
Open Access, Volume 10
Is continuous chemotherapy necessary for elderly patients with chemosensitive bone-metastatic non-small cell lung cancer?
Ming Peng Luo1 ; Cong Quan Huang2*
1The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, 310014, China.
2Guangzhou Tianhe Nan Street Community Health Service Center, Guangzhou, Guang Dong, China.
Cong Quan Huang
Guangzhou Tianhe Nan Street Community Health Service Center, Guangzhou, Guang Dong, 510620, China.
Email: 514450605@qq.com
Received : Jan 05, 2024,
Accepted : Jan 26, 2024
Published : Jan 31, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Background: Bone metastases from non-small cell lung cancer pose a significant threat to elderly patients, with a certain number succumbing to this condition annually. For patients who have experienced tumor reduction post-chemotherapy, the dilemma of whether to continue chemotherapy or not becomes a confounding factor in the medical decision-making process for their families, considering the ability of elderly patients to tolerate further chemotherapy.
Objective: The purpose of this study is to investigate the quality of life in elderly patients with non-small cell lung cancer who do not undergo surgery but experience tumor reduction following chemotherapy, based on a large-sample cohort study. By comparing Overall Survival (OS) and Lung Cancer Symptom Scale (LCSS) outcomes, the study aims to provide reference recommendations to inform future medical decisionmaking.
Methods: Utilizing data from the Surveillance, Epidemiology, and End Results (SEER) database from 2010 to 2018, we selected a total of 15,870 elderly patients with non-small cell lung cancer who had not undergone surgery but had received chemotherapy for a retrospective cohort study. The follow-up duration was 4 years, during which there were multiple diagnostic records, and a subset of 33 patients demonstrated tumor size reduction when comparing two diagnostic records. We employed chi-square tests for testing differences, and Cox regression analyses were conducted to evaluate the impact of various clinico pathological factors retrieved from the database on tumor reduction, resulting in the generation of OS and LCSS curves.
Results: Compared to the reference population, significant statistical differences (P<0.05) were observed in datasets of patients experiencing tumor reduction post-chemotherapy compared to those who received chemotherapy but with ambiguous efficacy, in aspects including primary site, laterality, sex, and histology. Through univariate and multivariate Cox regression analyses, we observed that patients with ambiguous post-chemotherapy tumor reduction demonstrated a significantly higher risk of death compared to those with confirmed tumor reduction (HR=1.86, 95% CI: 1.24-2.78). In the comparative analysis of OS between patients with ambiguous versus confirmed tumor reduction post-chemotherapy, those with confirmed reduction had a significantly lower risk of death compared to the reference population [HR (95% CI): 0.640 (0.429-0.955), P=0.029 Figure 3A]. Similarly, significant differences were found in the comparison of LCSS, with patients who had confirmed tumor reduction demonstrating a notably lower risk of death compared to the reference population[HR (95%CI): 0.564 (0.364-0.874), P=0.010 (Figure 3A)].
Conclusion: Patients with lung cancer and concurrent bone metastases who experienced tumor size reduction post-chemotherapy had a decreased risk of death compared to the control group. The feasibility of intermittent chemotherapy regimens for patients sensitive to chemotherapy warrants further investigation.
Keywords: Elderly patients; Small cell lung cancer; Bone metastases; Chemotherapy; Quality of life.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Huang CQ (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Luo MP, Huang CQ. Is continuous chemotherapy necessary for elderly patients with chemosensitive bone-metastatic non-small cell lung cancer?. Open J Clin Med Case Rep. 2024; 2193.
Introduction
The incidence of non-small cell lung cancer is high, accounting for approximately 85% of all lung cancer cases [1], posing a significant threat to public health [2]. The occurrence of metastases in lung cancer cases often leaves many families in despair, with approximately one-third of non-small cell lung cancer patients presenting with metastatic disease at the time of diagnosis. The most common sites of metastasis are the bones, followed by the lungs and brain [3]. Confronted with a prognosis of advanced disease, many families are brought to the brink of despair, as prolonging life requires substantial financial support, which can be an overwhelming burden for small households [4].
In the treatment of lung cancer with bone metastasis, there is currently a lack of large-sample prospective or retrospective randomized controlled clinical trial data. Clinicians are not completely confident in determining which therapeutic efficacy is optimal when providing medical decisions, which inevitably leaves patients themselves or their families feeling at a loss when making the final medical choices.
