
Open Access, Volume 10
Disseminated Actinomyces meyeri infection: A case report and review of the literature
Abraham E Wei1*; Amanda Walker2; Ashkan Hashemi3; Debra Chew1
1Department of Medicine, Division of Infectious Diseases, New Jersey Medical School, 185 South Orange Avenue, MSB I-689, Newark, NJ 07101, USA
2Division of Internal Medicine and Pediatrics, Rutgers New Jersey Medical School, Newark, NJ 07101, USA.
3Division of Internal Medicine, Rutgers New Jersey Medical School, Newark, NJ 07101, USA.
Abraham E Wei
Department of Medicine, Division of Infectious Diseases, New Jersey Medical School, 85 South Orange
Avenue, MSB I-689, Newark, NJ 07101, USA.
Tel: 973-972-2449 & 973-972-3129;
Email: aewei37@gmail.com
Received : Dec 22, 2023,
Accepted : Jan 16, 2024
Published : Jan 19, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Actinomycosis is a chronic granulomatous infection rarely presenting as disseminated disease. We describe a case of disseminated Actinomyces meyeri infection involving the lung, brain, heart, and skin, and review cases of disseminated A. meyeri. To our knowledge, this is the first report of a disseminated A. meyeri case associated with endocarditis.
Keywords: Disseminated actinomycosis; Actinomyces meyeri.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Wei A (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Wei AE, Walker A, Hashemi A, Chew D. Disseminated Actinomyces meyeri infection: A Case report and review of the literature. Open J Clin Med Case Rep. 2024; 2188.
Introduction
Actinomycosis is an indolent infection caused by Actinomyces, a gram-positive anaerobic bacteria. It is characterized by infection crossing tissue planes, and mass-like features mimicking malignancy. Actinomycosis most often presents as oral-cervical facial disease and can sometimes involve the abdominal-pelvic and thoracic areas. It rarely causes disseminated disease [1].We report a rare presentation of disseminated A. meyeri with skin, lung, brain, and heart involvement.
Case Presentation
A 36-year-old man with no past medical history was admitted with multiple skin abscesses of his extremities and chest wall for 4 months. He endorsed having 40-pound weight loss, fatigue, and night sweats for the past few months, and developed headaches and left eye blurry vision for the past 2 weeks. Outside hospital records showed multiple emergency department visits over the past 3 months, where he was diagnosed and treated for pneumonia, followed by short courses of antibiotics for his skin abscesses. On admission, he was afebrile. He had multiple subcutaneous abscesses on his extremities, with an 8 cm fluctuant mass overlying his sternum (Figure 1). He had heavy dental plaques on oral exam. His social history was significant for being a 20 pack-year cigarette smoker, worked in a warehouse as a package handler, he was born and had lived in New Jersey all his life, and denied any recent travel.
Computed Tomography (CT) of the chest showed a consolidation within the lingula with extension into the anterior chest wall, and a 2 x 5.7 cm soft tissue chest wall fluid collection (Figure 2). Magnetic Resonance Imaging (MRI) brain showed innumerable enhancing intraparenchymal and leptomeningeal/ependymal lesions and enhancement within the right mastoid and below the skull base (Figure 3A). On second night of hospitalization, he developed a fever of 102.3o F. After chest wall abscess was aspirated, he was started on isoniazid, rifampin, pyrazinamide, ethambutol, azithromycin, linezolid, cefoxitin, amikacin and dexamethasone for suspicion of possible mycobacterium infection. Chest wall lesion was also biopsied, and preliminary pathology review showed foamy histiocytes and no granulomas. Transthoracic and transesophageal echocardiogram revealed a small mitral valve vegetation. Culture from chest wall aspirate grew a Gram-positive rod anaerobe after 6 days of incubation, subsequently identified as Actinomyces meyeri by Matrix-Assisted Laser Desorption/Ionization-Time of Flight (MALDI-TOF) mass spectrometry. Fusobacterium necrophorum (beta-lactamase negativefi) also grew on culture and later identified. 16S ribosomal RNA testing showed minor abundance of Aggregatibacter actinomycetemcomitans, Fusobacterium nucleatum, Ralstonia pickettii, Methylbacterium radiotolerans, Caulobacter spp, Novosphingobium spp, and Pseudomonas japonica. Final pathology review of chest wall lesion showed acute and chronic inflammation with prominent histiocytic infiltrates. Gram, acid-fast bacillus, Fite, Giemsa, and periodic acid-Schiff stains did not reveal any microorganisms.

