
Open Access, Volume 10
Evaluating the quality of life in new mothers: A simplified approach
Saumya Uppal*
My Digi Records, Kansas City, 1801 Oak Street Kansas City, Missouri 64108, USA.
Saumya Uppal
My DigiRecords, Kansas City, 1801 Oak Street Kansas City, Missouri 64108, USA.
Tel: 732-642-0251;
Email: saumya.uppal@gmail.com
Received : Jan 05, 2024,
Accepted : Feb 01, 2024
Published : Feb 09, 2024,
Archived : www.jclinmedcasereports.com
Abstract
According to Oxford Definitions, Quality of Life (QoL) is defined as the standard of health, comfort, and happiness experienced by an individual or group. For this project, I assessed the correlation between a vulnerable population, new mothers, and their QoL. I worked with My Digi Records, a healthcare organization embodying a patient-centered approach, to see if QoL for this population could be improved using an application (app) where new mothers can keep track of their newborn’s health records. My project goals were to research and understand the primary needs and barriers within this population so, I can pinpoint potential contributing factors affecting their QoL. Then, I would explore how new mothers currently track or plan to track their newborn’s health records. Based off the collected feedback and research, my objective was to identify and pinpoint areas where the MyDigiRecords app could be leveraged as a solution in improving new mothers’ QoL.
My overall aim was to outline and formulate a final protocol/playbook with improvement recommendations to capture Phase One of MyDigiRecords’ application integration process and align with organization-wide goals. This would provide them with the background and research necessary to proceed with Phase Two of integrating the app into birthing clinics and practices and even expanding their scope to cater to other populations in the future.
I extracted numerous findings from this project such as that it is evident that while QoL in general has been an existing and well-researched topic, QoL within the new mother population is relatively newer. Because of this, I found that there was a scarcity of literature regarding the long-term QoL parameter in new mothers. However, the studies I did research and analyze showed many factors such as but not limited to, education levels, type of feeding for newborn, type of birth, environment, and social activity, can impact a new mother’s QoL. Generally, most studies agreed that QoL scores worsen as the pregnancy journey continues. It was found that during pregnancy, traumatic or abnormal scenarios significantly and negatively impacted a mothers’ postpartum QoL score. Along with this, new mothers having poor QoL prior to pregnancy, due to external factors outside of pregnancy, birth, and postpartum, will likely have an aggravated or deteriorated QoL postpartum.
Keywords: Quality of life; New mothers; Application; Electronic health records; Digital health; Population; Focus group.
Abbreviations: EHR: Electronic Health Records; QoL: Quality of Life; App: Application.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Uppal S (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Uppal S. Evaluating the quality of life in new mothers: A simplified approach. Open J Clin Med Case Rep. 2024; 2195.
Introduction
MyDigiRecords (MyDigiRecords CEO, Dr. Saroj Gupta, saroj@mydigirecords.com) is a healthcare organization that focuses on digital health records and patient data management, providing a secure platform for patients, healthcare providers, and stakeholders to access and manage their Electronic Health Records (EHR). The organization’s emphasis on leveraging technology to enhance data accessibility, interoperability, and security contributes to the advancement of personalized medicine and data-driven research, making it extremely patient-centered and ultimately, improving patient outcomes.
Partnering with MyDigiRecords for my capstone helped me not only expand on my existing interest in digital health, but I also learned more about the processes and best practices that organizations in this field follow, the different moving parts, and areas to be cognizant about, and how important it is to advocate for patients in vulnerable populations, as this is the priority demographic MyDigiRecords focuses on. MyDigiRecords’ commitment to improving healthcare delivery, facilitating seamless data sharing, and empowering patients highlights their overarching mission of transforming the way people manage their health data, empowering them to make better-informed decisions and improve overall health outcomes.
MyDigiRecords has developed an application for users to manage as well as organize their important health information, such as immunizations and current medications. This application allows users to have increased accessibility to their health records and remain up to date with any changes related to their health records. MyDigiRecords would like to integrate the application within a variety of healthcare settings and populations for greater convenience for patients and healthcare professionals alike.
The purpose of my project is to help jumpstart the initial phase of the ongoing endeavor of app integration and usage at MyDigiRecords. I will be researching current available data and studies on QoL for one specific population, new mothers, to understand and assess needs, gaps, and risks amongst this vulnerable population and using that information to formulate a well-planned playbook so that the organization can utilize and refer to it not just for themselves, but for various types of clinics, where new mothers would visit, or even just for patients seeking easier alternatives to record keeping. I chose this population because aside from it being a vulnerable population, this is a bigger population and there is a greater need in this area. New mothers are widespread across the world and there will always be new mothers, so I wanted to study this population in hopes of making my research meaningful as well benefitting this population because motherhood is a complicated journey on its own. This application is essential in the health informatics and analytics space because it enables users to take control and become aware of their own health, all at the touch of their fingers. This innovation will be a positive step towards bridging health disparities for vulnerable populations such as new mothers, older adults, and children.