Last year, my father, aged 54, experienced a cough with hemoptysis lasting over a month. An initial CT scan suggested a diagnosis of lung cancer. Unfortunately, following a PET/CT (FDG-whole body imaging), not only was there a tumor approximately 4.2×4.2 cm in size identified in the right middle lobe of the lung, but also evidence of bone metastasis within the ilium, as shown in Figure 1. Ultimately, histological examination confirmed the diagnosis of Non-Small Cell Lung Cancer (NSCLC). Based on our analysis, the current situation of the father is living with lung cancer with a solitary bone metastasis. According to the 2022 CSCO (Chinese Society of Clinical Oncology) guidelines in China, for patients with a Performance Status (PS) scoring of 0-1 and lung lesions classified as N2 or T4, the recommendation includes sequential or concurrent chemo radiotherapy plus radiation therapy for bone metastatic lesions, combined with bisphosphonate or denosumab treatment, in addition to systemic chemotherapy (Category 2B evidence). Studies have shown that patients undergoing this treatment approach can benefit, with a median survival time of 13.5-14 months and overall survival rates at 1, 2, and 3 years of 58.1%, 24.8%, and 15.8%, respectively [5-7]. After medical decision-making discussions, my father underwent treatment with paclitaxel and carboplatin chemotherapy in conjunction with toripalimab immunotherapy, administered every 20 days. The treatment course proceeded smoothly with no significant discomfort. Following three treatment cycles, PET/CT (FDG-whole body imaging) revealed a marked reduction in the lesions, as illustrated in Figure 1. However, it is disheartening that my father experienced significant hair loss, which inevitably raises concerns regarding the toxic side effects of chemotherapy.
Currently, the dilemma we are facing is how to proceed with the treatment of elderly patients with isolated bone metastases from lung cancer who have demonstrated significant reduction in tumor size following chemotherapy. We do not subscribe to the notion of accepting a «countdown to life» prognosis. Can such patients undergo surgical removal of the primary lesion followed by continued chemotherapy? Should chemotherapy be continued, and how many cycles of chemotherapy can a patient tolerate at maximum? What is the eventual progression in such scenarios, and how long can my father live? This study has gathered data on elderly patients with non-small cell lung cancer with isolated metastases who received chemotherapy through a retrospective survey of a large sample database, and statistical analysis has been conducted, which may provide some references for clinical practice and medical decision-making.
Materials and Methods
Patient selection
We searched for and downloaded medical records of elderly lung cancer patients from the SEER database (SEER Research Plus Data, 18 Registries, Nov 2020 Sub, 2000-2018 & SEER Research Plus Data, 17 Registries, Nov 2021 Sub, 2000-2019), which covers cancer incidence and survival data for more than one-third of the US population [8]. The objective of our study was to explore the overall survival outcomes of patients diagnosed with non-small cell lung cancer between 2010 and 2018 who did not undergo surgical intervention and received chemotherapy. We set a four-year follow-up duration to ensure that each patient was observed for at least four years. The screening process was mainly divided into three steps: the first step was to select patients from the database with multiple diagnoses and to extract data for patients sensitive to chemotherapy by comparing the size of the tumors at diagnosis. The second step was to select patients with only one diagnostic record; these patients were considered to have received just one treatment, and the sensitivity of the tumor to chemotherapy could not be determined through comparison of diagnostic information, thus they were only used as a reference group. The third step was to combine the patient data obtained from the first and the second steps for statistical analysis.
In the first step, we filtered for elderly patients with non-small cell lung cancer who were sensitive to chemotherapy and had not undergone surgery, using the following criteria: (a) We downloaded data for all lung cancer patients over 50 years of age from 2010 to 2018, totaling 870,785 cases. We then selected patients with multiple entries of the same Patient ID within these cases. (b) We excluded patients whose sequence number was not «1st of 2 or more primaries» or «2nd of 2 or more primaries.» (c) We excluded patients who had only bone metastases without other metastatic sites. (d) We excluded patients not diagnosed with non-small cell lung cancer. (e) We excluded patients who had undergone surgical treatment. (f) We excluded patients who had not received chemotherapy. (g) We compared tumor size information from the first and second diagnoses and excluded patients whose tumor size did not decrease or for whom it was not possible to ascertain any change.
In the second step, we selected lung cancer patients who met the following criteria: (a) The sequence number was «one primary only.» (b) The diagnosis occurred between 2010 and 2018. (c) The site of the malignancy was specified as lung and bronchus. (d) The age was over 50 years old. (e) We excluded patients who had only bone metastases without other metastatic sites. (f) We excluded patients not diagnosed with non-small cell lung cancer. (g) We excluded patients who had undergone surgical treatment. (h) We excluded patients who had not received chemotherapy
In the third step, we merged the two datasets obtained from the above procedures. The flowchart representing the inclusion and exclusion process for participants is depicted in Figure 1. This study did not require ethical approval, as the clinical data of the recruited lung cancer patients were collected from the open-access and anonymized dataset of the public SEER database.
