
Open Access, Volume 10
Comparative analysis of horizontal alveolar ridge augmentation: Guided bone regeneration versus screw-tenting techniques - A systematic review
Manoj Bhatia1; Anthony Murto1; Sidharth Bhatia1; Waqar Ahmed2; Fadi Barrak1,3*
1School of Medicine and Dentistry, University of Central Lancashire, UK.
2School of Mathematics and Physics, University of Lincoln, UK.
3VSS Academy, London, UK.
Fadi Barrak
School of Medicine and Dentistry, University of Central Lancashire, UK.
Email: fnbarrak@uclan.ac.uk
Received : Dec 18, 2023,
Accepted : Jan 08, 2024
Published : Jan 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
The aim of this study was to systematically review bone volume changes obtained via the use of the Guided Bone Regeneration Technique (GBR-T) versus the Screw-Tenting Technique (ST-T) in horizontally defective alveolar ridges. In addition to review and compare rates of complications pertaining to post-operative dehiscence with membrane exposure, graft exposure, graft loss or other unforeseen complications and rates of implant placement into grafted sites.
PRISMA protocol was used for systematic reviewing, electronic and manual searches of primary and secondary objectives were performed using the National Library of Medicine (MEDLINE via PubMed), EMBASE (Ovid), and EBSCO Host up to and including the 1st May 2023.
Three articles qualified under the stipulated inclusion and exclusion criteria. Regarding GBR-T, the mean horizontal ridge bone gain was 2.47±3.16 mm with a mean complication rate of 16.50%, a mean graft loss rate of 11.70% and a mean implant placement rate of 91.30%. Regarding ST-T, the mean horizontal ridge bone gain was 4.76.02±2.57 mm with a mean complication rate of 9.30%, a mean graft loss rate of 2.80% and a mean implant placement rate of 98.10%.
Both techniques are predictable in achieving horizontal ridge bone gains with low complication/failure rates leading to high second stage implant placement rates. The adjunctive use of tenting screws appears to be effective, offering additional benefit to the mechanism of space maintenance. Current evidence is however limited and of moderate risk-of-bias with heterogeneity within and between studies. Different interventions were performed by various clinicians with varying surgical skillsets in differing clinical environments using different biomaterials so caution must be used when interpreting these findings.
Keywords: Screw tenting; Alveolar bone; Augmentation; Guided bone regeneration; Biomaterials; Bone graft.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Barrak F (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Bhatia M, Murto A, Bhatia S, Ahmed W, Barrak F. Comparative analysis of horizontal alveolar ridge augmentation: Guided bone regeneration versus screw-tenting techniques - A systematic review. Open J Clin Med Case Rep. 2024; 2184.
Introduction
Alveolar bone undergoes dimensional changes following tooth loss due to various factors, such as periodontal disease, trauma, and pathology [1]. These changes unfold over a 1-year post-tooth extraction timeline [2]. The resulting horizontal and vertical ridge dimensional alterations, particularly buccolingually, underscore the need for augmentation before embarking on successful implant therapy
The pre-clinical insight that peri-implant bone sites with buccolingual thickness ≥1.5 mm exhibit fewer changes than those with <1.5 mm emphasises the pivotal role of augmentation in long-term success [3]. There are numerous regenerative techniques, such as Distraction Osteogenesis, Orthodontic tooth movement, Inlay/Onlay Bone Block Grafting, Ridge Splitting/Expansion, Osseodensification. However, this review focuses on Guided Bone Regeneration (GBR) to address alveolar bone defects.
Defined by [4], GBR deploys a barrier membrane over a bone defect to impede the ingress of rapidly proliferating epithelial and connective tissue cells. The major biological principles of GBR, succinctly coined as ‘PASS’ by [5], encompass primary/tension-free wound closure, adequate vascularity, space maintenance, and stability of the wound.
Barrier membranes, resorbable or non-resorbable, play a crucial role in providing space maintenance and stability to the clot within the defect [6]. Resorbable membranes, lauded for their handling and fewer exposures, are particularly suitable for certain applications [7], but are less suitable for vertical bone augmentation since they are less rigid [8]. The other advantage is that a second surgery is not required as they degrade preventing disruption of healing [9]. In contrast, non-resorbable membranes, while offering greater stability, come with a higher risk of perforation and wound dehiscence [10]. A second surgery is also required for membrane removal, nevertheless, clinical horizontal bone gains of up to 9 mm and vertical gains of up to 12 mm have been recorded [10].
