
Open Access, Volume 10
Catheter-directed therapies for high and intermediate-high risk patients with acute pulmonary embolism: Results from a multiparametric follow-up protocol
André Grazina*; Bárbara Lacerda Teixeira*; Luís Almeida Morais; António Fiarresga; Ruben Ramos; Tiago Pereira da Silva; Francisco Barbas Albuquerque; João Reis; Ana Galrinho; Ana Santana; Duarte Cacela; Rui Cruz Ferreira
Cardiology Department, Hospital de Santa Marta, Lisbon, Portugal.
André Grazina & Bárbara Lacerda Teixeira
Cardiology Department, Hospital de Santa Marta, Lisbon, Portugal.
Tel: +351-964792602;
Email: grazina.andre@gmail.com
Received : Dec 18, 2023,
Accepted : Jan 11, 2024
Published : Jan 19, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Intermediate-high- and high-risk pulmonary embolism (PE) patients treated with anticoagulation alone are associated with a considerable risk of circulatory collapse, death, or long-term pulmonary hypertension. Pulmonary Embolism Response Teams (PERT) have been created to deliver PE patients a better care. Catheter-Directed Therapies (CDT), with mechanical thrombolysis and/or local fibrinolysis allow faster reperfusion and hemodynamic improvement without the systemic bleeding risk of systemic fibrinolysis. However, clinical evidence of its safety and benefits are lacking.
Objectives: This analysis aims to describe the hemodynamics, morphological and perfusion improvement over time in intermediate-high- and high-risk acute PE patients submitted to CDT.
Methods: Prospective registry of consecutive intermediate-high- and high-risk PE patients submitted to CDT (mechanical thrombolysis with Penumbra aspiration system and/or intrapulmonary local fibrinolysis with alteplase) in a single tertiary center. A multiparametric follow-up protocol was designed to evaluate echocardiographic, CT-scan, pulmonary angiogram, and right heart catheterization data at admission and at 3 months after CDT.
Results: 39 PE patients (46.2% male, mean age 60 years old) were submitted to CDT (18% combined Penumbra and local fibrinolysis, 10% isolated Penumbra and 72% isolated local fibrinolysis). No major bleeding was seen during or after the procedure. 1 pulmonary artery dissection and 1 Penumbra burr partial avulsion occurred, both treated conservatively. 4 patients died during the follow-up (1 with cardiogenic shock and 3 for non-cardiovascular). Of the remaining, 23 patients completed the 3-month follow-up protocol. At 3 months, a significant improvement was seen in the patients’ hemodynamics with 3.6mmHg, 16.8mmHg and 10.7mmHg mean drops in RA, systolic PA and mean PA pressures (p<0.001), 1.61L/min and 0.85L/min/m2 mean increases in cardiac output and index (p <0.001), and 1.65 Wood units decrease in the pulmonary vascular resistance (p 0.012). It was also seen an improvement in the perfusion defects with a mean drop of 8.7 points in the modified Miller index (p <0.001) and an improvement in the RV function with a mean decrease of 0.5 in the RV/LV ratio by CT-scan (p <0.001) and a mean increase of 5.4mm in TAPSE (p <0.001) and tricuspid annular s’ velocity by 5.0cm/s (p 0.006).
Conclusions: In patients with intermediate-high- and high-risk PE, the use of CDT with mechanical thrombolysis and/or local fibrinolysis is feasible and safe, with a very low rate of procedure-related complications. The use of CDT is associated with benefits at several levels, including improvement in hemodynamics, RV function and perfusion defects at 3 months after the procedure.
Keywords: Acute pulmonary embolism; Catheter-directed therapies; Mechanical thrombectomy; Fibrinolysis In-Situ; Pulmonary hypertension.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Grazina A & Teixeira BL (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Grazina A, Teixeira BL, Morais LA, Fiarresga A, Ramos R, da Silva TP, Albuquerque FB, et al. Catheter-directed therapies for high and intermediate-high risk patients with acute pulmonary embolism: Results from a multiparametric follow-up protocol. Open J Clin Med Case Rep. 2024; 2185.
