
Open Access, Volume 10
Very late amplatzer device thrombosis and stroke
Gülüzar Traş; Halil Coşkun; Emre Paçacı*; İbrahim Halil Kurt
Adana City Training and Research Hospital, Turkey.
Emre Paçacı
Adana City Training and Research Hospital, Turkey.
Tel: 973-972-2449 & 973-972-3129;
Email: emre.pcci@hotmail.com
Received : Dec 23, 2023,
Accepted : Jan 17, 2024
Published : Jan 19, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Paçacı E (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Traş G, Coşkun H, Paçacı E, Kurt IH. Very late amplatzer device thrombosis and stroke. Open J Clin Med Case Rep. 2024; 2189.
Introduction
In many large center randomized controlled studies, it has been shown that percutaneous closure is more effective in patients with Atrial Septal Defect (ASD) who have cryptogenic stroke, when percutaneous closure is compared with medical treatment [1-6]. However, thrombus formation in percutaneous closure devices is one of the known and rare late complications [7]. In this context, we present a case of recurrent stroke attack after late thrombus development in the ASD closure device in a patient receiving dual antithrombotic therapy in our clinic
Case Presentation
A 53 years old male patient diagnosed with known gastric adenocarcinoma and with no comorbidities was admitted to the emergency department of our center on 05/10/2021. Diffusion MRI, taken after he presented with the complaint of left side weakness, revealed diffusion restriction in the right MCA irrigation area consistent with acute infarction. After the patient was evaluated by the stroke team, he underwent percutaneous thrombectomy. During the post-procedure follow-up, vital signs were stable, left lower extremity muscle strength was 4/5, and other neurological system examinations were observed naturally. After Transthoracic Echocardiography (TTE) and Transesophageal Echocardiography (TOE) performed for stroke etiology, a 9 mm secundum type ASD was observed at the edge of the tunnel type PFO. The patient was evaluated by a team consisting of cardiovascular surgery, neurology and cardiology specialists. The council decided to perform percutaneous ASD closure. After the patient was discharged with dual antithrombotic treatment, on 08/11/2021, the 16 mm Amplatzer closure device was delivered to the left atrium through the catheter and the left atrial disc was opened. The right atrial disc of the device, which was placed on the interatrial septum under TOE and fluoroscopy control, was opened to include all rims, and then all necessary checks were made. It was observed that the current was cut off and the device was successfully left in the septum. The patient, who had no complications after the procedure and whose follow-up was normal, was discharged with recommendations for continuation of dual antiplatelet therapy.
The diffusion MRI was taken after the patient re-applied to the emergency department of our center on 18/10/2023 with the complaint of speech impairment and numbness in the left arm. Acute infarction areas with sharply limited diffusion restriction with a long axis of approximately 5.5 cm in size were observed in the cortico-subcortical area at the ventricular level in the right cerebral hemisphere, in the temporoparital lobe, in the right cerebral hemisphere. Medical treatment was arranged according to the recommendation of neurology. In the TEE performed on the patient, an appearance consistent with a pedunculated mobile thrombus measuring 30*14 mm was observed on the left atrial side of the occluder device. After the patient was evaluated by the cardiology-cardiovascular surgery council, a surgical decision was made. The patient was discharged in full recovery after surgical treatment by cardiovascular surgery.
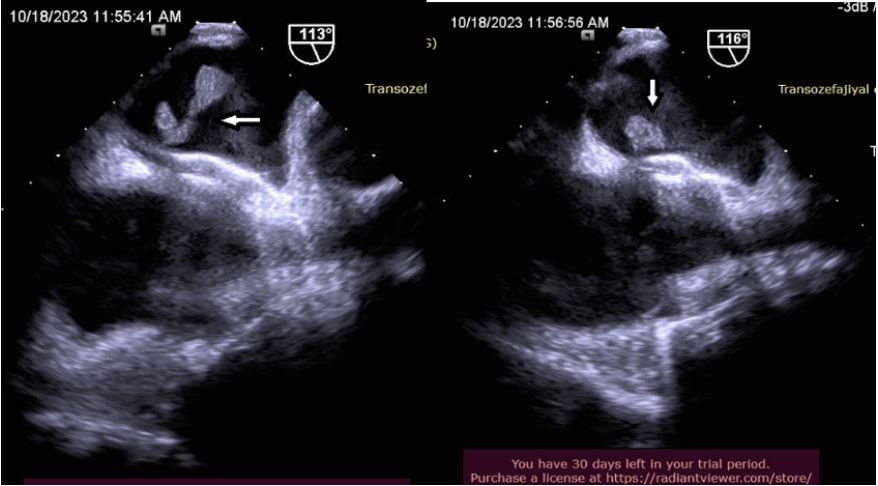
Figure 1
Discussion
Perioperative and short-term complications of ASD closure are frequently reported, but mortality and morbidity rates are relatively low. Late complications, especially those associated with the device, are rare but can be life-threatening, such as thrombosis and cardiac erosion. After device placement, late thrombosis can often cause ischemia in vital organs such as the lungs, brain and intestines. This condition is closely related to the patients hypercoagulable state and ineffective anticoagulation therapy. The Amplatzer device has a significantly lower incidence of thrombosis compared to other devices [8]. Unfortunately, there are no definitive guidelines for the management of cardiac thrombus in patients with acute cerebral infarction and pulmonary embolism. As an alternative to surgical treatment, there are also cases treated with fractionated/unfractionated heparin with close neurological monitoring. However, in our case, surgical treatment was applied considering the patients preference. Increasing evidence shows that the device can be fully endothelialized 6 months after implantation, but thrombosis may develop on the device due to certain predisposing factors such as infection and malignancy. In this patient, it must be ensured that the cerebral infarction is not caused by persistent atrial septal shunts. In our patient, TTE and TEE showed that there was no intra-device shunt, and a 30*14 mm thrombus was observed on the left atrial side of the device. It was suggested that the development of cerebral infarction in our patient after 2 years under dual antiplatelet therapy may be related to incomplete endothelialization of the device or may be due to hypercoagulability caused by oncology disease.