Case Study
My project goals were to assess this new mother population and understand their primary needs and how they trace back to QoL. Since QoL is complex, I wanted to understand which solutions to improve QoL would be most advantageous for this population. Through researching and identifying the methods new mothers use or plan to use to track their newborn’s health records, I intended to receive important real-world insight and was able to find areas where MyDigiRecords’ app can serve to alleviate the stressors and information gaps faced by new mothers today. With this information and deeper interviews and literature reviews, my goal was to clearly present my findings for MyDigiRecords, clinics, and even patients, to utilize in the future for greater accessibility and clarity.
MyDigiRecords app is a unique health record app in the market today. There are valuable features embedded into the app that would cater to all populations. One of the standout features is a dashboard that can provide a user with an overview of not just their own records, immunizations, and medications, but also the same information for other family members through family profiles. This is extremely beneficial for those users living in a household with younger children and older adults. This feature exemplifies MyDigiRecords’ primary message of personal health management. There is also a medication management dashboard, which serves as a central location for all things medications, including medication records, over the counter medications, and past and current medications. Additionally, the app allows users to set medication alerts to ensure no dose is missed.
This app could help new mothers tremendously, especially during the first few months postpartum. The screens below (from left to right) show what it would look like if a new mother was using the app. Figure 1 is an example of what the new mother would see if she wanted to find out about immunization records (Figure 1). The mother can view and manage both her immunization records and her newborn’s immunization records from this screen. If the mother wants to just see her newborn’s immunization list along with the progress status in timeline form, the interface will be like Figure 2. With this screen, the new mother can distinct which immunizations are completed, which are coming up short-term, and which are coming up long-term.
Furthermore, if, postpartum, the new mother had to take any medications and was unable to or too busy with the newborn to keep track of it, the app has a feature where the new mother can input her own medications as well dosage and frequency (Figures 3 and 4). Similarly, if her newborn required medications at certain times, she could input the newborn’s medications as well as set alerts to remind her when to take her medication and when to give the newborn his or her medications. In this scenario with the new mother population, she can utilize the medication list for both her and her newborn, if applicable, and have alerts set so that she can be reminded during their busy days. These types of features would prove to be incredibly helpful for new mothers, potentially enhancing their QoL. The postpartum phase represents a significant period of adjustment and can pose considerable challenges for new mothers as they strive to reintegrate back into their regular routines. Even seemingly simple alerts from an app could contribute to reducing worries and concerns, and lessening some of the new mother challenges faced, providing this population with more peace of mind.
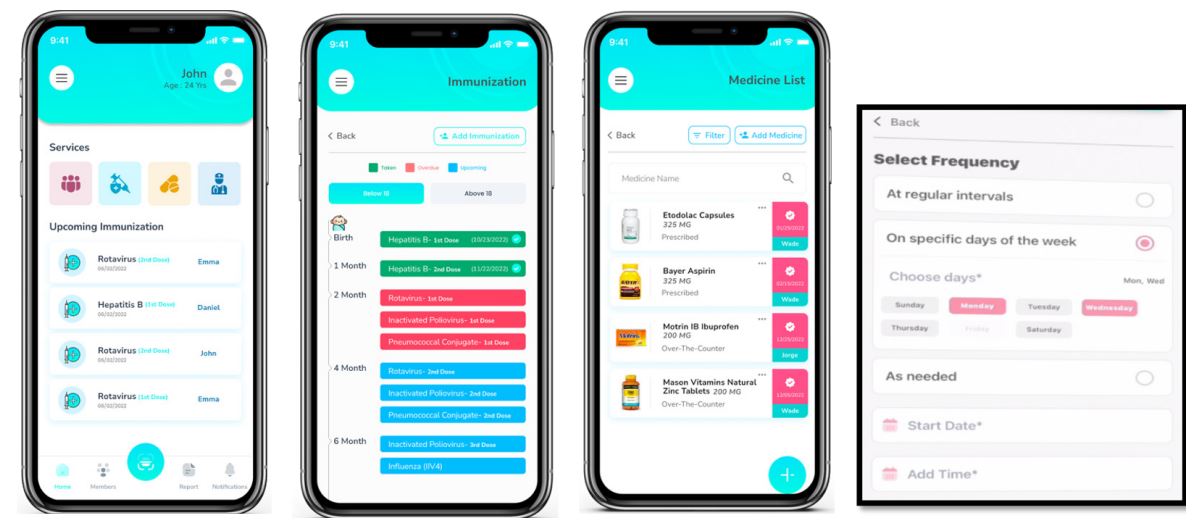
Figure 1 to 4:
Data Collection and Methods
General QoL is a well-studied parameter. Therefore, I began my data collection by conducting a general literature review on QoL that encompassed various populations. Then, I delved into a more extensive search, specifically searching for correlations between QoL and new mothers. Within this investigative analysis, I concentrated more on the range of factors that influence new mothers’ QoL, both positively and negatively. The literature searches and review allowed me to obtain quantitative data. Parallelly, I wanted to identify and engage with new mothers to obtain real-time qualitative data and methods. To do so, I formulated a series of questions to ask new mothers and conducted one-on-one interviews (Table 1).
