
Open Access, Volume 10
A case of patient with decompensated Budd-Chiari syndrome treated with T-TIPS: A case report
Bevilacqua Michele1,2*; Gasparini Clizia3; Cortellini Nino3; Cattazzo Filippo1; Roberta Stupia1; Leonardo De Marco1; Andrea Dalbeni1,2; Donatella Ieluzzi2; Irene Zagni4; Paolo Bonfante4; Mansueto Giancarlo3; Alberto Contro3; Sacerdoti David2
1Department of Medicine, General Medicine C, University of Verona, Verona Integrated University Hospital, Verona, Italy.
2Department of Medicine, Liver Unit, University and Azienda Ospedaliera Universitaria Integrata of Verona, Italy.
3Department of Diagnostics and Public Health, Radiology and Interventional Radiology Unit, University and Azienda Ospedaliera Universitaria Integrata of Verona, Italy.
4Departement of Internal Medicine, Desenzano Hospital, Italy.
Bevilacqua Michele
Department of Medicine, General Medicine C, University of Verona, Verona Integrated University Hospital,
Verona, Italy.
Email: bevilacqua.michele92@gmail.com
Received : Dec 30, 2023,
Accepted : Jan 23, 2024
Published : Jan 31, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Michele B (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Michele B, Clizia G, Nino C, Filippo C, Stupia R, De Marco L, Dalbeni A, et al. A case of patient with decompensated Budd-Chiari syndrome treated with T-TIPS: A case report. Open J Clin Med Case Rep. 2024; 2191.
Case Report
A 46-years old man with a recent onset of painful hepatomegaly and abdominal swelling was referred to the emergency department and hospitalized in the internal medicine ward for a diagnostic hepatological work-up. He had no clinically significant previous medical history, except for a mild long-standing polycitemia. When admitted to hospital, he was febrile but hemodynamically stable (blood pressure 100/60 mmHg, pulse rate 90/min) and had a satisfactory blood oxygen saturation levels in room air. At clinical examination, he was slightly sub-icteric; a palpable but tender hepatomegaly together with a significant abdominal effusion and a mild leg swelling were noticed. In order to evaluate different possible causes of liver disease, alcoholic, viral, autoimmune, metabolic and congenital etiologies were excluded, mainly by biochemical tests.
Common blood tests revealed impressive polycitemia (haemoglobin 19 g/dL) and thrombocythemia (700.000 platelets/mm3 ), normal renal function, mild hypoalbuminemia (30 g/L), hyperbilirubinemia (total bilirubin 3 mg/dL with direct bilirubin 2.5 mg/dL) and mild hypertransanasemia (AST 76 U/L) with slightly elevated International Normalized Ratio (INR 1.3). Abdominal Color-Doppler Ultrasound (US) showed moderate-to-severe ascites, normal spleen size (polo-polar diameter 11.5 cm), global hepatomegaly and caudate lobe hypertrophy (8.5 cm, with caudate lobe vein enlarged, 4 mm) with inhomogeneous ecostructure, patent extra-and intra-hepatic portal vein with markedly reduced hepatopetal portal flow, large intra-hepatic collaterals without detectable supra-hepatic veins. Hepatic and splenic shear wave-based elastometries (SW) were significantly elevated (liver SW 25 kPa, spleen SW 35 kPa). An abdominal MRI scan was performed, and beyond confirming the clinical and US-based suspicion of Budd-Chiari syndrome, revealed a significant thrombotic stenosis of the intra-hepatic tract of the Inferior Vena Cava (IVC).
A complete diagnostic work-up for haematological disorders and congenital or acquired thrombophilia showed the presence of JAK-2 positive myeloproliferative disease (unspecific features of both essential trombocythemia and polycitemia on bone marrow biopsy) together with Leiden’s Factor V mutation. Small oesophageal varices without red wale marks and hypertensive gastropathy were detected at endoscopic evaluation.