Figure 1: CT chest showing right lung pneumothorax, hemothorax, and subcutaneous emphysema.
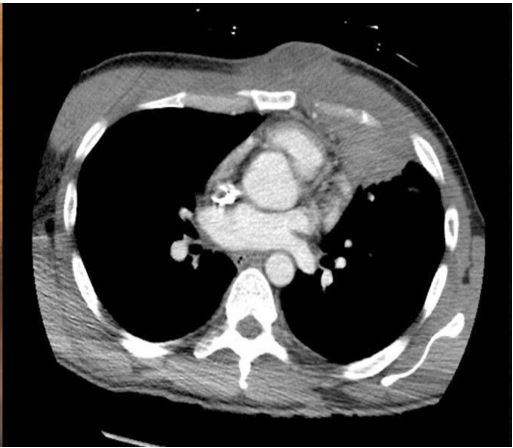
Figure 2: Pathological examination with hematoxylin and eosin stain showing spindle-shaped cells in whorls and bundles
supporting the diagnosis of pulmonary meningioma at 10X (Figure 2) and 20X (Figure 3).
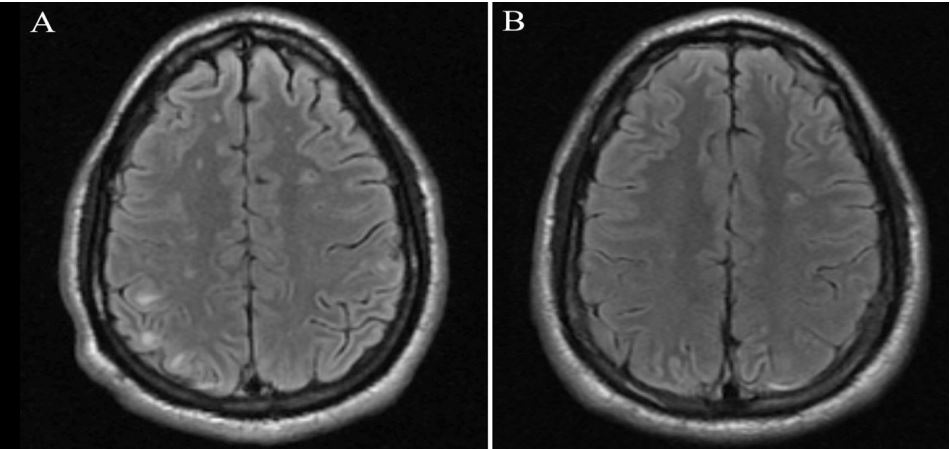
Figure 3: Immunohistochemical examination showing
tumor cells stained positive for vimentin.
Table 1: Summary of disseminated actinomycosis cases reported in literature.
