
Open Access, Volume 10
From trauma to tumor: Primary pulmonary meningioma revealed
Rajvi Gor1*; Arlene Yu2; Yutika Dongre1; Shaunak Mangeshkar1; Praneeth Reddy Keesari3; Abhishek Kumar2
1Department of Internal Medicine, Jacobi Medical Center/Albert Einstein College of Medicine, USA.
2Department of Hematology & Oncology, Jacobi Medical Center/Albert Einstein College of Medicine, USA.
3Department of Internal Medicine, Staten Island University Hospital, USA.
Rajvi Gor
Department of Internal Medicine, Jacobi Medical Center/Albert Einstein College of Medicine, USA.
Email: rajviskansagara@gmail.com
Received : Dec 22, 2023,
Accepted : Jan 15, 2024
Published : Jan 19, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Primary pulmonary meningiomas (PPMs) are a rare type of meningioma that arises primarily in the lungs, outside the dura mater of the central nervous system. The majority of PPMs are benign and present as asymptomatic solitary pulmonary nodules incidentally diagnosed on imaging. A 32-year-old male presented to the hospital after a motor vehicle accident resulting in multiple injuries, including right apical pneumothorax, and underwent right upper lobe wedge resection. Surgical pathology of the VATS specimen revealed a 2 mm irregular nodule with morphologic and immunohistochemical features favoring a meningothelial nodule. CT of the head and the entire spine did not show any primary brain or spinal meningioma, and a diagnosis of PPM was made. Unlike most cases that are diagnosed incidentally on imaging, the PPM in our case was first noted only on the pathology specimen and found to be excised entirely on the biopsy specimen. When an isolated pulmonary nodule is seen incidentally on imaging or lung biopsy, primary pulmonary meningioma (PPM) should be considered as a differential. CNS imaging with CT or MRI is needed to confirm an isolated extracranial presence of PPM as opposed to a metastatic primary CNS meningioma. Only pathology can differentiate between a benign vs malignant PPM.
Keywords: Meningioma; Primary pulmonary meningioma; Lung nodule; Meningothelial nodule; Ectopic meningioma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Gor R (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Gor R, Yu A, Dongre Y, Mangeshkar S, Keesari PR, Kumar A. From trauma to tumor: Primary pulmonary meningioma revealed. Open J Clin Med Case Rep. 2024; 2187.
Introduction
Meningiomas are the most common type of primary brain tumor [1]. However, primary ectopic meningiomas, defined as meningiomas arising outside of the dura, are uncommon, with incidence ranging from 0.9% to 2% of all meningiomas [2]. Among them, primary pulmonary meningiomas are sporadic, with the majority presenting as an asymptomatic solitary pulmonary nodule, usually incidentally diagnosed on imaging. We report a rare case of primary pulmonary meningioma (PPM) diagnosed incidentally on videoassisted thoracic surgery (VATS) lung specimen biopsy in a trauma patient, which was not visualized in imaging studies.
Case Presentation
We present a case of a 32-year-old male who presented to the hospital after a motor vehicle accident resulting in multiple facial bone fractures, displaced right third and fourth lateral rib fractures, right lung contusion, right apical pneumothorax, and hemothorax (Figure 1). The patient underwent multiple surgeries, which included right 4th rib open reduction and internal fixation (ORIF), VATS with right upper lobe wedge resection, mechanical pleurodesis, and chest tube placement. Surgical pathology of the VATS specimen revealed a 2 mm irregular nodule with morphologic and immunohistochemical features favoring a meningothelial nodule (Figures 2 and 3). The immunohistochemical stain was positive for vimentin (Figure 4) and epithelial membrane antigen (EMA) and negative for CD56, progesterone receptor, and cytokeratin. A diagnosis of benign pulmonary meningioma was made. The lesion appeared to be excised entirely on the biopsy specimen. Interestingly, this lung nodule was not visualized on any prior chest X-ray or computed tomography (CT) of the chest and was first noted only on the pathology specimen. CT of the head (Figure 5) and the entire spine did not show any primary brain or spinal meningioma, enabling the diagnosis of primary pulmonary meningioma.
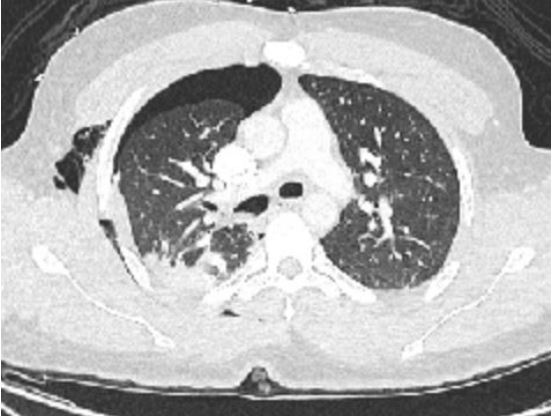
Figure 1: CT chest showing right lung pneumothorax, hemothorax, and subcutaneous emphysema.