Conclusion
Atrial Septal Defect (ASD) and Patent Foramen Ovale (PFO) transcatheter closure has become an invasive alternative to open heart surgery. The first attempt at transcatheter ASD closure was described by King and Mills in 1974. Since then, a remarkable evolution has been observed in different devices with different materials, closing mechanisms and implantation methods. Although excellent results have been reported for transcatheter closure with different devices, concerns have been raised about peri- and/or post-interventional complications. The use of new generation ASD closure devices has made thrombus formation rare. The generally reported rate is between 1% and 2% [8]. The European Society of Cardiology recommends antiplatelet therapy for 6 months after device implantation and follow-up by a professional cardiology team for 2 years [9]. This case raises questions about the long-term safety of device-related complications and the importance of long-term clinical and echocardiographic evaluations. It is noteworthy that clinicians focus not only on standard anticoagulation therapy and routine ultrasound monitoring, but also on patient education and medication compliance.
References
- Furlan AJ, Reisman M, Massaro J, Mauri L, Adams H, et al. CLOSURE I Investigators. Closure or medical therapy for cryptogenic stroke with patent foramen ovale. N Engl J Med. 2012; 366: 991-999.
- Carroll JD, Saver JL, Thaler DE, Smalling RW, MacDonald LA, Marks DS, et al. Respect Investigators. Closure of patent foramen ovale versus medical therapy after cryptogenic stroke. N Engl J Med. 2013; 368: 1092-1100.
- Mas JL, Derumeaux G, Guillon B, Massardier E, Hosseini H, et al. Patent foramen ovale closure or anticoagulation vs. antiplatelets after stroke. N Engl J Med. 2017; 377: 1011-1021.
- Søndergaard L, Kasner SE, Rhodes JF, Andersen G, Iversen HK, et al. Gore REDUCE Clinical Study Investigators. Patent foramen ovale closure or antiplatelet therapy for cryptogenic stroke. N Engl J Med. 2017; 377: 1033-1042.
- Meier B, Kalesan B, Mattle HP, Khattab AA, Hildick-Smith D, et al. PC Trial Investigators. Percutaneous closure of patent foramen ovale in cryptogenic embolism. N Engl J Med. 2013; 368: 1083-1091.
- Lee PH, Song JK, Kim JS, Heo R, Lee S, et al. cryptogenic stroke and high-risk patent foramen ovale: the DEFENSE-PFO trial. J Am Coll Cardiol. 2018; 71: 2335-2342.
- Incidence and Clinical Course ofThrombus Formation on Atrial Septal Defect and Patient Foramen Ovale Closure Devices in 1,000 Consecutive Patients. 2004; 43(2): ISSN 0735-1097/04/$30.00 doi: 10.1016/j.jacc.2003.10.030
- Ulrike Krumsdorf, Stefan Ostermayer, Kai Billinger, Thomas Trepels, Elisabeth Zadan, et al. Incidence and clinical course of thrombus formation on atrial septal defect and patient foramen ovale closure devices in 1,000 consecutive patients. J Am Coll Cardiol. 2004; 43: 302-309.
- Baumgartner H, Bonhoeffer P, De Groot Nm, DE Haan F, Deanfield JE, Galie N, et al. Esc guidelines for the management of grown-up congenital heart disease (new version 2010). Eur Heart J. 2010; 31: 2915-57. 10.1093/eurheartj/ehq249.