For this project, I employed two primary methods: interviews and literature searches and reviews. The literature I studied and extracted majority of data from was from different regions: United States, Iran, India, Spain, Saudi Arabia, and South Korea. Secondary methods comprised of further qualitative and quantitative research, leveraging analysis and general observations derived from social media platforms such as Facebook, Reddit, and Instagram.
Table 1:
| 1. How long ago was your pregnancy? Was it your first pregnancy? |
|---|
|
2. How was your pregnancy
experience on a scale of
1-5, 1 being relatively
easy, 5 being extremely
difficult? Briefly explain
why you rated the way you did. |
| 3. What was the most difficult aspect of the transition from pregnancy to postpartum? |
| 4. In your opinion, what impacted your quality of life after pregnancy the most? |
| 5. How are you currently tracking or planning to track your baby’s medical records (immunizations, tests, treatments, notes)? |
| 6. Would you consider tracking your baby’s medical records with the help of an app? If so, why? If not, why not? |
| 7. Personally, what do you think could help with positively increasing your Quality of Life? |
Data Analysis and Results
My analysis plan consisted of finding 15 to 20 relevant studies related to general QoL and QoL in new mothers specifically. Upon reviewing the studies, I would narrow down the number of studies to my project needs. This refinement included identifying the credibility of the source, sample sizes, frequency of time between check-ins or follow ups and so on. After having my set number of studies, I highlighted areas where I found overlaps and contradictions when discussing QoL factors in new mothers. This was my principal focal point as I was looking for if contributing QoL factors are standardized in new mothers. If there were consistent contributing QoL factors, then an app, like MyDigiRecords’ app, could facilitate new mothers with managing those and even further assist with recognizing individual needs, which would not be found in any such literature.
Depression is a common factor new mothers deal with during postpartum. Approximately 50% of the new mother population experience a mild period of depression after giving birth [2]. This phase usually lasts up to two weeks postpartum. However, up to 20% of new mothers, will experience a more serious depression period, consisting of heightened sensations of sadness, anxiety, and irritability [2]. This is commonly known as postpartum depression. These symptoms are longer lasting and may manifest at any point within the initial year after giving birth. Some women may also develop postpartum psychosis, which is a rare, but serious condition, impacting 1 out of 500 to 1,0000 new mothers [2].
There was a QoL study done in Iran with a sample size of 357 pregnant women. This study examined the QoL of women in their third trimester of pregnancy and at 8 weeks postpartum and the factors associated with their overall QoL. The premise of the study was that these women gauged their QoL during the antenatal and postnatal periods. It was found that in the antenatal period, meaning prior to birth, 27% of these women evaluated their overall QoL as very good, 54% as good, 18% as ‘not good, not bad’, 8% as bad and 0.3% as very bad [7]. In the postnatal period, we see the percentages shift. 26.5% women evaluated their overall QoL as very good, 52.8% as good, 19% as ‘not good, not bad’, 0.9% as bad and 0.9% as very bad [7]. The biggest takeaway here is that QoL was lower across most categories in the postnatal period when compared to the antenatal period.
There was another study from my literature review which looked at collective QoL scores and the specific dimensions that influence QoL over three specific time points: before 1 year postpartum, 1 to 3 years postpartum and more than 3 years postpartum [6]. This study was done with a sample size of 2990 Spanish women. This was a unique study because most studies typically refer to QoL during pregnancy and a short postpartum period, ranging six weeks or six months, but have not dealt with long-term QoL as this study does. This study also highlights the many different dimensions contributing to and directly impacting QoL. As seen in Table 2, we see that QoL tends to worsen with time in the motherhood journey, as the overall QoL score indicates with a p-Value of 0.045, making it statistically significant [Table 2]. Many of the other dimensions are also statistically significant, such as general health and emotional role with a p-Value of less than 0.001, and mental health with a p-Value of 0.0056. These poorer QoL values align with another study done in South Korea with 5146 women, who were over 50 years of age. The study done with Spanish women showed that the mother’s age is not a QoL-related factor, which contrasts the South Korea study, where Parks and Choi found that a younger aged mother (at childbirth) is a determining factor for lower QoL [10]. Amongst majority of other studies, it was found that the gestational age of women at the time of birth was indeed a risk factor for a worse QoL score [6,10].