Oral anticoagulation with vitamin K antagonists, cyto-reductive therapy with low-dose hydroxyurea and diuretics (either loop diuretics and k+ sparing drugs) were initiated. Good short and long-term prognosis was estimated by calculating classical risk scores (Rotterdam BCS index 1.0, Clichy prognostic index 4). Since blood biochemistry did not improve over time and the patient required paracentesis for symptomatic tense ascites despite optimal medical therapy (Child-Pugh B9-C10), a work-up evaluation for TransJugular Intra-Hepatic Porto-Systemic shunt (TIPS) placement was done. Significant cardiac systo-diastolic dysfunction as well as pulmonary hypertension were excluded performing a trans-thoracic echocardiography. After a detailed multidisciplinary discussion with the interventional radiologist we concluded that the classical direct trans-jugular and trans-caval approaches for stent placement were not feasible because of an unexpectedly hard fibrotic wall of the intra-hepatic IVC. For this reason, 2 metal guides, were previously placed inside the IVC (via trans-jugular route) and the right portal branch (through a trans-hepatic access) and then connected by another percutaneously-inserted needle (Gun-Sight technique) to create the final 8 millimeter-dilated and 6 cm-long TTIPS (Trans-Jugular Trans-Caval Intra-Hepatic Porto-Systemic shunt) implantation (Figure 1). At the end of the procedure, a contrast medium-based fluoroscopy confirmed both the patency and the correct functioning of the shunt, with nearly no portal flow through hepatic parenchyma. A CT scan after TTIPS placement showed a well-placed stent between IVC and portal bifurcation without any procedure-related complications. After 1 month, a significant clinical and biochemical amelioration was noticed: the ascites disappeared and blood tests (transaminases and bilirubin) were normalized. A focused Color-Doppler US showed a patent stent with normal-velocity hepatofugal blood flow (peak medium velocity from 90 cm/s in proximal/medial tract to 140 cm/s in distal part of the TTIPS, see Figure 2) and a significant decrease in hepatic and splenic stiffness and arterial resistance indexes (for liver: 25 to 12 kPa and RI 0.75 to 0.52; for spleen 35 to 25 kPa and RI 0.73 to 0.48), suggesting effective splanchnic decongestion and amelioration of portal hypertension (Figure 2). The patient discontinued diuretic therapy and a direct oral anticoagulant with a full dosage of apixaban was started; since the risk of thrombosis and TIPS dysfunction, the patient is undergoing a biochemical and US follow-up every three months; he is still fine.
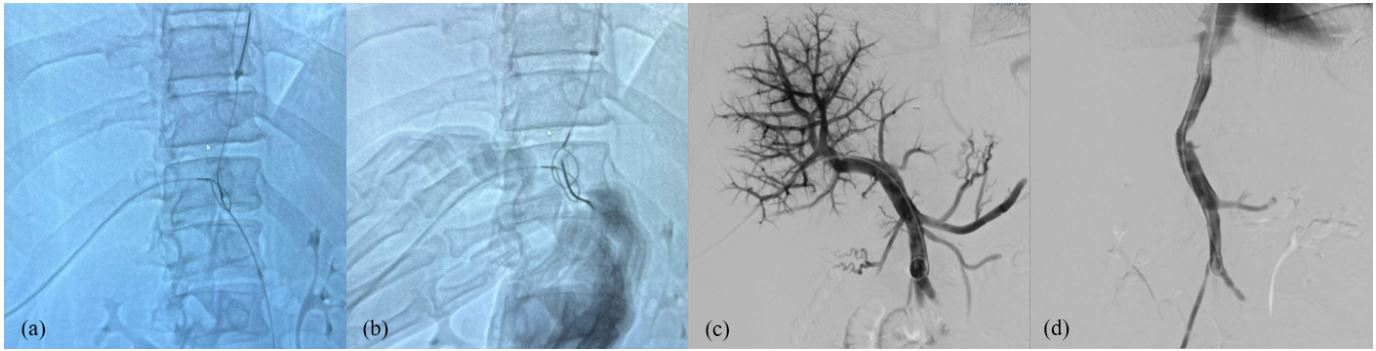
Figure 1: “Gun-Sight technique” by Haskal and colleagues;
(a) Overlapping two snares introduced from a transjugular access and a transhepatic access, respectively, and using them as
a fluoroscopy- guided target (“Gun-sight”) for a percutaneous transabdominal needle puncture.