| Ref | Case no. |
Sex | Age | Clinical manifestations |
Comorbidities and risk factors |
Treatment |
Antibiotic duration (months) |
Outcome | Copathogens |
|---|---|---|---|---|---|---|---|---|---|
| [5] | 1 | F | 72 | Empyema, pelvic mass | RA, IUD, S | Amoxicillin | 6 | N/A | None |
| [6] | 2 | M | 46 | Lung mass, brain abscess | S, A | Amoxicillin | 12 |
Improved at 5-months
after starting antibiotic therapy |
Propionibacterium acnes, Fusobacterium nucleatum |
| [7] | 3 | M | 50 | Lung mass, brain abscesses | A, PO |
Penicillin (4 months) →
amoxicillin (16 months), surgical drainage |
20 | Resolved | Petostreptococcus spp, Fusobacterium spp |
| [8] | 4 | M | 43 | Thoracic mass, peritonitis | A, S | Penicillin, thoracotomy | 6 | Resolved | None |
| [9] | 5 | M | 34 |
Pneumonia, thigh abscess, paravertebral mass |
PO | Amoxicillin, abscess drainage | 12 | Resolved | Fusobacterium nucleatum |
| [3] | 6 | M | 47 |
Lung mass, skin
abscesses, osteomyelitis of tibia |
A, S, PO | Penicillin, surgical debridement | 12 | Resolved | Actinobacillus actinomycetemcomitans |
| [10] | 7 | M | 44 |
Pneumonia, skin
abscesses, brain abscesses |
A, S | Amoxicillin, neurosurgical aspiration | 12 | Resolved | Actinobacillus actinomycetemcomitans |
| [11] | 8 | M | 62 |
Pneumonia and empyema, hip skin abscess |
A, PO |
Penicillin, chest tube
drainage, surgical drainage |
12 | N/A |
Fusobacterium nucleatum,
Bacteroides ureolyticus, Streptococcus constellatus, Peptococcus spp, Propionibacterium spp |
| [12] | 9 | M | 35 |
Pneumonia, liver abscess, mesenteric abscesses |
PO | Penicillin | 12 | Resolved | Actinobacillus actinomycetemcomitans |
| [13] | 10 | M | 16 |
Empyema, bone marrow infection |
Tuba player* |
Clindamycin, chest tube
drainage, thoracotomy |
6 | Resolved | None |
| [14] | 11 | M | 58 |
Pleuropulmonary
infection, pyomositis of calf |
Chronic bronchitis, A, S |
Penicillin, surgical drainage | 6 | Resolved | None |
| [15] | 12 | M | 49 |
Osteomyelitis of tibia
and fibula, skin abscesses |
PO | Penicillin | 4 |
Improved at 3-months
after starting antibiotic therapy |
None |
| [15] | 13 | M | 34 |
Vertebral abscesses, skin abscesses, suspected pericarditis |
PO | Penicillin, surgical drainage | 4 | Resolved | None |
| [16] | 14 | M | 46 | Pneumonia, skin abscess | A, S | Penicillin, surgical debridement | 4 | Resolved | Capnocytophaga spp |
| [17] | 15 | M | 40 |
Pneumonia, osteomyelitis
of tibia, skin abscess |
A, S, PO | Penicillin | 3 | Resolved | None |
| [18] | 16 | M | 49 | Skin abscesses, tibial lesion | PO | Penicillin | 4 | N/A | None |
| [PC] | 17 | M | 36 |
Pneumonia and lung mass, skin abscesses, brain abscesses, endocarditis |
S, PO |
Ceftriaxone (1.5 months)
→ Amoxicillin, percutaneous drainage |
12 |
Improved at 2 months
after starting antibiotic therapy |
Fusobacterium necrophorum,
Fusobacterium nucleatum, Aggregatibacter actinomycetemcomitans, Ralstonia pickettii, Methylbacterium radiotolerans, Caulobacter spp, Novosphingobium spp, Pseudomonas japonica |
A: alcohol abuse; IUD: intrauterine device; N/A: not applicable; PC: present case; PO: periodontal disease; RA: rheumatoid arthritis; S: current smoker; *possible aspiration risk as a tuba player.
His antimicrobials were changed to high dose intravenous ceftriaxone (2 gm every 12 hours). Metronidazole was added but discontinued after 8 days due to pruritis and lack of beta-lactamase positive anaerobes identified on cultures. Positron Emission Tomography (PET) scan confirmed disseminated disease with fluorodeoxyglucose avid foci in the left temporal lobe of brain, multiple subcutaneous nodules in the neck, chest, abdomen, pelvis and both upper and lower extremities, and airspace consolidation in the anterior left upper lung lobe extending to the adjacent mediastinum and left anterior chest wall. After 6 weeks, his chest wall abscess had significantly improved with resolved lesions on MRI brain (Figure 3B), and he was switched to high dose oral amoxicillin with plan to complete a 12 month treatment course.
Discussion
Actinomyces is a branched, filamentous, Gram-positive bacteria usually causing slowly progressive oral-cervical, thoracic, abdominal, or pelvic disease. Disseminated Actinomyces infection is rare, occurring when hematogenous seeding of infection results in multi-organ involvement. We highlighted a rare case of disseminated A. meyeri infection involving the lung, brain, heart, and skin. To our knowledge, only 16 disseminated A. meyeri cases have previously been reported (Table 1). Only 2 reported A. meyeri infective endocarditis cases without disseminated disease have previously been reported [2,3].