Variable description
The study population consisted of elderly patients who were diagnosed with non-small cell lung cancer with bone metastases within the period from 2010 to 2018, who did not receive surgical treatment but did receive chemotherapy, with an observation period of four years. (1) The clinical-pathologic factors to be analyzed included: (a) Year of diagnosis (2010-2018). (b) Primary site (lower lobe, upper lobe, others). (c) Laterality (left, right, others). (d) Age at diagnosis (51-60, 61-70, 71-80, 81+ years). (e) Race (White, Black, others). (f) Histologic type (adenocarcinoma, squamous cell carcinoma, non-small cell carcinoma not otherwise specified). (g) Tumor size (0-3 cm, 3-6 cm, 6+ cm, unknown/others). (h) Radiotherapy (Yes, None/Unknown). (i) Stage (I-II, III-IV, unknown). (j) Marital status (married, single, others). (2) The outcome variables were: (a) Interval Time. (b) Vital status.
Statistical analysis
This study was a retrospective cross-sectional survey that included statistical analysis. Characteristics of patients or tumors were expressed as percentages and data was ultimately analyzed using Chi-square test or Fisher’s exact test for statistical significance. A difference was considered statistically significant when p<0.05. All statistical analyses were performed using SPSS software, version 25.0. To analyze the impact of each predictor on overall survival, univariate and multivariate Cox regression analyses were performed on the entire dataset using SPSS version 25.0. Kaplan-Meier analysis was utilized to assess both the overall survival and disease-specific survival of all patients.
Results
Baseline characteristics of enrolled patients: A total of 15,903 patients were ultimately screened. Among them, there were 33 patients with multiple diagnostic records showing a definite decrease in tumor size post-chemotherapy, and there were 15,870 patients with bone metastases from lung cancer who underwent chemotherapy and had only one diagnostic record; the latter group was used as the reference cohort, as seen in Table 1. It is not difficult to ascertain from the table that the number of patients in the dataset with multiple diagnoses exhibiting a clear tumor shrinkage is low, being only 33 cases, and the annual frequencies were not stable, with zero occurrences reported from 2016 to 2018. Due to the low frequency, only a preliminary reference could be made. There were statistically significant differences (P<0.05) between the dataset of patients experiencing tumor shrinkage post-chemotherapy and those who underwent chemotherapy without a clear assessment of its effect in terms of primary site, laterality, sex, and histology, when compared to the reference group. It is important to note that the population with a definite decrease in tumor size was predominantly male, constituting 75.76%. The most frequently occurring age subgroup was 71-80 years old, accounting for 39.39%. Among histologic types, adenocarcinoma was the most prevalent, representing 42.42%.
Univariate and multivariate Cox regression analyses with tumor reduction post-chemotherapy as the outcome
As presented in Table 2, we conducted univariate and multivariate Cox regression analyses on some predictors with statistically significant differences. Regarding the primary site, the risk of death was higher for the lower lobe compared to the upper lobe (HR=1.07, 95% CI: 1.03-1.12). As for laterality, no statistical difference was found in the influence on tumor reduction between left and right-sided tumors (multivariate regression: P=0.101). Concerning sex, female patients had a lower risk of death compared to male patients (HR=0.80, 95% CI: 0.78-0.83). In terms of histology, squamous cell carcinoma showed no statistical difference in the risk of death compared to unspecified non-small cell lung cancer in the multivariate regression analysis (P=0.197); however, adenocarcinoma had a slightly lower risk of death (HR=0.72, 95% CI: 0.68-0.76). Notably, regarding tumor shrinkage after chemotherapy, the risk of death was significantly higher in the patient population where tumor reduction was not clear compared to those with a definite reduction following chemotherapy (HR=1.86, 95% CI: 1.24-2.78).
OS and LCSS
In the analysis comparing Overall Survival (OS) between patients with non-clear versus definite tumor shrinkage post-chemotherapy, those with definite tumor reduction exhibited a significantly lower risk of death compared to the reference cohort [HR (95% CI): 0.640(0.429-0.955), P=0.029. See Figure 3A]. Similarly, significant differences were observed when comparing Lung Cancer-Specific Survival (LCSS), with patients who had definite tumor shrinkage demonstrating a significantly lower risk of death compared to the reference cohort [HR (95% CI): 0.564(0.364 - 0.874), P=0.010. Refer to Figure 3A].