Another debated contrast between the studies included types of feedings: Breastfeeding versus formula-fed. In one study, the women who formula-fed their newborns did not obtain worse QoL scores than those who breast-fed, which contradicts the results of another study lead by Triviño-Juárez et al., where the authors associated breast feeding with a better QoL at six weeks postpartum [6]. The study based in Iran showed that breastfeeding difficulties negatively affect all dimensions of QoL [7]. Breastfeeding difficulties include “pain, cracked nipples, milk stasis or mastitis” and are “associated with higher levels of psychological stress during first weeks postpartum” [7]. Furthermore, another study found that women who had negative breastfeeding experiences were “more likely to experience depressive symptoms at 2 months postpartum” [7] when compared to those women who had neutral to positive breastfeeding experiences.
Table 2:
| Variable | Time since last birth | * For linear | |||
|---|---|---|---|---|---|
| Less than 1 year Mean (SD) |
between 1-3 years Mean (SD) |
More than 3 years Mean (SD) |
p-Value* | p-Value tendency |
|
| Overall quality of life | 71.94(17.48) | 71.75(18.01) | 70.23(19.25) | 0.084 | 0.045 |
| Physical function | 89.46(20.72) | 91.27(18.76) | 89.11(22.58) | 0.040 | 0.786 |
| Physical role | 65.25(44.52) | 72.96(40,78) | 70.53(42.04) | <0.001 | 0.005 |
| Bodily pain | 85.34(22.77) | 84.99(23.87) | 83.40(24.67) | 0.168 | 0.079 |
| General health | 63.11(18.76) | 60.01(19.89) | 57.28(19.72) | <0.001 | <0.001 |
| Vitality | 51.72(23.00) | 51.27(22.39) | 51.23(23.66) | 0.868 | 0.632 |
| Social role functioning | 75.70(25.99) | 74.68(26.98) | 74.41(26.08) | 0.525 | 0.284 |
| Emotional role | 80.61(36.98) | 76.58(39.83) | 73.88(41.53) | 0.001 | <0.001 |
| Mental health | 64.31(18.08) | 62.23(18.58) | 61.96(18.97) | 0.009 | 0.005 |
*Analysis of variance; SD: Standard Deviation
While there were contradictions between each study’s outcomes, there were quite a few overlaps, one of the most significant ones being the correlation between type of birth and a mother’s QoL. One Iranian study reported that women who had cesarean births reduced the global QoL [7]. In an additional Iranian study, it was found that mothers who had vaginal deliveries also had a better QoL for dimensions, “such as vitality and mental health, at 8 weeks and for physical functioning at 12 weeks postpartum” [7]. The findings from this study corroborated the same results from the first Iranian study, showing that the “vaginal delivery group improved more on physical health related QoL than the caesarean group” [7]. There was another study done in India, with a sample size of 224 women, between 18 to 36 years of age. Of these women, 79% gave vaginal birth and 21% gave birth by cesarean section [5]. This study evaluated the QoL and five health dimensions (mobility, self-care, usual activities, pain or discomfort, and anxiety or depression) of these women 3 times after giving birth: 0 to 3 days postpartum, 3 to 7 days postpartum, and 21 to 30 days postpartum. Collectively, it was found that postpartum QoL in both groups improved between the first check-in and the third [5]. When comparing between vaginal and cesarean births, it was found that the vaginal birth group had a higher QoL (0 to 3 days postpartum: 0.28 vs. 0.57, 3 to 7 days postpartum: 0.59 vs. 0.81; P<0.001) and was less likely to report any slight problems in four of the five health dimensions (mobility, self-care, usual activities, pain or discomfort; P≤0.04) during interviews 1 and 2 (Table 3). Overall, it was discovered through this study that vaginal births, even with complications such as episiotomy, were associated with a higher postpartum QoL in comparison to caesarean births [5] (Table 4).
Another significant parameter affecting QoL identified across majority of the studies were prior impacting factors, unrelated to pregnancy. It was learned that women who had poor QoL before their pregnancy, due to factors unrelated to the pregnancy, birth, and postpartum process, are predisposed for lower postpartum QoL scores as the journey from pregnancy to postpartum is quite stressful and the prior factors can continue to aggravate their QoL. Other common postpartum overlaps found impacting QoL amongst the studies included presence or lack of social engagement [11], presence or lack of marital intimacy [4], and body weight postpartum, which contributed to increased mental health issues like depressive symptoms, and therefore lower QoL scores [7]. Higher QoL scores postpartum were associated with the presence of social engagement and marital intimacy. In fact, marital intimacy (β=0.466, p<0.001) was the most influencing factor on the QoL of women during the postpartum period [4] and with proper social support, mothers would be able to cope with any physical and psychological issues faced during postpartum [11]. Comparison of problems by EQ-5D health dimension in women with vaginal birth and cesarean section within the first month postpartum.