Despite the evidence of membrane use and GBR definition, if there is no support by an underlying bone graft or bone substitute within the defect there may be a propensity for membrane collapse which in turn can affect space maintenance and wound stability [11]. Thus, if the grafted space is compromised due to membrane collapse, augmentation will be compromised [12].
Bone grafts and bone substitutes, integral to GBR, contribute to space maintenance and possess four principal biological properties: osteogenesis, osteoconduction, osteoinduction, and osteopromotion [14,15]. The types of grafts encompass autografts (patient’s own bone), allografts (another individual’s bone, usually obtained from treated cadaver bone and have osteoconductive and osteoinductive properties), xenografts (osteoconductive), and alloplasts (osteoconductive), each with its unique characteristics and applications. The principles of GBR showing the barrier membrane occluding a bone defect are shown in Figure 1.
First introduced by [16] GBR Technique (GBR-T) is considered a reliable and predictable technique for alveolar ridge augmentation. It involves the use of barrier membranes and bone grafts, yielding reproducible results with high long-term success rates. It has been extensively described as yielding reproducible results with high-long term success rates [8,17,18]. For illustration purposes (Figure 2) shows a schematic diagram of the GBR technique.
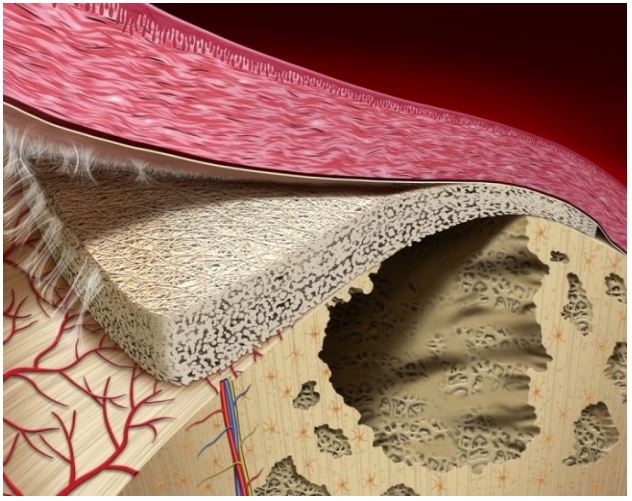
Figure 1: Principles of GBR depicting barrier membrane
occluding a bone defect [13].
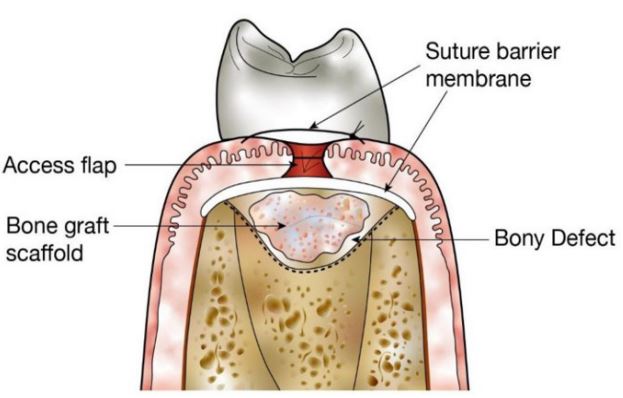
Figure 2: Schematic of the GBR Technique [19].