Introduction
Anticoagulation alone has proven efficacy for the treatment of low- and intermediate-low-risk acute pulmonary embolism (PE) patients [1]. Nonetheless, intermediate-high- and high-risk PE are associated with a considerable risk of short-term circulatory collapse, death or long-term pulmonary hypertension (PH), ranging from 3 to 10%, when treated with anticoagulation alone [1]. Although systemic fibrinolysis decreases this risk by 50%, it significantly increases the risk of major bleeding (PEITHO trial) [2], which have limited the use of systemic fibrinolysis to high-risk patients with hemodynamic instability, as recommended in the current guidelines [3-5]. This limitation has led to growing interest in catheter-directed therapies (CDT) for patients with high-risk acute PE with contraindication or failure of systemic fibrinolysis and intermediate-high-risk patients who develop worsening hemodynamics despite anticoagulation [5]. CDT include percutaneous interventions, mainly catheter-directed mechanical thrombectomy and/ or catheter-directed local fibrinolysis, that are innovative, less invasive and allow faster perfusion defects resolution and hemodynamic improvement without the systemic hemorrhagic effects of systemic thrombolysis. Despite the existence of other devices, Indigo aspiration system (Penumbra Inc) is the most used in Europe [6]. Pulmonary Embolism Response Teams (PERT) have been created to deliver PE patients a better care, through engagement of multiple specialists in order to determine and coordinate the course of action in patients with acute PE [7]. Despite an increasing use of CDT, to date the clinical evidence of its benefits is still limited, as there are no adequately powered randomized controlled trials and current studies have been limited to immediate hemodynamic improvement or imaging surrogate markers [8,9]. For example, SEATTLE II trial was a single-arm study with a small cohort of high and intermediate-high risk PE patients submitted to catheter-directed fibrinolysis, that showed promising results with short-term improvement in Systolic Pulmonary Artery Pressure, as a potential surrogate for long-term outcomes [10].
Objectives: This study pretends to assess the long-term hemodynamical, pulmonary perfusion and clinical impact on high and intermediate-high risk patients with acute pulmonary embolism submitted to catheter-directed therapies.
Methods
Patient selection: Between 2020 and 2022, in a single tertiary center, consecutive high and intermediatehigh risk PE patients considered suitable for CDT by our PERT were prospectively enrolled in a multiparametric follow-up protocol. Selection criteria included patients with high-risk acute PE in whom systemic fibrinolysis was contraindicated or have failed and patients with intermediate-high risk acute PE with signs of worsening hemodynamics despite anticoagulation. Patients with PE clinical onset over two weeks and with “on transit” thrombus in inferior vena cava or right heart were considered unsuitable for catheterdirected therapies.
Procedure protocol: Procedure planning included assessment of hemodynamic and respiratory status, laboratory evaluation, bedside echocardiography, and careful evaluation of computed tomography angiography (CTA) scan in order to plan in advance the catheter approach (local fibrinolysis, mechanical thrombectomy or a combined approach). Femoral vein or right antecubital basilic vein were the used access routes. The procedure began with a right heart catheterization, using an Arrow Berman catheter (Teleflex) to fully assess hemodynamics. Then, this catheter is exchanged for a pigtail catheter to perform bilateral pulmonary angiogram and assess the perfusion defects more accurately. The decision between in-situ fibrinolysis, mechanical thrombectomy or both was made by the operators and based on several factors as thrombus burden, thrombus localization, hemodynamic status and bleeding risk. For the catheter-directed local fibrinolysis, an alteplase intrapulmonary perfusion through a Cragg-McNamara valved infusion catheter (Medtronic) was used at a rate of 1 mg/h for 12 hours, after a bolus of 1mg. For the catheter-directed mechanical thrombectomy, it was used the 8 and 12 French Indigo aspiration system (Penumbra Inc), to restore the perfusion in the most branches possible until achievement of a god angiographic result or until a blood loss (aspiration) of 300-350ml. All the patients completed 48 hours of unfractionated heparin. Afterwards, a full dosage direct oral anticoagulant was prescribed. Most patients took rivaroxaban 15mg twice daily for 3 weeks followed by 20mg once daily for at least 6 months.
Follow-up protocol: The follow-up protocol included laboratorial and echocardiographic evaluation, CTA scan, right heart catheterization and pulmonary angiogram at 3 months after CDT, clinical assessment at 3 and 12 months. Patients with residual chronic thromboembolic pulmonary hypertension (CTEPH) were referred to our pulmonary hypertension (PH) unit.