Table 3: Reason for unwillingness to pain relief in labor (n=127).
| Health dimension | Problem level | 0-3 days | Postpartum | 3-7 days | Postpartum | 21-30 | Days postpartum | |||
|---|---|---|---|---|---|---|---|---|---|---|
| VB (%) | CS (%) | P | VB (%) | CS (%) | P | VB (%) | CS (%) | P | ||
| Mobility | No problems | 24.7 | 4.3 | <0.001 | 53.4 | 39.1 | 0.004 | 93.3 | 93.5 | 0.75 |
| Slight problems | 48.3 | 17.4 | 39.3 | 39.1 | 5.6 | 6.5 | ||||
| Moderate problems | 11.2 | 4.3 | 6.2 | 13.0 | 1.1 | |||||
| Severe problems | 5.1 | 34.8 | 1.1 | 2.2 | ||||||
| Unable to | 10.7 | 39.1 | 0.0 | 6.5 | ||||||
| Self-care | No problems | 23.0 | 2.2 | <0.001 | 69.7 | 23.9 | <0.001 | 96.1 | 91.3 | 0.18 |
| Slight problems | 52.2 | 32.6 | 27.0 | 50.0 | 3.9 | 8.7 | ||||
| Moderate problems | 1.7 | 17.4 | 1.7 | 0.0 | ||||||
| Severe problems | 0.6 | 6.5 | 0.0 | 0.0 | ||||||
| Unable to | 22.5 | 41.3 | 1.7 | 26.1 | ||||||
| Usual activities | No problems | 20.8 | 19.6 | 0.01 | 60.1 | 28.3 | <0.001 | 95.5 | 80.4 | 0.001 |
| Slight problems | 46.6 | 23.9 | 35.4 | 39.1 | 3.9 | 19.6 | ||||
| Moderate problems | 8.4 | 10.9 | 1.1 | 8.7 | ||||||
| Severe problems | 1.1 | 6.5 | 1.1 | 0.6 | ||||||
| Unable to | 23.0 | 39.1 | 2.2 | 23.9 | ||||||
| Pain or discomfort | No | 27.0 | 28.3 | 0.008 | 47.8 | 28.3 | 0.04 | 92.1 | 89.1 | 0.28 |
| Slight | 48.9 | 30.4 | 39.3 | 47.8 | 5.6 | 10.9 | ||||
| Moderate | 21 3 | 261 | 11: 8 | 23.9 | 2.2 |
VB: Vaginal Birth; CS: Cesarean Section.
Table 4:
| Vaginal birth | Cesarean section | |||
|---|---|---|---|---|
| All | No episiotomy | Episiotomy | ||
| Mean (95% CI) | Mean (95% CI) | Mean (95% CI) | Mean (95% CI) | |
| QOL weight | ||||
| 0-3 days postpartum | 0.57 (0.52, 0.61) | 0.68 (0.6, 0.75) | 0.51 (0.46, 0.56) | 0.28 (0.18, 0.38) |
| 3-7 days postpartum | 0.81 (0.78, 0.84) | 0.9 (0.87,0.93) | 0.76 (0.73,0.8) | 0.59 (0.51, 0.67) |
| 21-30 days postpartum | 0.93 (0.92, 0.94) | 0.96 (0.95, 0.98) | 0.92 (0.9, 0.93) | 0.85 (0.82, 0.89) |
| QALDs (1-21 days postpartum) | 16.6 (16.2, 17.0) | 18.0 (17.5, 18.5) | 16.0 (15.5, 16.4) | 13.1 (12.0, 14.2) |
| N | 178 | 58 | 120 | 46 |
QALDs: Quality-Adjusted Life Days; QoL: Quality of life.
Two-sample t-tests and Wilcoxon rank-sum tests indicate significant differences in the means and distributions of the QoL weights and QALDs in the following comparisons: All vaginal births vs. cesarean section, no episiotomy vs. episiotomy, no episiotomy, vs. cesarean section, and episiotomy vs cesarean section; P<0.001. QoLs weights increased significantly with the time passed since birth in each of the four birth groups distinguished; P<0.0001 for all comparisons between visits, except for the following comparison: aP=0.04.