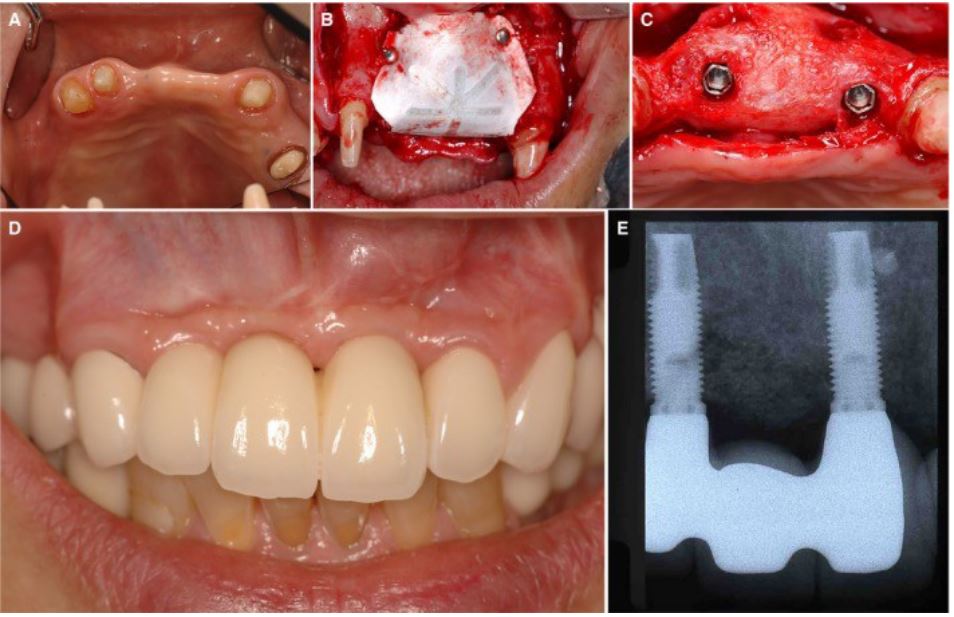
Figure 3: GBR-T for a horizontal ridge augmentation using e-PTFE non-resorbable membrane and xenograft
bone substitute in the pre-maxilla. A) Pre-operative view of horizontal bone defect, B) e-PTFE non-resorbable membrane fixated with titanium pins overlying xenograft bone substitute, C) Implant placement 7 months after GBR-T, (D and E) 1-year post-op photograph and radiograph [20].
A challenging aspect of particulate bone grafting with resorbable membranes is graft immobilisation. This is key as there is an increased dehiscence rate and reduced augmentation if there is no immobilisation [21].
In addition to the use of barrier membranes and bone grafts/bone substitutes alone or in combination, adjunctive space-maintaining modalities such as titanium mesh trays [9,22], Titanium-Reinforced PTFE (Ti-PTFE) membranes [23], tenting techniques [24-26] or their combinations [27-29] also serve as variations attempting to avoid this collapse and promote enhanced stability. Figure 3 shows GBR-T for a horizontal ridge augmentation using e-PTFE non-resorbable membrane and xenograft bone substitute in the pre-maxilla.
Tenting techniques: The tenting techniques, as described by [24,30,25], raise the periosteum to create and maintain space thus favouring stability. These techniques aim to serve as adjuncts to GBR [31-34,11,23], supporting the membrane against mechanical influences.
The Tent-Pole technique used dental implants as space-maintaining tent-poles, achieving stability for the surrounding iliac crest-derived bone graft in severely resorbed mandibular ridge areas of ≤6 mm height, resulting in mean vertical bone gains of 10 mm after a 5-year follow-up. Augmentation was reliable with 99.5% of implant success despite experiencing short-term paraesthesia in 17.1% of the cases with the important drawback being the need for extraoral incisional access, thus rendering this procedure tailored to hospital settings and far from general practice [24].
The Cortical autogenous tenting technique involves securing autogenous cortical bone blocks to the recipient site via titanium screws leaving a gap which is filled with a bone graft/bone substitute mix. The blocks supersede the use of membranes by tenting the periosteum. Complications reported included wound infection, graft exposure/failure and resorption. This technique requires a second surgical site, increasing morbidity and complexity relative to the GBR Technique [35].
The Khoury technique further modified this Cortical autogenous tenting technique to attain bone augmentation via the splitting of the autologous cortical bone block graft into thinner sections which were then secured via titanium screws alongside an autologous particulate bone graft infill. Similarly, this discarded the need for membranes and carried with it greater morbidities [36].
A direct modification of GBR-T, Screw-Tenting Technique (ST-T) introduces titanium screws to create space within the defective recipient site. This alteration, while achieving significant bone gain, introduces challenges such as wound dehiscence and screw exposure. The ST-T technique demands a meticulous approach [25], through treating severe localised mandibular/maxillary vertical ridge defects, achieving a mean vertical bone gain of 9.7 mm. A schematic diagram of the screw tenting technique is shown in Figure 4 whilst Figure 5 shows clinical photographs demonstrating ST-T.