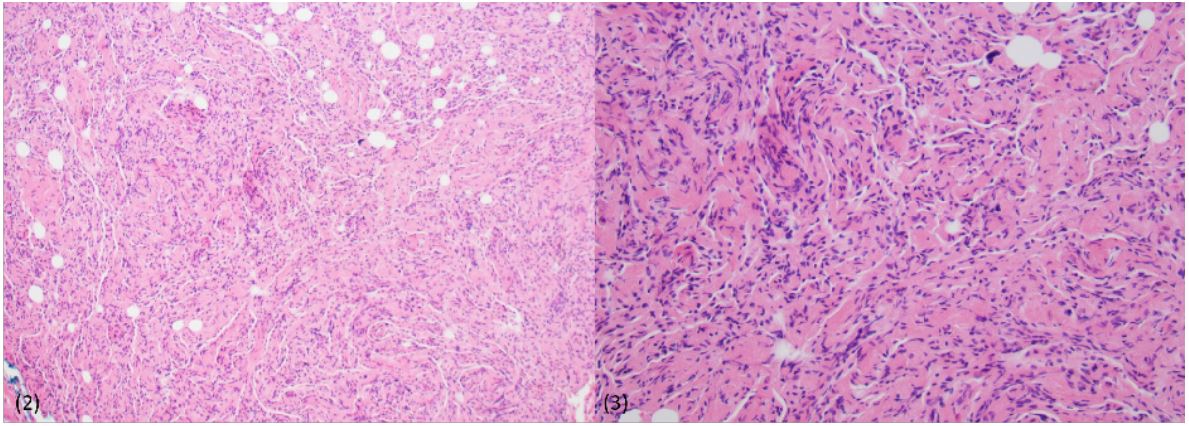
Figure 2 & 3: Pathological examination with hematoxylin and eosin stain showing spindle-shaped cells in whorls and bundles
supporting the diagnosis of pulmonary meningioma at 10X (Figure 2) and 20X (Figure 3).
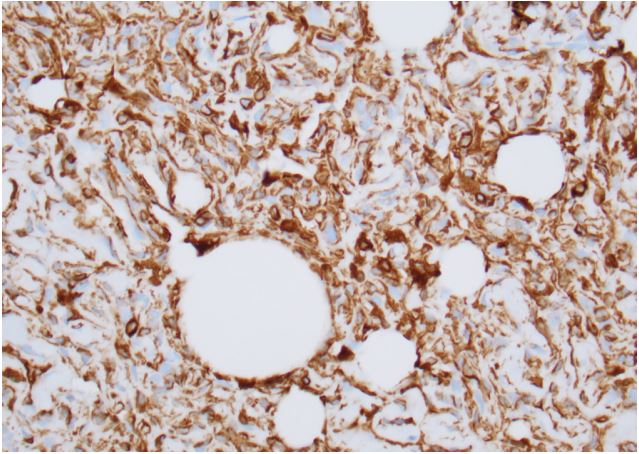
Figure 4: Immunohistochemical examination showing
tumor cells stained positive for vimentin.
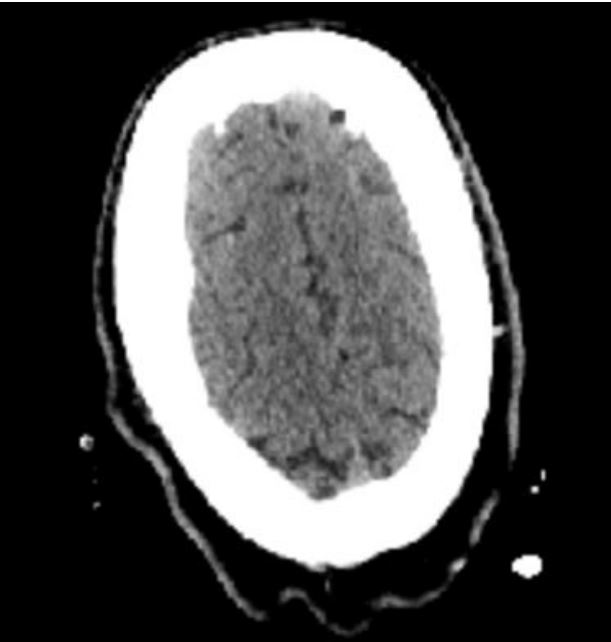
Figure 5: CT head without evidence of dural lesion/meningioma in the brain, confirming that the pulmonary
meningioma is ectopic and arising primarily in the lungs.