Table 1: Statistical description of the dataset for the overall population after conducting a chi-square test.
| Variable | Total (n=15903) |
Has the tumor reduced in size following treatment? |
P | ||
|---|---|---|---|---|---|
| Unknown (n=15870) | Yes (n=33) | ||||
| Year of diagnosis, n (%) | - | <.001 | |||
| 2010 | 1644(10.34) | 1637(10.32) | 7(21.21) | ||
| 2011 | 1660(10.44) | 1656(10.43) | 4(12.12) | ||
| 2012 | 1667(10.48) | 1659(10.45) | 8(24.24) | ||
| 2013 | 1824(11.47) | 1816(11.44) | 8(24.24) | ||
| 2014 | 1841(11.58) | 1839(11.59) | 2(6.06) | ||
| 2015 | 1923(12.09) | 1919(12.09) | 4(12.12) | ||
| 2016 | 1923(12.09) | 1923(12.12) | 0(0.00) | ||
| 2017 | 1672(10.51) | 1672(10.54) | 0(0.00) | ||
| 2018 | 1749(11) | 1749(11.02) | 0(0.00) | ||
| Primary Site, n(%) | χ²=6.966 | 0.031 | |||
| Lower lobe | 4094(25.74) | 4080(25.71) | 14(42.42) | ||
| Upper lobe | 8550(53.76) | 8533(53.77) | 17(51.52) | ||
| Others | 3259(20.49) | 3257(20.52) | 2(6.06) | ||
| Laterality, n(%) | χ²=6.364 | 0.041 | |||
| Left | 6371(40.06) | 6351(40.02) | 20(60.61) | ||
| Right | 8955(56.31) | 8942(56.35) | 13(39.39) | ||
| Others | 577(3.63) | 577(3.64) | 0(0.00) | ||
| Sex, n(%) | χ²=4.080 | 0.043 | |||
| Female | 6608(41.55) | 6600(41.59) | 8(24.24) | ||
| Male | 9295(58.45) | 9270(58.41) | 25(75.76) | ||
| Age, n(%) | χ²=2.324 | 0.508 | |||
| 51-60 | 4094(25.74) | 4088(25.76) | 6(18.18) | ||
| 61-70 | 6088(38.28) | 6076(38.29) | 12(36.36) | ||
| 71-80 | 4498(28.28) | 4485(28.26) | 13(39.39) | ||
| 81+ | 1223(7.69) | 1221(7.69) | 2(6.06) | ||
| Race, n(%) | - | 0.053 | |||
| White | 12495(78.57) | 12464(78.54) | 31(93.94) | ||
| Black | 1756(11.04) | 1756(11.06) | 0(0.00) | ||
| Others/Unknown | 1652(10.39) | 1650(10.40) | 2(6.06) | ||
| Histology, n(%) | χ²=28.455 | <.001 | |||
| Adenocarcinoma | 11400(71.68) | 11386(71.75) | 14(42.42) | ||
| Squamous cell carcinoma | 2966(18.65) | 2959(18.65) | 7(21.21) | ||
| Non-small cell carcinoma, NOS | 1537(9.66) | 1525(9.61) | 12(36.36) | ||
| Grade, n(%) | χ²=2.329 | 0.312 | |||
| I-II | 1824(11.47) | 1823(11.49) | 1(3.03) | ||
| III-IV | 3422(21.52) | 3414(21.51) | 8(24.24) | ||
| Unknown | 10657(67.01) | 10633(67.00) | 24(72.73) | ||
| Radiotherapy, n(%) | χ²=0.014 | 0.907 | |||
| None/Unknown | 6906(43.43) | 6892(43.43) | 14(42.42) | ||
| Yes | 8997(56.57) | 8978(56.57) | 19(57.58) | ||
| Marital status, n(%) | χ²=2.409 | 0.3 | |||
| Married | 9195(57.82) | 9172(57.79) | 23(69.70) | ||
| Single | 2165(13.61) | 2163(13.63) | 2(6.06) | ||
| Others | 4543(28.57) | 4535(28.58) | 8(24.24) | ||
Table 2: Results of univariate and multivariate COX regression analyses on the dataset of the total population.