(b) A guidewire is then “hooked” through the snares and withdrawn from the percutaneous transjugular access.
(c) A through-and-through access (transhepatic and transjugular) is obtained.
(d) Balloon dilation of the TIPS parenchymal tract. (e,f) Release of a covered PTFE stent through the trans-jugular access.
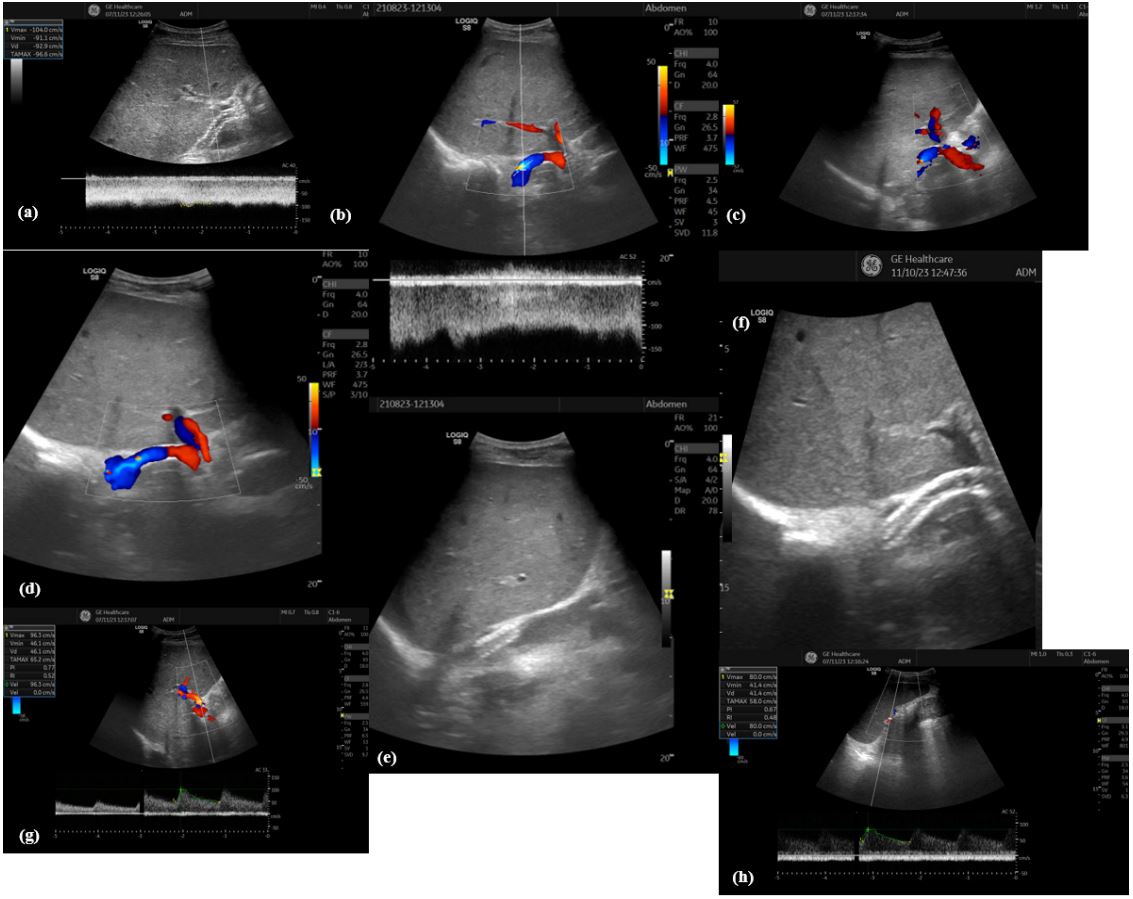
Figure 2: Hepatic hemodynamic after T-TIPS. (a) Right branch of portal vein with hepatofugal flow after TTIPS entrance;
(b,c,d). show patent TTIPS with normal flow velocity and slight flow turbolence in the distal part of the shunt; distal end of
the TTIPS directly enter in IVC in (e,f); very low arterial Resistance Index (RI) of both liver (g) and spleen (h) after TTIPS,
demonstrating highly effective decongestion of the splanchnic district.