Discussion
Primary pulmonary meningioma is a rare tumor entity, with the first case being reported by Kemnitz et al. in 1982 [3]. Since then, 67 cases of PPMs have been reported between 1982 and 2021, of which five were identified as malignant meningiomas [4]. These tumors may affect all age groups ranging from 18 to 108 years [5], with slightly higher occurrence in females [6]. Several hypotheses have been proposed to explain the origin of primary pulmonary meningiomas. Per one hypothesis, PPMs can arise from the proliferation of arachnoid cells that were misplaced during embryogenesis [7]. Another plausible explanation involves their origin from pluripotent sub-pleural mesenchymal cells or minute pulmonary meningothelial-like nodules (MPMNs) [6]. MPMNs stain positive for vimentin, epithelial membrane antigen (EMA), progesterone, and CD56, similar to PPMs [8,9]. In our case, immunohistochemistry was positive for vimentin and EMA, although negative for progesterone receptors.
Most PPMs present as asymptomatic nodules, incidentally found on imaging. However, some may present with pulmonary symptoms such as hemoptysis [10], cough, shortness of breath, or non-specific symptoms. PPMs commonly appear as single, spherical, well-defined nodules on chest CT, with sizes varying from 0.6 cm to 6 cm [11,12]. Sometimes, unusual features such as lobulations, calcifications, or ground-glass opacities can be seen [4]. The contrast enhancement pattern also varies, with several PPMs showing uniform enhancement [13]. Most PPMs show high uptake on standard F18-fluorodeoxyglucose (18F-FDG) computed tomography–positron emission tomography (CT–PET); however, low uptake has also been noted [14]. Hence, due to vast variability, CT contrast or FDG uptake may not help differentiate malignant vs. benign PPM. Unlike the vast majority of these cases, no lesion was seen on the CT scan in our case, which could be attributed to the small size of 2 mm or a difficult-to-visualize nodule location.
PPMs typically appear as spindle- or ovoid-shaped cells grouped in lobules or a whorl arrangement on histological exam [15]. Features more likely seen in malignant meningiomas include increased nuclear atypia, mitoses, necrosis, and increased Ki-67 proliferation index [14]. As in our case, most tumors stain positive for vimentin and EMA. Unlike our case, positive staining for CD56 and progesterone has also been noted in some PPM cases, which could mean similar precursor cells as MPMNs [8]. Cytokeratin, desmin, and CD34 are usually negative.
When a meningioma is discovered in the lungs, it is crucial to differentiate between metastatic primary CNS meningioma and primary ectopic meningioma. Most primary CNS meningiomas do not metastasize. However, more than 60% go to the lungs when they do metastasize [16]. Some risk factors for distant metastasis of CNS meningioma include recurrence of primary tumor, venous sinus invasion, non-skull base location, and high grade on histology [17]. Per WHO 2021 grading system, CNS meningiomas can be graded as Grade I (benign), Grade II (atypical), and Grade III (malignant or anaplastic), with higher grades (II and III) associated with risk of metastasis [18,19]. In a retrospective analysis of eight primary ectopic and five metastatic meningiomas, metastatic lesions were more associated with nuclear atypia, necrosis, and mitoses [20]. Both PPM and metastatic meningioma to the lungs can have similar microscopic findings; hence, a histologic diagnosis of pulmonary meningioma, as in our case, is inadequate to differentiate between the two entities [15,21]. Hence, CNS imaging to rule out intracranial or spinal tumors is crucial for this distinction, with MRI being preferred over CT scan [9,21,22]. Our patient underwent a CT head, which did not show evidence of CNS meningioma, hence confirming the diagnosis of PPM.
Primary ectopic meningiomas can be benign PPM or malignant PPM. Features more likely seen in malignant meningiomas include increased nuclear atypia, mitoses, necrosis, and increased Ki-67 proliferation index [4]. The mainstay of treatment for PPMs is surgical resection, with lobectomy for central lesions and wedge resection preferred for minor peripheral nodules [6]. Overall prognosis is good, without recurrence or metastasis, especially in benign lesions [6]. However, recurrence has been noted in malignant PPMs [5,23]. In our case, PPM was diagnosed incidentally after the VATS lung resection specimen was histologically examined and appeared to be excised entirely on pathology. There are no formal guidelines for the management and surveillance of PPM, as it is rare. As per the tumor board discussion, repeat CT chest imaging in one year is planned for our patient to assess for recurrence. Given the dearth of clinical data available, summarizing any and all clinical presentations and management of this unique diagnosis will pave the way for better recognition of this sporadic tumor
Acknowledgements: We thank Dr. Maria Abadi, Department of Pathology at Jacobi Medical Center/AECOM for assistance in obtaining pathology slides.