| Variables | Beta | S.E | Z | P | HR (95% CI) | m_Beta | m_S.E | m_Z | aP | aHR (95% CI) |
|---|---|---|---|---|---|---|---|---|---|---|
| Primary Site | ||||||||||
| Upper lobe | Ref | Ref | ||||||||
| Lower lobe | 0.06 | 0.02 | 2.87 | 0.004 | 1.06 (1.02-1.11) | 0.07 | 0.02 | 3.33 | <.001 | 1.07 (1.03-1.12) |
| Others | 0.2 | 0.02 | 8.7 | <.001 | 1.22 (1.16-1.27) | 0.19 | 0.02 | 7.81 | <.001 | 1.21 (1.15-1.26) |
| Laterality | ||||||||||
| Left | Ref | Ref | ||||||||
| Right | 0.04 | 0.02 | 2.34 | 0.02 | 1.04 (1.01-1.08) | 0.03 | 0.02 | 1.64 | 0.101 | 1.03 (0.99-1.07) |
| Others | 0.18 | 0.05 | 3.66 | <.001 | 1.19 (1.08-1.31) | 0.03 | 0.05 | 0.61 | 0.54 | 1.03 (0.93-1.14) |
| Sex | ||||||||||
| Male | Ref | Ref | ||||||||
| Female | -0.27 | 0.02 | -14.89 | <.001 | 0.77 (0.74-0.79) | -0.22 | 0.02 | -12.02 | <.001 | 0.80 (0.78-0.83) |
| Histology | ||||||||||
| Non-small cell carcinoma, NOS | Ref | Ref | ||||||||
| Adenocarcinoma | -0.33 | 0.03 | -11.54 | <.001 | 0.72 (0.68-0.76) | -0.33 | 0.03 | -11.32 | <.001 | 0.72 (0.68-0.76) |
| Squamous cell carcinoma | 0.08 | 0.03 | 2.36 | 0.018 | 1.08 (1.01-1.15) | 0.04 | 0.03 | 1.29 | 0.197 | 1.04 (0.98-1.11) |
| Reduced in size following treatment? | ||||||||||
| Yes | Ref | Ref | ||||||||
| No | 0.45 | 0.2 | 2.18 | 0.029 | 1.56 (1.05-2.33) | 0.62 | 0.2 | 3.02 | 0.002 | 1.86 (1.24-2.78) |
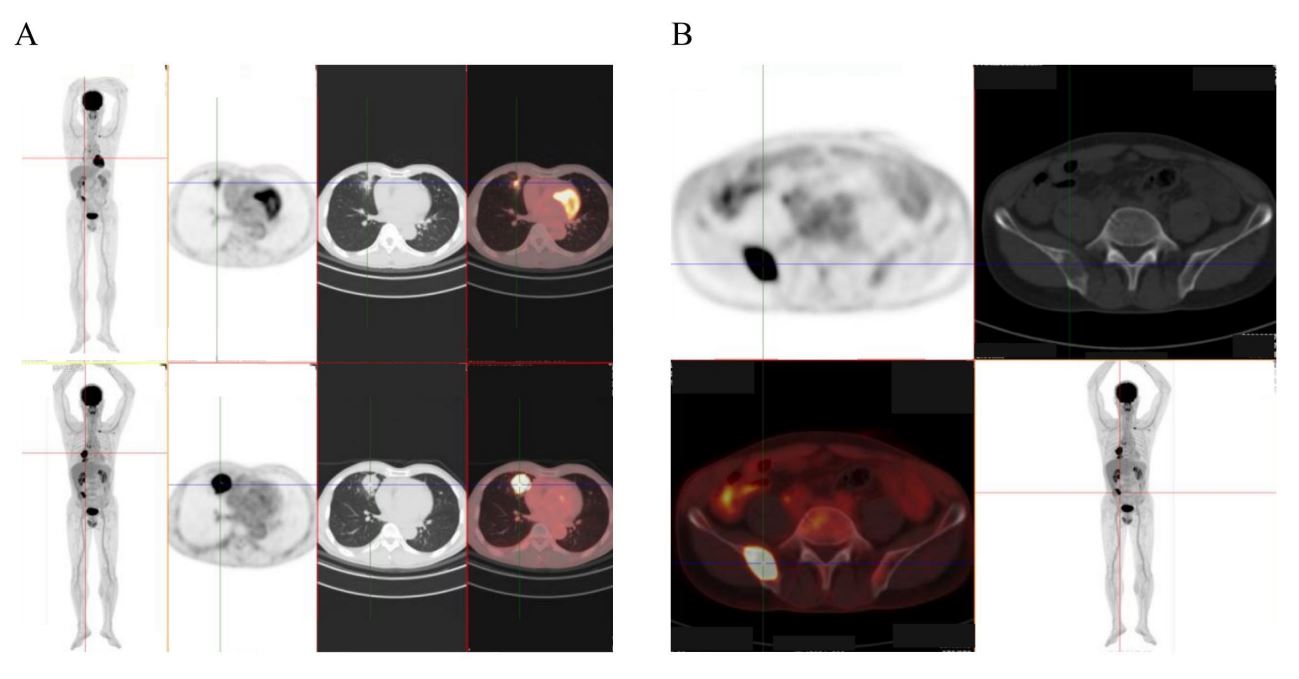
Figure 1: PET/CT images. (A) Changes in tumor size before and after treatment. (B) PET/CT images of metastatic lesions.