Statistical analysis: Baseline characteristics, clinical presentation, laboratorial, echocardiographic and CTA scan evaluation were noted at admission. Procedure data included hemodynamics, perfusion defects quantified using the modified Miller index, intervention, and complications. Continuous variables with normal distribution are presented as mean value and standard deviation (SD), continuous variables with non-normal distribution are presented as median and interquartile range (IQR) and categorical variables presented in absolute and relative values (percentage rounded to one decimal place). Laboratorial, echocardiographic, imaging, hemodynamic and angiographic data collected at 3 months was compared with the admission, using a paired samples t-Test analysis. Statistical analysis was done using the software SPSS version 25.0.
Results
Population baseline characteristics: During the analyzed period, a total of 39 patients (46.2% male, mean age 60 years old) with intermediate-high or high risk acute pulmonary embolism were consecutively submitted to CDT. Baseline characteristics are depicted in table 1 and are concordant with pulmonary embolism patients stratified as intermediate-high and high risk, with high rate of syncope at presentation, tachycardia, increased serum lactate, low PaO2 /FiO2 ratio and increased blood levels of troponin and NTproBNP. Admission echocardiogram shows RV dilation in 95% of the patients with RV systolic disfunction in 69% of the patients. Regarding medical background it was registered a 10% rate of active oncologic disease and 13% of previous venous thromboembolism.
Procedure data and related complications: Isolated intrapulmonary fibrinolysis with alteplase was performed in 71% of the cases, isolated mechanical thrombectomy with the Penumbra aspiration system in 10% and combined therapy in 18%. No major bleeding (leading to death, requiring a medical intervention or transfusion) was seen during or after the procedure. 1 pulmonary artery dissection and 1 Penumbra burr partial avulsion occurred, both treated with conservative measures with good result. No pulmonary artery perforation or pulmonary valve damage were observed. 1 patient developed persistent and refractory cardiogenic shock, leading to death. Procedure data is depicted in table 2.
Multiparametric follow-up: From the 39 patients submitted to catheter-directed therapies, 23 completed the follow-up at months (Figure 1), due to almost 10% of deaths, mainly for non-cardiovascular reasons and a significant rate of incomplete follow-up for several reasons. It was verified a significant number of foreign patients, that developed the PE event during travelling, and therefore were unable to complete the follow-up.
In the 23 patients that completed the follow-up, right heart catheterization data shows a statistically significant improvement in the patients’ hemodynamics with 3.6mmHg, 16.8mmHg and 10.7mmHg mean drops in RA, systolic PA and mean PA pressures, respectively (p<0.001), 1.61L/min and 0.85L/min/m2 mean increases in cardiac output and index respectively (p <0.001), and a1.65 Wood units decrease in the pulmonary vascular resistance (p 0.012). It was also seen an improvement in the perfusion defects with a mean drop of 8.7 points in the modified Miller index (p <0.001) and an improvement in the RV function with a mean decrease of 0.5 in the RV/LV ratio by CT-scan (p <0.001), a mean increase of 5.4mm in TAPSE (p <0.001) and a mean increase of 5.0cm/s in tricuspid annular s’ velocity (p<0.006). The hemodynamic parameters, perfusion defects and RV function data comparison between admission and 3 months after the intervention are illustrated in figures 2, 3, 4 and 5.
Table 1: Baseline characteristics, clinical presentation, laboratorial and imaging findings, and procedure data of intermediate-high- and high-risk pulmonary embolism patients submitted to catheter-directed therapies.
