
Open Access, Volume 10
Bilateral breast metastasis due to rectal cancer: A rare case report
Zekeriya Hannarici1*; Ali Yılmaz1; Mehmet Emin Buyukbayram1; Mehmet Bilici1; Salim Başol Tekin1; Remzi Arslan2; Aykut Turhan1; Alperen Akansel Çağlar1; Pınar Çoban Eşdur1; Salih Gölcüklü1; Elif Bayraktar1
1Department of Medical Oncology, Faculty of Medicine, Atatürk University, Erzurum, Turkey.
2Department of Pathology, Faculty of Medicine, Atatürk University, Erzurum, Turkey.
Zekeriya Hannarici
Department of Medical Oncology, Atatürk University Faculty of Medicine, Erzurum, Turkey.
Tel: +905303768489;
Email: hannarici@hotmail.com
Received : Jan 20, 2024,
Accepted : Feb 06, 2024
Published : Feb 09, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Metastasis from solid organs to the breast is rare. Similarly, metastasis from the rectum to the breast is a quite rare clinical condition. In particular, metastasis from the rectum to the bilateral breast is much less common. We reported a women patient with bilateral breast metastasis from the rectum at the age of 58 years. Extensive metastatic mass was detected in both breasts on Positron Emission TomographyComputer Tomography and biopsy was performed separately from the masses of both breasts. CDX-2 positive, Cytokeratin 7 negative, estrogen receptors negative, progesterone receptors negative in tumoral areas immunohistochemically verified the breast metastasis of rectal adenocarcinoma. In light of this information, biopsy should be performed to direct the treatment in patients with solid organ cancer with a potential mass in the breast in need of metastasis or primary tumor differentiation.
Keywords: Breast cancer; Breast metastasis; Rectal carcinoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Hannarici Z (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Hannarici Z, Yılmaz A, Buyukbayram ME, Bilici M, Tekin SB, Arslan R, Turhan A, et al. Bilateral breast metastasis due to rectal cancer: A rare case report. Open J Clin Med Case Rep. 2024; 2197.
Introduction
Metastases to the breast are uncommon [1]. Breast metastases mostly develop from contralateral primary breast cancer, however, only around 0.3-2% develops from solid organs such as lung, nasopharynx, ovary, stomach, thyroid and cervix [2]. Metastases from rectal carcinoma to the breast are uncommon. Additionally, metastasis from rectum to bilateral breast is much uncommon [3,4]. We reported rectum cancer with bilateral breast metastasis.
Case Presentation
A married women patient aged 58 years applied to our hospital with a diagnosis of rectal cancer in an external health center. In the general examination of patient there were icterus an the Eastern Cooperative Oncology Group (ECOG) performance score of patient was three. The patient was hospitalized having carcinoembryonic antigen (CEA): 299 ng/ml (normal, 0-3 ng/ml), Carbohydrate Antigen (CA) 15-3: 18.1 U/ ml (normal, 0-31.3 U/mL), bilirubin: 2.44 mg/dL (normal 0.18-1.20 mg/dL) and International Normalized Ratio (INR): 2.9 (normal, 0.9-1.3) in her laboratory. The patient applied to another healthcare center with the complaints of diarrhea and weight loss that started about three months ago, and upon undergoing colonoscopy, it was reported that the patient had polypoid lesions in 6 cm of the rectum, mass lesion at 10-15 cm, and irregular mucosa at 20 cm. The patient’s three focal pathology reports were reported as moderate adenocarcinoma. In Positron Emission Tomography-Computer Tomography (PET-CT), besides a primary mass of 20 cm starting from the distal rectum-proximal anal canal to the distal of the sigmoid colon; there were inferior retropharyngeal Lymph Node (LN) metastasis, inferior jugular LN metastasis, pulmoner metastasis, widespread bone metastasis, liver metastases, intraabdominal metastases and mass lesions in both breast parenchyma (Figure 1). A tru cut biopsy was performed from both breasts in terms of synchronous mass or metastasis in the breast defined in PET-CT. Histopathologically atypical pleomorphic cells with hyperchromatic nucleus, some with distinct nucleolus, large cytoplasm in invasive stroma, partly solid islands and tumoral structures with gland-like structures partly were observed among sparse normal ductus structures in the samples taken from both breasts. The immunohistochemical study resulted in CDX2 diffuse nuclear positive, e-caderin positive, Estrogen Receptors (ER) and Progesterone Receptors (PR) negative, p63 negative, Cytokeratin (CK) 7 and CK20 negative, CerbB2 negative (score 0) in tumoral elements (Figures 2,3). The supportive treatment was provided to the patient as the ECOG performance score of the patient was 3, and the bilirubin and INR levels in the admission laboratory test were high. The patient whose performance worsened in the follow up died three months after the diagnosis.