Another question I had asked was what they felt was the most difficult aspect of the transition from pregnancy to postpartum. Here again, I saw repetitive answers, most answered that sleep deprivation and breastfeeding were the most difficult and those who had answered with scores of 4s and 5s explained that along with these new changes, constant anxiety and worrying if everything is normal with the baby and processing their birth trauma took a toll on their physical and mental health. One interviewee brought up the fact that advice given to a new mother is not only abundant and overwhelming, but also extremely generic. After birth, there were times where she was not sure what was normal versus abnormal for her baby, which contributed to her stress levels. For example, someone had told her that babies need to be fed every 4 hours, but she noticed her baby became inconsolable if he was not fed every 2 to 3 hours. Due to these diverse scenarios, she started tracking her baby’s records by hand, which was a stark contrast from most of the other interviewees, who were dependent on the doctor’s office tracking and managing their newborn’s records. Out of the 8 women, only one was currently using an app called Huckleberry, to track her baby’s records.
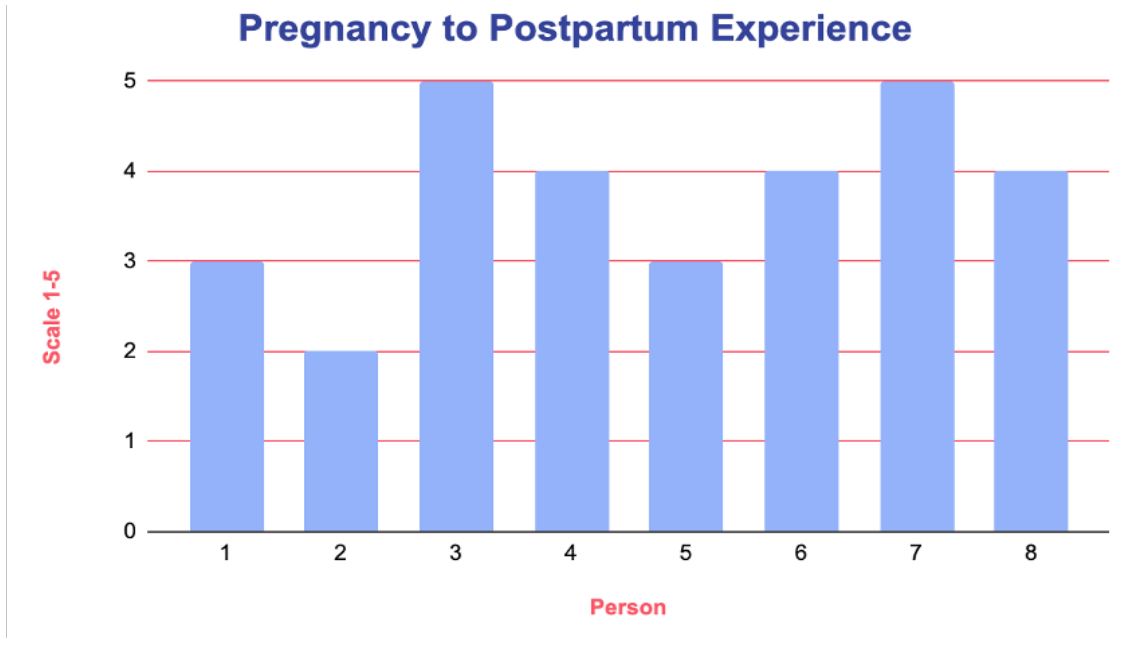
Figure 5:
Figures 6-8 showcase exactly how one of the new mothers recorded her newborn’s health records by hand (Figures 6-8). She tracked everything on her phone’s notes, including vital measurements such as the baby’s weight, height, head circumference over the months. She went into supplementary details and kept track of how much milk she was producing, the range and gaps of times the baby used the diaper, she even differentiated the number of ‘pees’ [diapers] from poos’ [diapers]. At one point, her newborn fell sick and needed antibiotics and she noted down the timings she gave the antibiotics to the baby. This is where an app like MyDigiRecords’ can save time and reduce the manual effort a new mother takes on. The app could facilitate with not only tracking this information, but also alerting her of when it’s time to give the baby the antibiotic.
Although only one out of the 8 women interviewed was using an app, almost all the interviewees were open to the idea of using an app, like the one shown by MyDigiRecords, to help with managing their baby’s health records. Moreover, a few interviewees stated that using an app like this would be especially beneficial for those new mothers whose newborns are experiencing problems and need to frequent the doctor more often or require medications and closer care.