Discussion
In recent years, TIPS placement has been increasingly recognized as a safe and effective treatment of portal hypertension-related complications, especially in the setting of decompensated cirrhosis, such as refractory ascites (i.e resistant or intractable) and severe or recurrent variceal gastro-intestinal bleeding (rescue and early/pre-emptive TIPS) [1]; moreover, despite a lower amount of literature evidences, TIPS can be considered as a treatment option for hepatic hydrothorax, hepato-renal syndrome, severe hyponatremia, gastro-intestinal bleeding other than those related to gastro-oesophageal varices and both acute and chronic portal vein thrombosis [2]. Similarly to decompensated cirrhosis, the rationale for TIPS in Budd-Chiari syndrome is to rapidly improve portal hypertension, significantly decreasing liver-related complications (ascites, bleeding and hepatic encephalopathy, need for liver transplant) and improving short-and long term survival [3]. Compared to the he high feasibility of TIPS procedure in cirrhosis, the abnormal venous anatomy of patients with Budd-Chiari syndrome has raised some technical concerns, especially in those with completely thrombosed supra-hepatic veins and IVC involvement. In these cases, a transcaval approach has been shown, almost 20 years ago, to be the first choice to achieve a clinically significant decrease of hepatic congestion and, consequently, portal hypertension and liver-related morbidity and mortality [4]. In previous years, many different procedures were described, such as a direct fluoroscopy-guided puncture of both portal vein and IVC with a single needle-catheter or using a intravascular or trans-abdominal US-guided catheter for reaching the portal bifurcation from the IVC and a trans-hepatic access to allocate the stent [5]. In our case, a successfully treated patient with decompensated Budd-Chiari syndrome with a Trans-Jugular Trans-Caval Intra-Hepatic Shunt (TTIPS) is shown. Because of the impossibility to punch the fibrotic wall of the inferior vena cava (old thrombosis), two guidewires were placed in portal vein and IVC lumens by a trans-jugular and percutaneous access, respectively. Then, they were aligned and captured by a third metallic guide through an epigastric trans-cutaneous puncture obtaining a direct route from IVC to the portal vein which allows the release of a covered PTFE stent through the classical trans-jugular access.
TTIPS and DIPS [6] (i.e. direct intra-hepatic porto-caval shunt), a similar procedure in which a stent is put directly through an hepatic puncture to create a porto-caval shunt [7], have been shown to be quite difficult procedures and, in some series, associated with an increased risk of complications, such as retroperitoneal and sub-capsular bleeding, intra-hepatic hematoma, acute renal and hepatic failure [3,5]. However, in expert centers, TTIPS and DIPS are relatively safe procedures. As regards cirrhosis-related portal hypertension, only few series of patients were shown to obtain favourable results with TTIPS or DIPS, especially in terms of ascites and bleeding, reduced risk of stent thrombosis and major decrease of portal pressure (in both cases probably mainly due to the lower length of the prothesis), and this could encourage to consider this procedures as a valid alternative to conventional TIPS in presence of anatomic abnormalities [5]. On the contrary, in more than half of Budd-Chiari syndrome patients, conventional TIPS is not possible mainly because of the complete occlusion of supra-hepatic veins and the absence of at least one of their “remnants” near the ostium of IVC. In these patients, TTIPS and DIPS are considered the first choice, also when portal vein thrombosis is present [8]; and in many previous reports different techniques were demonstrated [9-11]. In this case and for the first time in our hospital, a Gun-Sight approach was used, as firstly described in 1996 by Haskal and collegues [12], with prompt optimal hepatic drainage as shown in final contrast-induced portography. According to clinical practice guidelines, long-term anticoagulation was initiated and a strict US-based follow-up was started, since the well-known considerable risk of stent thrombosis and dysfunction in Budd-Chiari syndrome [13,14].