| Baseline characteristics (n = 39) | |||
|---|---|---|---|
| Age in years old (mean±SD) | 60.0 ± 17.6 | Previous VTE | 12.8% (5) |
| Gender (male) | 46.2% (18) | Oncologic disease | 10.3% (4) |
| Clinical and laboratorial findings (n= 39) | |||
| Syncope at presentation | 28.2% (11) | Serum lactate - mean±SD | 1.7 ± 1.6 |
| Dyspnea at presentation | 76.9% (30) | PaO2/FiO2 ratio - mean±SD | 262 ± 96 |
| Days from symptoms onset - median (IQR) | 1.0 (1.8) | hs-Troponin I - median (IQR) | 262 (520) |
| Systolic arterial pressure - mean±SD | 116 ± 26 | NT-proBNP - median (IQR) | 2775 (3910) |
| Heart rate - mean±SD | 102 ± 21 | Peak D-dimer - median (IQR) | 8835 (12254) |
| Imaging findings – initial work-up (n = 39) | |||
| Central PE in angio-CT scan | 34.2% (13) | Dilated RV in TTE | 94.6% (35) |
| RV/LV ratio angio-CT scan - mean±SD | 1.4 ± 0.2 | RV dysfunction in TTE | 69.4% (25) |
VTE: venous thromboembolism; PE: Pulmonary Embolism; RV: right ventricle; LV: left ventricle; NT-proBNP: N-terminal pro-B natriuretic peptide; TTE: transthoracic echocardiogram; CT: computed tomography.
Table 2: Procedure data relative to type of intervention and procedure related complications (PR – pulmonary valve regurgitation).
| Procedure data and complications (n = 39) | |||
|---|---|---|---|
| Thrombectomy + local fibrinolysis | 17.9% (13) | Pulmonary artery perforation | 0% |
| Isolated thrombectomy | 10.3% (4) | Pulmonary artery dissection | 2.6% (1) |
| Isolated local fibrinolysis | 71.2% (28) | Penumbra burr avulsion | 2.6% (1) |
| Any procedure complication | 5.6% (2) | Moderate-to-sever PR | 0% |
| Cardiogenic shock | 2.6% (1) | Cardiac tamponade | 0% |
| Major bleeding | 0% | Cardiovascular death | 2.6% (1) |
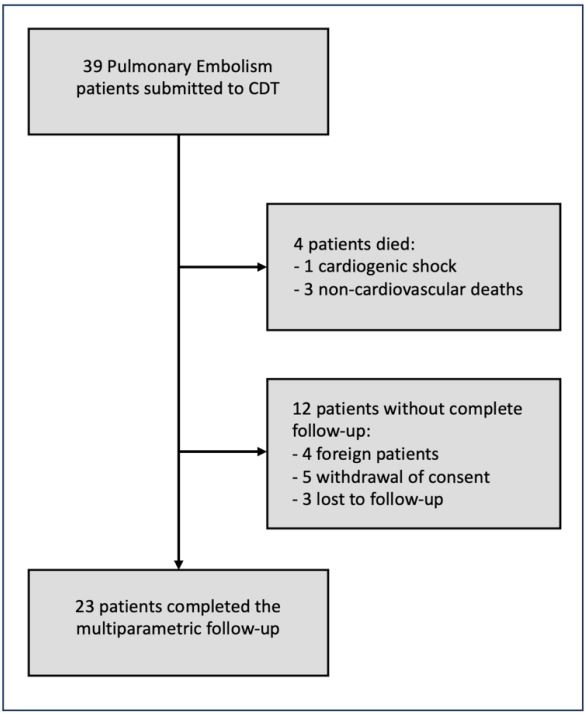
Figure 1: Study scheme of the 39 consecutive patients
enrolled after catheter directed therapies for intermediate-high and high risk acute pulmonary embolism.
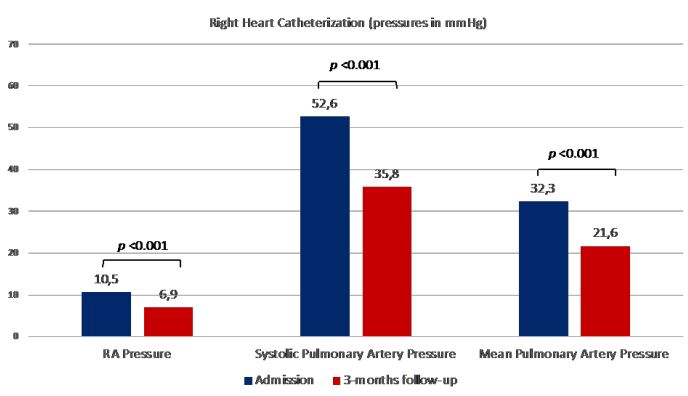
Figure 2: Right heart catheterization data comparison
between admission and 3 months (RA: right atrium).