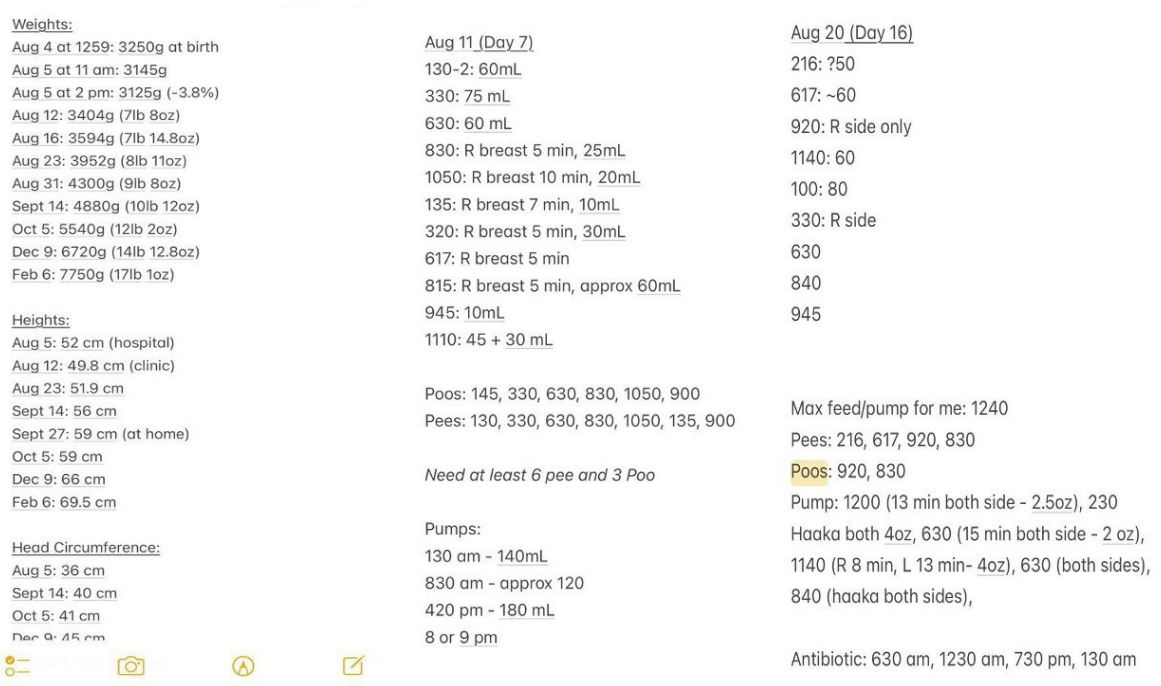
Figure 6 to 8
Discussion
There were a few limitations I faced while working on this project. First, I was not able to find enough literature or studies done on QoL for new mothers only. I did find many on generic QoL and I came across some new mother focused QoL studies which were incomplete and/or very short with no real data. For my own interviews that I conducted, I had a small sample size of just 8 women, due to the timing constraints and the nature of the capstone project having to be completed over one semester. Additionally, I didn’t include set specific criterion, other than just being 0 months to 1 year postpartum, when recruiting new mothers for my interviews. If I had more time, I would have maybe done interviews across various demographics such as age, educational level, race, etc. just to verify my results with the literature I researched. Lastly, this project was solely focused on new mothers, but I do acknowledge that there are other vulnerable populations whose QoL is also suffering and can be improved via an app, but because of timing and having a narrower scope so that the project can be done over the semester, I was unable to assess the linkage between those other populations and their QoL in order to identify if an app could serve as a solution for them as well.
From my interviews and the literature reviews, I gathered that new mothers tend to receive an influx of information from a range of sources, be it their physicians, specialists, neighbors, family members, and so on, throughout their pregnancy journey, but there are no standardized solutions yet to help tackle various QoL-related dimensions. Through this project, I gained exposure to this population and the concept of QoL. I understood the need for this type of research and how all vulnerable populations truly would benefit from this work as well. When I initially decided on this topic, I did not expect it to be as relatable as it ended up becoming. Although I am not a new mother or a mother in general yet, I could identify with the factors, such as stressors or physical and emotional roles, impacting QoL and I think others could as well on a day to day, albeit not to the degree that new mothers do. This is truly an important topic, and I am glad I was given this opportunity to research it. Although prior to this project, I knew my interests lie in product management and app development under the digital health realm, working on this project allowed me to find both related and unrelated interests and areas I thrive in.
Conclusion
Through discovering the contributing factors impacting QoL in new mothers, here are areas where MyDigiRecords can update their app to best care for the new mother population. Currently, the app has prenatal features and pages to support expecting mothers on their pregnancy journeys. Likewise, MyDigiRecords can launch similar features and screens, related to postpartum care for new mothers. Screens within the app related to upcoming baby appointments, postpartum tips and tricks, articles, and a mood journal for the mother can all help with relieving the stress and confusion faced when it comes time to keep track of their baby’s health records and manage their own QoL.
In the short term, based on the findings detailed in this report, MyDigiRecords could refine their app and add in a ”Mood” section for new mothers to help gauge their QoL and stress factors throughout their postpartum journey. Then, MyDigiRecords could start to integrate the app into clinics to increase awareness and accessibility for new mothers. Lastly, in the long term, MyDigiRecords could build upon the findings from this project and align it to other vulnerable populations. Right now, MyDigiRecords works in the US and just launched in India, but there is great potential to continue to expand the app globally in the long term to serve all vulnerable populations.