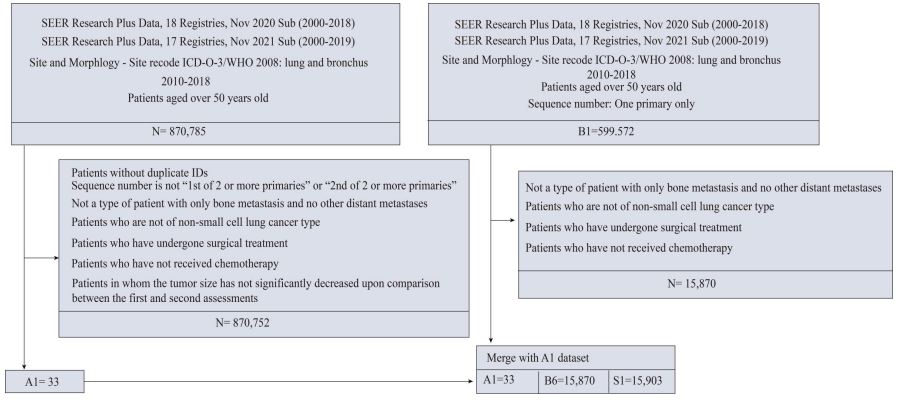
Figure 2: The flow diagram of participant inclusion and exclusion.
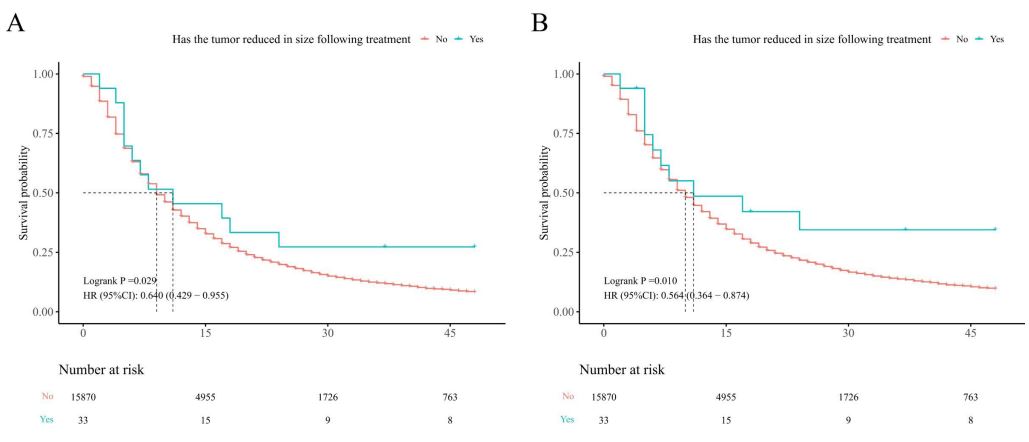
Figure 3: Comparison of Overall Survival (OS) (A) and Lung Cancer-Specific Survival (LCSS) (B) between patients with posttreatment tumor shrinkage and those with only a single diagnostic record.
Discussion
Following significant reduction of isolated metastatic foci post-chemotherapy in lung cancer, the suggestion of surgical resection of the primary lesion might be contemplated. It cannot be denied that there are reservations to consider when making such a decision. The substantial trauma of surgical resection could potentially impact the patient’s subsequent quality of life. Could the immunosuppression post-resection promote the enlargement of metastatic foci? In the absence of surgical removal, should chemotherapy be continued? Given that chemotherapy itself is harmful to the body and can lower immune function, could this immunosuppression lead to a rebound of the primary or metastatic tumor sites? Alternatively, after alleviation of hemoptysis and significant tumor reduction, might it be feasible for the patient to enjoy a period of recovery, allowing for a pause in treatment before continuing to observe and proceed with the next phase of chemotherapy after some time? Or, during this recuperative interval, could immunotherapy alone be employed?
In the study presented herein, patients who exhibited definitive shrinkage demonstrated significantly lower risk values for both Overall Survival (OS) and Lung Cancer-Specific Survival (LCSS) as compared to the control population. This indicates that in the cohort of lung cancer patients with bone metastases who did not undergo surgical intervention but only received chemotherapy, the risk of death for those demonstrating significant reduction of the primary lesion is reduced relative to the entire chemotherapytreated population.