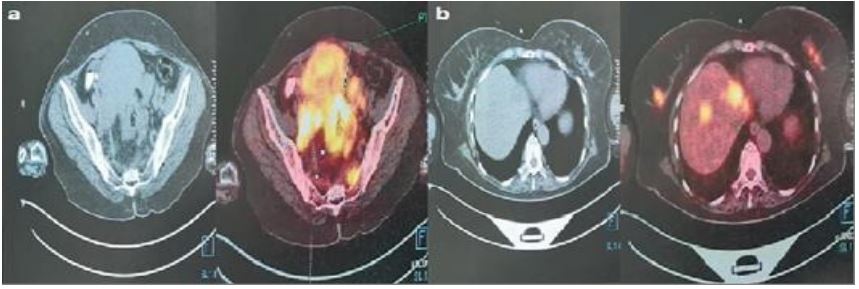
Figure 1: In PET-CT screenings, a: Hypermetabolic primary mass areas were observed in the rectum. b: Metastatic masses
with FDG uptake were observed in both breasts.
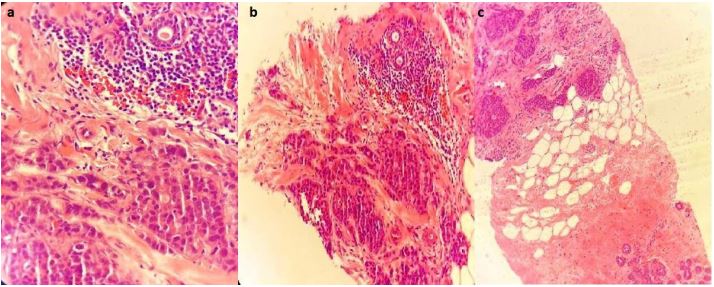
Figure 2: Histopathologically metastatic areas are verified in both breasts (a: Light lymphocytes around normal duct structures in the upper right breast and metastatic tumoral areas in the lower part H&Ex200, b: Light lymphocytes around normal
duct structures in the upper right breast and metastatic tumoral areas in the lower part H&Ex100, c: Left breast: Normal
breast ducts in the lower right corner and metastatic tumoral areas in the upper left corner H&Ex40).
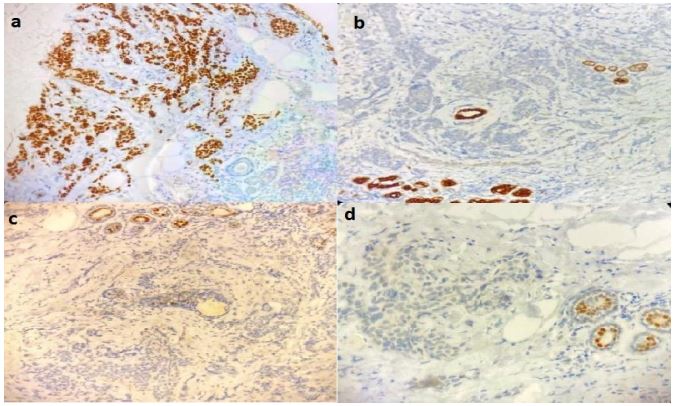
Figure 3: Staining verifying rectal metastasis immunhistochemically (a: Diffuse nuclear CDX2 positivity in the metastatic
tumoral area CDX2x100, b: CK7 negative in the metastatic tumoral area CK7x100, c: ER negative in the metastatic tumoral
area ERx100, d: PR negative in the metastatic tumoral area PRx100).
Discussion
Metastasis from the extra mammarial region to the breast is very rare while primary breast cancer is one common cancer [5]. Lymphoma, leukemia, melanoma, sarcoma, lung, stomach, esophagus, ovarian and oropharynx cancers can metastasize to the breast [1,6]. Whereas breast metastasis of colorectal cancer is very rare, breast metastasis is associated with widespread disease and poor prognosis [7]. Although metastasis of rectal adenocarcinoma is rare, in the literature review, two women cases aged 45 and 28 years diagnosed with rectal adenocarcinoma and bilateral breast metastasis were reported [8,9]. In a review, the majority (55%) of the 19 colorectal cancer patients was detected to have left breast metastasis, 30% right breast metastasis, and only two cases had bilateral breast metastasis. Also, 75% of the cases had metastases in other organs besides the breast [10]. In our case, there was both breast and axillary LN node uptake. Similarly to the information from the literature, besides the breast, there were inferior retropharyngeal and inferior jugular LN metastases, pulmoner metastases, widespread bone metastases, liver metastases and intraabdominal metastases.