QoL is multifaceted-there is a broad range of influencing factors affecting new mothers’ QoL in different and unexpected ways. However, an app like the one from MyDigiRecords can simplify the postpartum journey process for new mothers by enabling the QoL-related contributing factors. This app could mitigate the overwhelming amount of information new mothers handle, leading to fewer questions and worries all while prioritizing their QoL rather than neglecting it in this new journey. All things considered, although the studies I researched were not just limited to the US, but also included India, Iran, Spain, Saudi Arabia, and South Korea, more studies need to be conducted globally to help us better understand how to help this population with their QoL scores in the long-term and how to cushion the impact of the various existing contributing factors.
Conflicts of interest: The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgements: I would like to immensely thank my preceptors, Dr. Brian Swann and Dr. Saroj Gupta, and Chris Humphreys along with Dr. Olaf Dammann. They were all incredible resources and with their support and guidance, I was able to produce meaningful work. I thoroughly appreciated their insights and enjoyed our discussions. I hope to continue and expand this project, with a larger sample size and even other vulnerable populations to collect more data with firmer conclusions on QoL.
References
- Akhter S. Digital records must be interoperable in order to be effective: Dr Saroj Gupta, Founder, MyDigiRecords. ETHealthworld.com. 2023. https://health.economictimes.indiatimes.com/news/health-it/digital-records-must-be-interoperablein-order-to-be-effective-dr-saroj-gupta-founder-mydigirecords/100828681#:~:text=As%20an%20innovative%20health%2Dtech,decisions%20and%20improve%20health%20outcomes
- Facts about POSTPARTUM DEPRESSION. (n.d.). Retrieved from http://www.idph.state.il.us/about/womenshealth/factsheets/pdpress.htm.
- How it works - MyDigiRecords. (n.d.). MyDigiRecords. Retrieved from https://mydigirecords.com/how-it-works/.
- Jeong YJ, Nho J, Kim HY, Kim JY. Factors influencing quality of life in early postpartum women. International Journal of Environmental Research and Public Health. 2021; 18(6): 2988. https://doi.org/10.3390/ijerph18062988.
- Köhler S, Annerstedt KS, Diwan V, Lindholm L, Randive B, et al. Postpartum quality of life in Indian women after vaginal birth and cesarean section: A pilot study using the EQ-5D-5L descriptive system. BMC Pregnancy and Childbirth. 2018; 18(1). https://doi.org/10.1186/s12884-018-2038-0.
- Martínez-Galiano JM, Hernández-Martínez A, Rodríguez-Almagro J, Delgado-Rodríguez M. Quality of Life of Women after Giving Birth: Associated Factors Related with the Birth Process. Journal of Clinical Medicine. 2019; 8(3): 324. https://doi.org/10.3390/jcm8030324
- Mortazavi F, Mousavi SA, Chaman R, Khosravi A. Maternal quality of life during the transition to motherhood. Iranian Red Crescent Medical Journal. 2014; 16(5). https://doi.org/10.5812/ircmj.8443.
- Otte R, Van Beukering AJE, Boelens-Brockhuis L. Tracker-Based personal advice to support the baby’s healthy development in a novel parenting app: Data-Driven Innovation. Jmir Mhealth and Uhealth. 2019; 7(7): e12666. https://doi.org/10.2196/12666.
- Oxford Languages and Google - English. (2022, August 12). Retrieved from https://languages.oup.com/google-dictionary-en/10. Park S, Choi NK. The relationships between timing of first childbirth, parity, and health-related quality of life. Quality of Life Research. 2017; 27(4): 937-943. https://doi.org/10.1007/s11136-017-1770-7.
- Rehaili BOA, Al-Raddadi R, ALEnezi NK, ALYami AH. Postpartum quality of life and associated factors: a cross-sectional study. Quality of Life Research. 2023; 32(7): 2099-2106. https://doi.org/10.1007/s11136-023-03384-3
- Resources - MyDigiRecords. (n.d.). MyDigiRecords. Retrieved from https://mydigirecords.com/resources/
- Triviño-Juárez JM, Nieto-Pereda B, Ayuso DMR, Arruti-Sevilla B, Avilés-Gámez B, et al. Quality of life of mothers at the sixth week and sixth month postpartum and type of infant feeding. Midwifery. 2016; 34: 230-238. https://doi.org/10.1016/j.midw.2015.11.003
- Valla L, Helseth S, Småstuen MC, Misvær N, Andenæs R. Factors associated with maternal overall quality of life six months postpartum: a cross-sectional study from The Norwegian Mother, Father and Child Cohort Study. BMC Pregnancy and Childbirth. 2022; 22(1). https://doi.org/10.1186/s12884-021-04303-5.