Disseminated infection is most often associated with Actinomyces meyeri [1,4], as in our case. The mechanism that predisposes A. meyeri for disseminated disease is unclear, but it has a predilection for lung disease, which is often the source of hematogenous seeding [4]. Poor oral hygiene (as in our case) and alcoholism have been risk factors associated with A. meyeri infection, and predispose to aspiration of Actinomyces species from the oropharynx to the lungs [1]. Infection occurs when there is a disruption of mucosal surface with subsequent bacterial invasion of the tissue.
Review of previously reported disseminated A. meyeri cases are summarized in Table 1. Similar to our case, they highlight clinical characteristics that are hallmarks of actinomycosis infection. These include an indolent, chronic course, development of abscesses with dense fibrosis, and progression of infection through normal fascial and tissue boundaries, with mass-like features that mimic malignancy. The vast majority of these cases involved the lungs.
Our case appears to be the first reported A. meyeri disseminated infection-involving endocarditis. By clinical history, we hypothesize that the lungs was the likely source of hematogenous dissemination in our case, however, endocarditis could also have contributed to septic emboli to the brain. It is possible that endocarditis in disseminated Actinomyces infection is unrecognized due to lack of associated positive blood cultures in disseminated cases and lack of performing echocardiography (Table 1). Actinomyces and common copathogens are classically associated with culture-negative endocarditis. Positive blood cultures have been rare in association with disseminated infection [3]. It is possible contiguous invasion of tissues and erosion into blood vessel walls may lend to hematogenous dissemination, similar to that described in nocardiosis infection [19]. The central nervous system (CNS) is infrequently involved in disseminated A. meyeri infection [4]. Similar to our case, CNS actinomycosis most commonly presents as brain abscess.
Diagnosis of actinomycosis requires a high index of clinical suspicion and is based on the presence of sulfur granules (dense aggregates of bacteria and neutrophilic infiltrate) on histopathology, visualization of Gram-positive branching filamentous organisms on Gram stain (a few Actinomyces species including A. meyeri are non-branching) and microbiologic isolation on cultures. Failure rate for culture isolation is high (>50%), and optimal microbiologic yield requires avoidance of antibiotics prior to specimen collection, appropriate timely collection of specimens, and alerting microbiology lab to hold specimens for prolonged anaerobic incubation (usually 5-21 days). Usually, Actinomyces species is isolated with common copathogens, such as Aggregatibacter actinomycetemcomitans, Eikenella corrodens, Fusobacterium, Bacteroides, Capnocytophaga, Staphylococcus, Streptococcus, and Enterobacteriaceae. Rapid diagnostic testing, such as MALDI-TOF and molecular studies with 16S ribosomal RNA sequencing, as used in our case, have led to more rapid and accurate identification of Actinomyces infection [1].
Standard treatment for extensive disease usually entails prolonged and high-dose antibiotic therapy for favorable outcomes. Average duration of treatment for disseminated cases was 8 months (range 4-12 months), often with intravenous penicillin G followed by oral amoxicillin. Actinomyces is generally susceptible to most antibiotics with the exception of metronidazole, quinolones, and clindamycin [20]. For CNS disease and endocarditis, intravenous ceftriaxone is desirable given penetration into tissues at these critical sites, and for greater dosing convenience. Some experts also recommend a short course of treatment for copathogens. CT/MRI studies and PET scans are useful in monitoring for disease resolution. Surgery is usually reserved for critical sites of infection and refractory disease and drainage of abscesses [1].
Conclusion
Although a rare event, clinicians should be aware that Actinomyces infection, particularly A. meyeri, has the potential to cause disseminated disease. Actinomycosis should be considered in indolent granulomatous diseases characterized by chronic abscesses, sinus tracts, and disease progression through normal tissue planes, prompting appropriate diagnostic testing. Therapy requires prolonged high-dose antibiotic therapy, often with penicillin G or beta-lactam antibiotics.
Acknowledgement
We would like to thank the Rutgers New Jersey Medical School microbiology laboratory for their expertise and assistance in our case.
References
- Russo TA. Agents of Actinomycosis. Bennett JE, Dolin R, Blaser MJ, editors. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 9th ed, Elsevier Saunders, Philadelphia. 2020; 3071-3081.