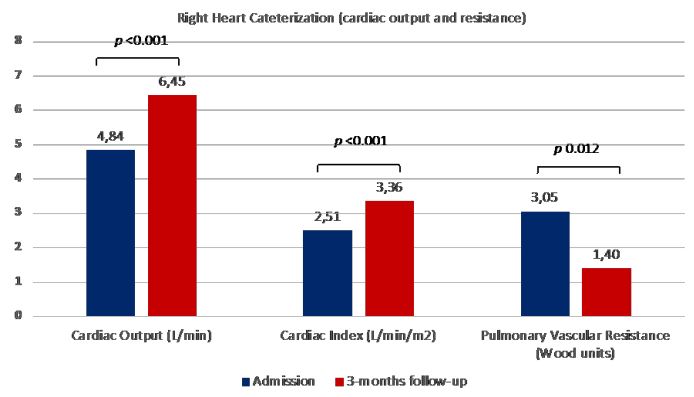
Figure 3: Right heart catheterization data comparison
between admission and 3 months.
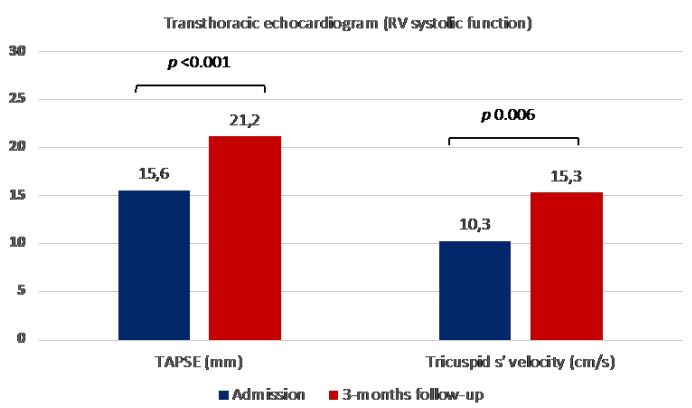
Figure 4: Right ventricular systolic function assessed by
transthoracic echocardiogram comparison between admission and 3 months (RV: right ventricle; TAPSE: tricuspid annular plane systolic excursion).
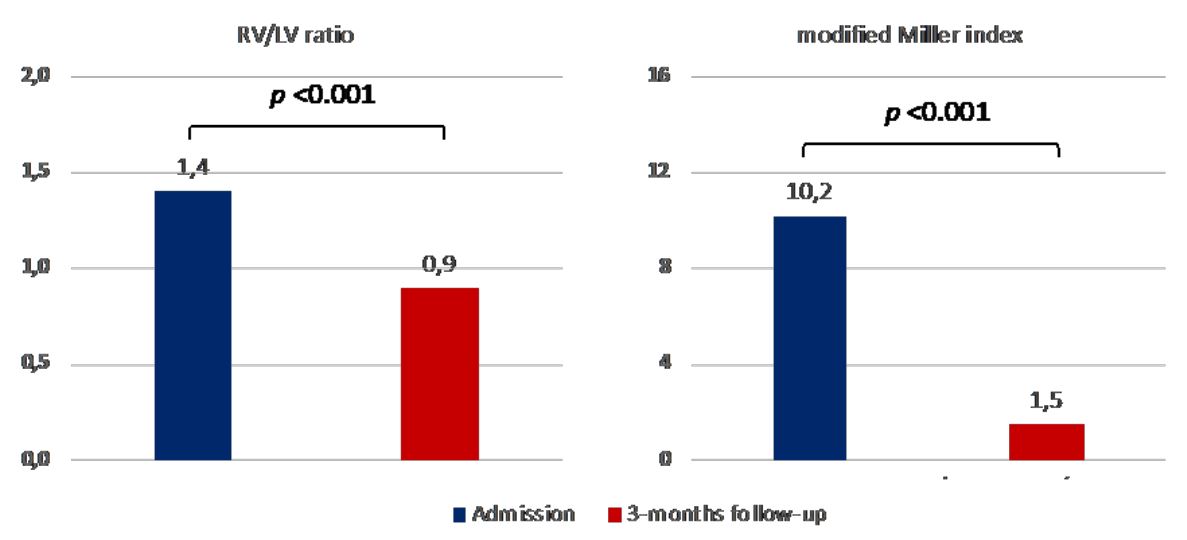
Figure 5: Right ventricular pressure overload/ dilation assessed by computed tomography and
residual perfusion defects/ thrombotic burden assessed by the modified Miller index comparison
between admission and 3 months (RV: right ventricle; LV: left ventricle).
