment strategy to avoid iatrogenic Pipkin type III femoral head fracturedislocations. Archives of orthopaedic and trauma surgery. 2016; 136: 1107-1113.
- Chun KA, Morcuende J, El-Khoury GY. Entrapment of the acetabular labrum following reduction of traumatic hip dislocation in a child. Skeletal Radiology. 2004; 33(12): 728-731. https://doi.org/10.1007/s00256-004-0800-z.
- Traumatic posterior dislocation of the hip-Prognostic factors influencing the incidence of avascular necrosis of the femoral head | SpringerLink. (n.d.). 2023, https://link.springer.com/article/10.1007/BF00435649
- Agha RA, Franchi T, Sohrab C, Mathew G, Kirwan A, et al. The SCARE 2020 guideline: Updating consensus Surgical Case Report (SCARE) guidelines. International Journal of Surgery. 2020; 84(1): 226-30.