- Huang KL, Beutler SM, Wang C. Endocarditis due to Actinomyces meyeri. Clin Infect Dis. 1998; 27(4): 909-910.
- Moffatt S, Ahmen AR, Forward K. First reported case of bacterial endocarditis attributable to Actinomyces meyeri. Can J Infect Dis. 1996; 7(1): 71-73.
- Apotheloz C, Regamey C. Disseminated infection due to Actinomyces meyeri: case report and review. Clin Infect Dis. 1996; 22(4): 621-625.
- Cliffe A, Hassan W, Ward D, Elgara M. Actinomyces meyeri causing disseminated actinomycosis in the presence of concurrent bronchogenic carcinoma. BMJ Case Rep. 2022; 15(2): e247577.
- Park HJ, Park K, Kim S, Sung H, Choi S, et al. A Case of disseminated infection due to Actinomyces meyeri involving lung and brain. Infect Chemother 2014; 46(4): 269-273.
- Colmegna I, Rodriguez-Barradas M, Rauch R, Clarridge J, Young EJ. Disseminated Actinomyces meyeri infection resembling lung cancer with brain metastases. Am J Med Sci. 2003; 326(3): 152-155.
- Mook WN, Simonis FS, Schneeberger PM, van Opstal JL. A rare case of disseminated actinomycosis caused by Actinomyces meyeri. Neth J Med. 1997; 51(1): 39-45.
- Liaudet L, Erard P, Kaeser P. Cutaneous and muscular abscesses secondary to Actinomyces meyeri pneumonia. Clin Infect Dis. 1996; 22(1): 185-186.
- Kuijper EJ, Wiggerts HO, Jonker GJ, Schaal KP, de Gans J. Disseminated actinomycosis due to Actinomyces meyeri and Actinobacillus actinomycetemcomitans. Scand J Infect Dis. 1992; 24(5): 667-672.
- Rose HD, Varkey B, Kutty CP. Thoracic actinomycosis caused by Actinomyces meyeri. Am Rev Respir Dis 1982; 125(2): 251-254.
- Marty HU, Wust J. Disseminated actinomycosis caused by Actinomyces meyeri. Infection. 1989; 17(3): 154-155.
- Lentino JR, Allen JE, Stachowski M. Hematogenous dissemination of thoracic actinomycosis due to Actinomyces meyeri. Pediatr Infect Dis. 1985; 4(6): 698-699.
- Alemanni A, Manigand G, Taillandier J. Pyomyosite a Actinomyces meyeri avec atteinte pulmonaire associee. Revue de la litterature. A propos d’une observation. Sem Hop Paris. 1988; 64: 2799-2803.
- Bussiere JL, Ristori JM, Beytout J, Janin-Mercier A, Martorell J, et al. Infections osseuses et articulaires a Actinomyces meyeri localisations cervico-fasciales exclues. A propos de 3 cas. Rev Rhum Mal Osteoartic. 1986; 53: 677-680.
- Machet L, Machet MC, Esteve E, Delarbre JM, Pelucio-Lopes C, et al. Actinomyces meyeri cutaneous actinomycosis with pulmonary localization. Ann Dermatol Venereol. 1993; 120(12): 896-899.
- Ferrier MC, Janin-Mercier A, Meyer A, Beytout J, Cambon M, et al. Actinomyces meyeri actinomycosis: A case with thoracic and tibial localization. Ann Med Interne (Paris) 1986; 137(8): 649-651.
- Ferrier MC, Ristori JM, Beytout J, Cambon M, Roger H, et al. Disseminated actinomycosis caused by Actinomyces meyeri. 3 cases with multiple cutaneous localizations. Ann Dermatol Venereol. 1991; 118(11): 843-845.
- Pujic P, Beaman BL, Ravalison M, Boiron P, Rodriguez-Nava V. Nocardia and Actinomyces: Diseases caused by Actinomyces. Tang Y, Sussman M, Liu D, Poxton I, Schwartzman J, editors. In: Molecular Medical Microbiology. Amsterdam: Academic Press. 2015; 731-752.
- Steininger C, Willinger B. Resistance patterns in clinical isolates of pathogenic Actinomyces species. J Antimicrob Chemother. 2016; 71(2): 422-427.