According to the literature, metastasis to the breast is generally seen in women at a mean age of 50 years [11]. Breast metastasis is thought to occur approximately 2 years following the diagnosis of the primary tumor after multiple metastases develop in the advanced stage of the disease [12]. In parallel with the literature, our female patient aged 58 years applied to the hospital with multiple metastases.
In the immunohistochemical study, CK20 and CDX2 were positive in colorectal cancers and the breast indicators CK7, ER, PR were negative in 90% of cases [13]. In our case, both CK20 and CK7 were negative, while e-cadherin and CDX2 specific to the intestinal area were positive. Breast indicators ER, PR and CerbB2 were negative. KRAS, NRAS and BRAF were not studied as the patient’s clinical condition was poor and right after she died.
In case of metastasis to the breast, treatment management is complex and is affected by many factors such as age, performance score and different organ metastases. According to the recent reports, the management of colorectal cancer that has metastasized to the breast should be diagnostic and palliative [14]. Surgery is not recommended due to its short life expectancy and the risk of inoculating the tumor to the skin [15]. Metastasis to the breast is reported to be associated with poor prognosis [7].Our patient was followed palliatively since her ECOG performance score was poor and biochemical parameters were not suitable for chemotherapy. Based on the information from the literature, the patient had a poor prognosis and she died shortly after being diagnosed with breast metastasis.
As a result; both breast and colorectal cancers are among the common types of cancer. Even though rectal cancer has the potential to metastasize to the breast localization, this has rarely been reported in the literature. In patients diagnosed with rectal cancer, the presence of suspicious breast lesions should be verified by biopsy with a second primary tumor.
Declarations
Ethical approval all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Conflict of interest: The authors declare that they have no conflict of interest.
Funding: This case report received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
References
- Toombs BD, Kalisher L. Metastatic disease to the breast: Clinical, pathologic and radiographic features. AJR Am J Roentgenol. 1977; 129: 673-676.
- Sun P, Chen J, Lu J, Luo R, Li M, et al. Characteristics of breast metastases from non-breast solid tumors in 22 patients from a southern Chinese population. Oncol Lett. 2018; 15: 3685-3693.
- Hisham RB,Th uaibah H,Gul YA. Mucinous adenocarcinoma of the rectum with breast and ocular metastasis. Asian J Surg. 2006; 29: 95-97.
- Wakeham NR, Satchithananda K, Svensson WE, et al. Colorectal breast metastases presenting with atypical imaging features. Br J Radiol. 2008, 81: 149-153.
- Ho YY, Lee WK. Metastasis to the breast from an adenocarcinoma of the colon. J Clin Ultrasound. 2009; 37(4): 239-41.
- Lee SK, Kim WW, Kim SH, et al. Characteristics of metastasis in the breast from extra mammarymalignancies. J Surg Oncol. 2010; 101(2): 137-140.
- Del Prete C, Del Prete SA, Babkowski RC. Breast metastasis from colonic primary: A case report and review of the literature. Conn Med. 2009; 73(7): 399-402.
- Wakeham NR, Satchithananda K, Svensson WE, et al. Colorectal breast metastases presenting with atypical imaging features. Br J Radiol. 2008; 81: e149153.
- Makhdoomi R, Mustafa F, Ahmad R, et al. Bilateral breast metastasis from mucinous adenocarcinoma of the rectum: A case report and review of the literature. Turk Patol Derg. 2013; 29: 231-4.
- Shackelford RE, Nandyala PA, Bui MM, Kiluk JV, Esposito NN. Primary colorectal adenocarcinoma metastatic to the breast: Case report and review of nineteen cases. Case Reports in Medicine. 2011; 2011: 738413.
- Williams SA, Ehlers RA 2nd, Hunt KK, et al. Metastases to the breast from nonbreast solid neoplasms: presentation and determinants of survival. Cancer. 2007; 110: 731-7.
- Vergier B, Trojani M, De Mascarel I, Coindre JM, Le Treut A. Metastases to the breast: Differential diagnosis from primary breast carcinoma. J Surg Oncol. 1991; 48: 112-116.
- Singh T, Premalatha CS, Satheesh CT, et al. Rectal carcinoma metastasizing to the breast: A case report and review of literature. J Can Res Ther. 2009; 5: 321-323.
- Vakili SM, Sharbatdaran M, Noorbarn A, et al. A case of colon cancer with breast metastasis and krukenberg tumor. Int J Hematol Oncol Stem Cell Res. 2014; 8: 46-50.
- Barthelmes L, Simpson JS, Douglas-Jones AG, Sweetland HM. Metastasis of primary colon cancer to the breast-leave well alone. Breast Care. 2010; 5: 23-25.