Analysis of the SEER database yields some optimistic findings. Regrettably, sufficient data for analysis was available from only 33 cases, and thus, references can only be sought from these 33 instances where definite tumor shrinkage was documented. We recognize various categories of chemotherapy including curative, palliative, adjuvant, Neoadjuvant, and concurrent chemo radiation. Given that surgery often necessitates the removal of lung lobes, or even a hemi lobectomy, which affects the quality of life for elderly patients, many patients and their families have reservations about this. Therefore, for patients who are reluctant to undergo surgery, is it viable to persist with chemotherapy indefinitely? We know that most patients upon hospital admission, aside from symptoms caused by lung pathology such as hemoptysis and cough, have largely normal organ functions. However, after several rounds of chemotherapy, patients can rapidly deteriorate and often succumb shortly thereafter. Should tumor shrinkage and the resolution of symptoms like hemoptysis and cough post-chemotherapy prompt consideration for de-escalating chemotherapy intensity and shifting toward less toxic immunotherapy?.
Due to the nephrotoxic and dose-related neurotoxic properties of chemotherapeutic agents [9], persisting with chemotherapy in a mechanical manner may not be the most judicious treatment approach. How to balance the benefits of chemotherapy-induced tumor shrinkage against the adverse effects of chemotherapy-induced systemic functional decline is an issue that warrants consideration. According to standard recommended chemotherapy protocols, one cycle of therapy consists of 3-4 administrations, with each spaced 3-4 weeks apart; thus, a complete cycle can be achieved within a maximum period of 4 months. Consequently, it might be plausible to consider interrupting chemotherapy for a period, such as administering only one cycle per annum, with the remainder of the year substituted by immunotherapy. From our previous OS analysis, the median survival time for patients with only a single diagnostic record was 10 months (95% CI=10-10), whereas the median survival time for patients showing definitive tumor reduction post-chemotherapy was 11 months (95% CI=6-NA). Based on these findings, we can conclude that half of the elderly patients suffering from Non-Small Cell Lung Cancer (NSCLC), who have not undergone surgery but have received chemotherapy, may survive beyond 10 months. Thus, the determination of treatment strategies to further extend survival is of significant concern.
The most common metastasis in lung cancer occurs in the bones [10], typically accompanied by pain and reduced mobility in patients [11]. If a patient maintains a Karnofsky Performance Scale (KPS) score of ≥60% post-chemotherapy, and does not experience persistent bone pain symptoms, does it imply that chemotherapy could be intermittently paused after one treatment cycle? Some literature provides support for this proposition. A study conducted by Laura Visa et al. found that the efficacy of a reduced-intensity chemotherapy regimen suited for patients aged ≥70 years was comparable to that of younger patients. Modifying the schedule to reduce the toxicity of chemotherapy is considered beneficial and prudent in a more vulnerable population [12]. Jeffrey Crawford et al. through a retrospective cohort study, investigated the impact of chemotherapy dosing patterns on the actual treatment outcomes in patients with advanced non-small cell lung cancer. The results indicated that a dose delay of ≥7 days was significantly associated with a 29.0% reduction in the risk of mortality (P<0.0001) [13]. Despite defining chemotherapy delay as merely 7 days rather than a month or even a quarter, these findings underscore the importance of understanding dose intensity’s impact on overall survival quality for managing toxicity and improving survival rates. Kenji Morimoto et al. conducted a 14-month retrospective survey of 249 patients with non-small cell lung cancer and discovered that there was no significant difference in Overall Survival (OS) between the group that terminated induction chemotherapy early and the group that completed at least four cycles of induction chemotherapy [14]. Mitsuhiro Kamiyoshihara and colleagues reported the diagnostic and treatment course of a patient with recurrent non-small cell lung cancer, who experienced a mediastinal lymph node recurrence 12 months post-surgery. The patient was subsequently treated with pembrolizumab monotherapy for 24 months, during which the disease did not progress. The tumor continued to shrink even after cessation of pembrolizumab treatment [15]. In conclusion, if patients switch to monoclonal antibody monotherapy after several cycles of chemotherapy, providing them with a period for physiological recovery, such as an interval of 3 to 6 months, may be a chemotherapy regimen worth investigating.
Lastly, it is undeniable that our study has certain limitations. The SEER database does not provide records of the number of metastases, targeted therapy, presence of tumor necrosis, underlying comorbidities, or family history. The chemotherapy regimen we propose is considered with the intent to minimize physical harm to the fullest extent; however, we lack more authoritative prospective research currently. This proposal can only offer a reference for clinical decision-making by physicians, patients, and their families. Whether it should be adopted requires further investigation.