References
- Lamszus K. Meningioma pathology, genetics, and biology. J Neuropathol Exp Neurol. 2004; 63: 275-86.
- Kershisnik M, Callender DL, Batsakis JG. Pathology consultation, extracranial, extraspinal meningiomas of the head and neck. Ann Otol Laryngol. 1993; 102: 967-70.
- Kemnitz P, Spormann H, Heinrich P. Meningioma of lung: first report with light and electron microscopic findings. Ultrastruct Pathol. 1982; 3: 359-365.
- Zhang DB, Chen T. Primary pulmonary meningioma: A case report and review of the literature. World J Clin Cases. 2022; 10(13): 4196-4206.
- Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. 4. Lyon: World Health Organization. 2015.
- Incarbone M, Ceresoli GL, Di Tommaso L, Cappuzzo F, Inzirillo F, Infante M, et al. Primary pulmonary meningioma: report of a case and review of the literature. Lung Cancer. 2008; 62(3): 401-7.
- Batsakis JG. Pathology consultation. Extracranial meningiomas. Ann Otol Rhinol Laryngol. 1984; 93(3-1): 282-3.
- Masago K, Hosada W, Sasaki E, Murakami Y, Sugano M, Nagasaka T, et al. Is primary pulmonary meningioma a giant form of a meningothelial-like nodule? A case report and review of the literature. Case Rep Oncol. 2012; 5(2): 471-8.
- Juan CM, Chen ML, Ho SY, Huang YC. Primary Pulmonary Meningioma Simulating a Pulmonary Metastasis. Case Rep Pulmonol. 2016; 2016: 8248749.
- Izumi N, Nishiyama N, Iwata T, Nagano K, Tsukioka T, et al. Primary pulmonary meningioma presenting with hemoptysis on exertion. Ann Thorac Surg. 2009; 88(2): 647-8.
- Han D, Deng H, Liu Y. Primary pulmonary meningiomas: report of two cases and review of the literature. Pathol Res Pract. 2020; 216: 153232.
- Lin D, Yu Y, Wang H, Fang Y, Yin J, Shen Y, et al. Radiological manifestations, histological features and surgical outcomes of pulmonary meningothelial proliferation: a case series and rethinking. Transl Lung Cancer Res. 2020; 9: 1159-68.
- Kim YY, Hong YK, Kie JH, Ryu SJ. Primary pulmonary meningioma: an unusual cause of a nodule with strong and homogeneous enhancement. Clin Imaging. 2016; 40(1): 170-3.
- Gürçay N, Öztürk A, Demirağ F, İncekara F. Primary pulmonary meningioma mimicking pulmonary metastasis: A rare case report. Turk Gogus Kalp Damar Cerrahisi Derg. 2020; 28(4): 699-701.
- Cesario A, Galetta D, Margaritora S, Granone P. Unsuspected primary pulmonary meningioma. Eur J Cardiothorac Surg. 2002; 21(3): 553-5.
- Yekeler E, Dursun M, Yilmazbayhan D, Tunaci A. Multiple pulmonary metastases from intracranial meningioma: MR imaging findings (case report). Diagn Interv Radiol. 2005; 11(1): 28-30.
- Eric Y. Montgomery, Chandrasekhar Sundarrajan, Mark N. Pernik, James P. Caruso, Tomas Garzon-Muvdi. Metastatic Meningioma: A Systematic Review of Incidence and Risk Factors, Interdisciplinary Neurosurgery. 2023; 101720: 2214-7519.
- Ogasawara C, Philbrick BD, Adamson DC. Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future Directions. Biomedicines. 2021; 9(3): 319.
- Dalle Ore CL, Magill ST, Yen AJ, Shahin MN, Lee DS, Lucas CG, et al. Meningioma metastases: incidence and proposed screening paradigm. J Neurosurg. 2019; 132(5): 1447-1455.
- Ocque R, Khalbuss WE, Monaco SE, Michelow PM, Pantanowitz L. Cytopathology of extracranial ectopic and metastatic meningiomas. Acta Cytol. 2014; 58(1): 1-8.
- Chiarelli M, Simone MD, Gerosa M, Guttadauro A, U. Cioffi. An incidental pulmonary meningioma revealing an intracranial meningioma: primary or secondary lesion? Annals of Thoracic Surgery, 2015; 99(4): 83-84.
- Whittle IR, Smith C, Navoo P, Collie D. Meningiomas. Lancet. 2004; 363(9420): 1535-43.
- Gomez-Aracil V, Mayayo E, Alvira R, Arraiza A, Ramón y Cajal S. Fine needle aspiration cytology of primary pulmonary meningioma associated with minute meningotheliallike nodules. Report of a case with histologic, immunohistochemical and ultrastructural studies. Acta Cytol. 2002; 46(5): 899-903.