During the follow-up, 4 patients died (overall mortality rate of 10.3%), but only one patient died from cardiac cause secondary to a worsening refractory cardiogenic shock. One patient died for oncologic disease progression, and two from non-cardiovascular causes.
Discussion
This study reports a low rate of procedural complications, around 5.6%, enhancing the feasibility and safety of catheter-directed therapies in the treatment of patients with intermediate-high and high risk acute pulmonary embolism. In the EXTRACT-PE trial, a 2.5% procedural rate of complications was reported, with 1.7% of major bleeding and 0.8% of device-related pulmonary vasculature injury [11]. Furthermore, both complications (one case of pulmonary artery dissection and one case of Penumbra device burr partial avulsion) were non-fatal, associated with the use of mechanical thrombectomy devices and both occurred in early phases of this device’s learning curve, leading the authors to believe that these complications could be minimized with increased operators experience. Despite the administration of catheter-directed fibrinolytic in nearly 90% (either isolated fibrinolysis or combined with mechanical thrombectomy), no major or life-threatening bleeding events were seen in the first 48h after the procedure. This is possibly related with the low dose of alteplase that was used, a total of 13mg (1mg bolus followed by 1mg/h infusion for 12 hours) which is about 8 times less than the recommended systemic fibrinolysis dose.
Most of previous trials used imaging parameters as surrogate markers to evaluate the immediate effect of CDT, most commonly the RV/LV ratio. In SEATTLE II trial, it was demonstrated that catheter-directed low dose fibrinolytic reduced mean RV/LV ratio in 0.42, mean pulmonary artery systolic pressure in 14.5mmHg and modified Miller Index score in 6.7 at 48h after the procedure [10]. In the EXTRACT-PE study, isolated mechanical thrombectomy with the 8 French Indigo aspiration system (Penumbra Inc) reduced the mean RV/LV ratio in 0.43 at 48h [11]. In the FLARE study, mechanical thrombectomy with Flow Triever System (Inari Medical) reduced mean RV/LV ration in 0.38 [12]. Of notice, our study provides more extensive and less immediate data of CDT benefits, including invasive direct assessment of hemodynamics instead of using imaging surrogate parameters. We obtained a mean reduction in the RV/LV ratio of 0.5 at 3 months that is similar with the rates described in previous studies. Besides that, our study also reports a significant improvement in RV systolic function (assessed by TAPSE and tricuspid annular s’ velocity), a significant decrease in pulmonary vasculature pressures and resistance measured invasively and a significant improvement in cardiac output measured invasively, all these benefits sustained at 3 months after the procedure. In our population, the invasive pulmonary angiogram at 3 months showed a higher mean reduction in modified Miller index when compared to the SEATTLE II trial, which may be explained by the ongoing incremental benefit of oral anticoagulation in the months after the acute event in reducing the residual perfusion defects.
The optimal treatment of intermediate-risk PE is still not established and current guidelines recommend anticoagulation alone, with catheter intervention reserved for patients who fail to respond to conservative therapy [5]. PEITHO trial showed that systemic fibrinolysis did result in a significant reduction in the combined primary endpoint of death and clinical deterioration, at the cost of a significant increase in major bleeding and intracranial hemorrhage [2]. Despite the fact that CDT have not been compared directly with anticoagulation alone in these patients, the authors believe that CDT (either with isolated or combined approaches) have several advantages. First, catheter-directed fibrinolysis may achieve the same intrapulmonary potential benefits without the systemic major bleeding risk of systemic fibrinolysis. Second, catheter-directed mechanical thrombectomy with aspiration systems allow faster and practically immediate reperfusion in main branches, avoiding further irreversible deterioration in unstable patients. Third, catheter-directed mechanical thrombectomy poses a very safe and efficient alternative in high-risk bleeding patients that have contraindication to fibrinolytic agents or even to anticoagulation. Fourth, both techniques appear to have an additive benefit on long term anticoagulation on reducing perfusion defects, pulmonary vasculature pressures and so, reducing the progression to chronic thromboembolic pulmonary hypertension (CTEPH).