Conclusion
(1) Patients with lung cancer and bone metastases who experience a reduction in tumor size following chemotherapy have a decreased risk of mortality compared to the control population.
(2) For patients with chemotherapy-sensitive tumors and mild symptoms, intermittent chemotherapy regimens merit further investigation.
Funding: The work was supported by Research on Xiyue Medicine.
References
- Leiter A, Veluswamy RR, Wisnivesky JP. The global burden of lung cancer: Current status and future trends. Nat Rev Clin Oncol. 2023; 20(9): 624-39.
- Rodak O, Peris-Díaz MD, Olbromski M, Podhorska-Okołów M, Dzięgiel P. Current Landscape of Non-Small Cell Lung Cancer: Epidemiology, Histological Classification, Targeted Therapies, and Immunotherapy. Cancers (Basel). 2021; 13(18).
- Tamura T, Kurishima K, Nakazawa K, Kagohashi K, Ishikawa H, Satoh H, et al. Specific organ metastases and survival in metastatic non-small-cell lung cancer. Mol Clin Oncol. 2015; 3(1): 217-21.
- Chou E, Ganti AK, Katranji K, Cotarla I, Sharma C, et al. OFP01.09 Economic Burden of Metastatic Non-Small Cell Lung Cancer (mNSCLC) in a Large United States (US) Claims Database. J Thorac Oncol. 2021; 16(1): S11-2. Available from: https: //doi.org/10.1016/j.jtho.2020.10.041
- De Ruysscher D, Wanders R, van Baardwijk A, Dingemans A-MC, Reymen B, et al. Radical treatment of non-small-cell lung cancer patients with synchronous oligometastases: long-term results of a prospective phase II trial (Nct01282450). J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2012; 7(10): 1547-55.
- Ouyang W-W, Su S-F, Ma Z, Hu Y-X, Lu B, et al. Prognosis of non-small cell lung cancer patients with bone oligo metastases treated concurrently with thoracic three-dimensional radiotherapy and chemotherapy. Radiat Oncol. 2014; 9: 147.
- Griffioen GHMJ, Toguri D, Dahele M, Warner A, de Haan PF, et al. Radical treatment of synchronous oligometastatic non-small cell lung carcinoma (NSCLC): Patient outcomes and prognostic factors. Lung Cancer. 2013; 82(1): 95-102.
- Wu J, Wang Z, Jing C, Hu Y, Yang B, et al. The incidence and prognosis of thymic squamous cell carcinoma: A Surveillance, Epidemiology, and End Results Program population-based study. Medicine (Baltimore). 2021; 100(15): e25331.
- Sul JK, Deangelis LM. Neurologic complications of cancer chemotherapy. Semin Oncol. 2006; 33(3): 324-32.
- Cho YJ, Cho YM, Kim SH, Shin K-H, Jung S-T, et al. Clinical analysis of patients with skeletal metastasis of lung cancer. BMC Cancer. 2019; 19(1): 303.
- Radeczky P, Moldvay J, Fillinger J, Szeitz B, Ferencz B, et al. Bone-Specific Metastasis Pattern of Advanced-Stage Lung Adenocarcinoma According to the Localization of the Primary Tumor. Pathol Oncol Res. 2021; 27: 1609926.
- Visa L, Jiménez-Fonseca P, Martínez EA, Hernández R, Custodio A, et al. Efficacy and safety of chemotherapy in older versus non-older patients with advanced gastric cancer: A real-world data, non-inferiority analysis. J Geriatr Oncol. 2018; 9(3): 254-64.
- Crawford J, Denduluri N, Patt D, Jiao X, Morrow PK, et al. Relative dose intensity of first-line chemotherapy and overall survival in patients with advanced non-small-cell lung cancer. Support care cancer Off J Multinatl Assoc Support Care Cancer. 2020; 28(2): 925-32.
- Morimoto K, Uchino J, Yokoi T, Kijima T, Goto Y, et al. Early discontinuation of induction therapy in chemoimmunotherapy as an effective alternative to the standard regimen in patients with non-small cell lung cancer: A retrospective study. J Cancer Res Clin Oncol. 2022; 148(9): 2437-46.
- Kamiyoshihara M, Igai H, Matsuura N, Ohsawa F, Numajiri K. Recurrent Postoperative Lung Cancer with Tumor Shrinkage after Discontinuation of Pembrolizumab-A Case Report. Gan to Kagaku Ryoho. 2022; 49(1): 67-9.