Conclusion
In conclusion, this case shows that, even in presence of important technical issues, a transcaval TIPS placement, when performed in expert tertiary centers, is a feasible tool for a successful treatment of complex decompensated Budd-Chiari patients.
References
- Angeli P, et al. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018; 69; 406-460.
- Vizzutti F, et al. Transjugular intrahepatic portosystemic shunt (TIPS): Current indications and strategies to improve the outcomes. Intern. Emerg. Med. 2020; 15: 37-48.
- Rössle M. Interventional Treatment of Budd-Chiari Syndrome. Diagnostics. 2023; 13.
- Gasparini D, et al. Transjugular intrahepatic portosystemic shunt by direct transcaval approach in patients with acute and hyperacute Budd-Chiari syndrome. Eur. J. Gastroenterol. Hepatol. 2002; 14: 567-571.
- Artru F, Moschouri E, Denys A. Direct intrahepatic portocaval shunt (DIPS) or transjugular transcaval intrahepatic portosystemic shunt (TTIPS) to treat complications of portal hypertension: Indications, technique, and outcomes beyond Budd-Chiari syndrome. Clin. Res. Hepatol. Gastroenterol. 2022; 46: 101858.
- Petersen BD, Clark TWI. Direct Intrahepatic Portocaval Shunt. Tech. Vasc. Interv. Radiol. 2008; 11: 230-234.
- Fujiwara K, Kondo T, Fujimoto K, Koizumi J, Kato N. Percutaneous Transhepatic Direct Portosystemic Shunt for a Patient With Budd-Chiari Syndrome Using a Balloon as a Target in a Stenotic Inferior Vena Cava. Cureus. 2023; 15.
- Malakar S, et al. Budd Chiari Syndrome with Portal Vein Thrombosis Managed Successfully with Direct Intrahepatic Portosystemic Shunt: A Case Report and Review of the Literature. J. Clin. Exp. Hepatol. 2023; 13: 917-920.
- Lee KH, et al. Transcaval Transjugular Intrahepatic Portosystemic Shunt: Preliminary Clinical Results. Korean J. Radiol. 2003; 4: 35-41.
- Boyvat F, Aytekin C, Harman A, Özin Y. Transjugular intrahepatic portosystemic shunt creation in Budd-Chiari syndrome: Percutaneous ultrasound-guided direct simultaneous puncture of the portal vein and vena cava. Cardiovasc. Intervent. Radiol. 2006; 29: 857-861.
- Ul Haq T, Munir K, Haider Z, Yaqoob J, Usman U. Transjugular intrahepatic cavoportal shunt for Budd-Chiari syndrome. Australas. Radiol. 2005; 49: 140-143.
- Haskal Z, Duszak R, Furth EE. Transjugular intrahepatic transcaval portosystemic shunt: The gun-sight approach. J. Vasc. Interv. Radiol. 1996; 7: 139-142.
- Klinger C, et al. Doppler ultrasound surveillance of TIPS-patency in the era of covered stents - retrospective analysis of a large single-center cohort. Z. Gastroenterol. 2018; 56: 1053-1062.
- Hemachandran N, et al. Long-Term Outcomes of Endovascular Interventions in More than 500 patients with Budd-Chiari Syndrome. J. Vasc. Interv. Radiol. 2021; 32: 61-69.e1.