Study limitations: The main limitation of this study was the lack of a comparator arm. Other limitations were the number of patients that did not complete the follow-up, the small sample size and the use of two different catheter-directed strategies either in combination or separately, according to the operator’s decision. Randomized comparative studies between CDT and anticoagulation alone in intermediate risk PE patients are needed to further consolidate the use of this therapies in this population and increase its level of recommendation.
Conclusion
In patients with intermediate-high- and high-risk PE, the use of CDT with mechanical thrombolysis and/or local fibrinolysis is feasible and safe, with a very low rate of procedure-related complications. The use of CDT is associated with benefits at several levels, including improvement in hemodynamics, RV function and perfusion defects at 3 months after the procedure.
Declarations
Statement of ethics: This study protocol did not require approval by the hospital ethical committee. Informed consent was collected from all patients.
Conflicts of interest statement: The authors have nothing to declare.
Funding sources: No funding.
Authors contribution: André Grazina and Luís Almeida Morais designed the study protocol. André Grazina, Bárbara Lacerda Teixeira, Francisco Barbas Albuquerque and Ana Santana collected and analyzed the data. André Grazina and Bárbara Lacerda Teixeira wrote the manuscript with support from Luís Almeida Morais, António Fiarresga, Ruben Ramos, Tiago Pereira da Silva and João Reis. Ana Galrinho, Duarte Cacela and Rui Cruz Ferreira coordinated the project.
Data availability statement: All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
References
- Giri J, Sista AK, Weinberg I, et al. Interventional therapies for acute pulmonary embolism: current status and principles for the development of novel evidence: a scientific statement from the American Heart Association. Circulation. 2019; 140: 774-801.
- Meyer G, Vicaut E, Danays, T et al. PEITHO Investigators. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014; 370: 1402-1411.
- Tapson VF, Friedman O. Systemic thrombolysis for pulmonary embolism: who and how. Tech Vasc Interv Radiol. 2017; 20: 162-174.
- Patel N, Patel NJ, Agnihotri K, et al. Utilization of catheter-directed thrombolysis in pulmonary embolism and outcome difference between systemic thrombolysis and catheter-directed thrombolysis. Catheter Cardiovasc Interv. 2015; 86: 1219-1227.
- Konstantinides S, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism. European Heart Journal. 2019; 41(4): 543-603.
- Pruszczyk P, Klok FA, Kucher N, et al. Percutaneous treatment options for acute pulmonary embolism: a clinical consensus statement by the ESC Working Group on Pulmonary Circulation and Right Ventricular Function and the European Association of Percutaneous Cardiovascular Interventions. EuroIntervention. 2022; 18(8): 623-638.
- Rosovsky R, Zhao K, Sista A, et al. Pulmonary embolism response teams: Purpose, evidence for efficacy and future research directions. Res Pract Thromb Haemost. 2019; 3: 315-330.
- Almarzooq ZI, Bergmark BA. Percutaneous Treatment of High-Risk Pulmonary Embolism: Bridging the Evidence Gap. European Heart Journal of Acute Cardiovascular Care. 2023.
- Aggarwal V, Giri J, Nallamothu BK. Catheter-Based Therapies in Acute Pulmonary Embolism: The Good, the Bad and the Ugly. Circulation: Cardiovascular Interventions. 2020; 13: 009353.
- Piazza G, Hohlfelder B, Jaff MR et al. A prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. JACC Cardiovascular Intervention. 2015; 8(10): 1382-1392.
- Sista AK, Horowitz JM, Tapson VF et al. Indigo Aspiration System for Treatment of Pulmonary Embolism: Results of the EXTRACT-PE Trial. JACC Cardiovascular Intervention. 2021; 14(3): 319-329.
- Tu T, Toma C, Tapson VF et al. A prospective, Single-Arm, Multicenter Trial of Catheter-Directed Mechanical Thrombectomy for Intermediate-Risk Acute Pulmonary Embolism: The FLARE Study. JACC Interventions. 2019; 12(9): 859-869.