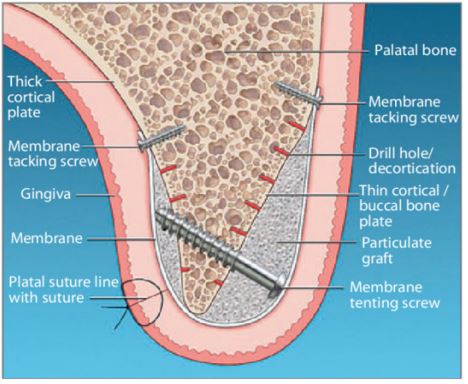
Figure 4: Schematic of the Screw-Tenting technique [11].
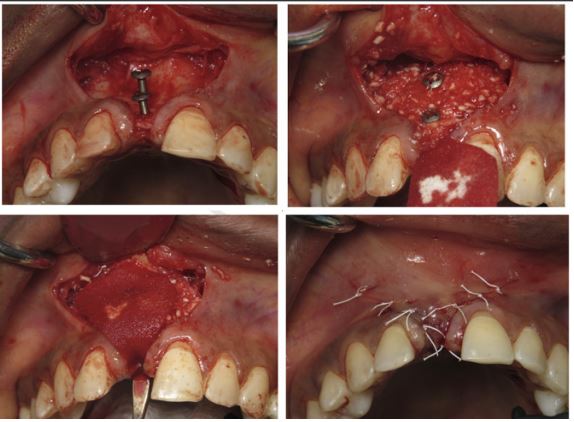
Figure 5: Clinical photographs demonstrating ST-T-Titanium tenting screws secured to the defective recipient
site; Bone graft/bone substitute placement up to the extent of the screwheads; Coverage with resorbable membrane; Primary closure [23].
Comparison between guided bone regeneration and Screw-Tenting Techniques: The comparative analysis between GBR-T and ST-T illuminate’s nuances in horizontal bone gains and associated complications [37]. Evaluated different GBR methods, showcasing an overall mean horizontal bone gain of 2.27±1.68 mm and a mean vertical bone gain of 3.05±1.02 mm. The literature, however, lacks direct comparisons between GBR-T and ST-T.
[38], in a systematic review of vertical ridge augmentation procedures, found no significant differences between various techniques, including GBR-T. However, ST-T was not considered in their analysis [39]. Focused on implant success rates, highlighting the efficacy of tenting techniques in achieving vertical bone gains but without direct comparison to GBR-T. The existing body of evidence presents a gap in systematically comparing these techniques.
Tenting screws have been used as adjuncts for GBR in several studies [40,31,11,23,33,34] with the intention of improving graft stability as previously mentioned. It is acknowledged that limitations of space maintenance identified with GBR have been considered in the addition of tenting screws to alveolar ridge defects.
This systematic review aims to provide clear guidelines regarding the judicious use of tenting screws in horizontal bone defects. The overarching question is whether and when the incorporation of screw tenting can modify and enhance the GBR approach. The goal is to assess if the adjunctive use of tenting screws offers tangible clinical enhancements in terms of bone gains and complication rates. The hypothesis underlying this investigation is that if screw tenting systematically improves the GBR protocol, it could potentially obviate the need for more invasive procedures involving autologous bone block harvesting and its associated morbidities.
Materials & Methods
The study employed the preferred reporting Items for Systematic Review and Meta-Analysis (PRISMA) Protocols, consisting of a 27-item checklist and a 4-phased diagram, to prevent and identify bias. The research question focused on the effectiveness of the Screw-Tenting Technique (ST-T) compared to the Guided Bone Regeneration Technique (GBR-T) in patients with horizontal alveolar bone ridge defects. The research followed the Participants, Intervention, Comparison, Outcome, Timeline (PICOT) framework and had a 12-month follow-up.
Study selection for the systematic review was dictated by the following criteria:
Inclusion criteria
• Population: Systemically healthy and non-syndromic human subjects of ≥18 years of age presenting with horizontal alveolar ridge defects requiring augmentation.
• Intervention: Screw-tenting Technique (ST-T).
• Comparison: Guided Bone Regeneration Technique (GBR-T).
• Outcome: Clinical horizontal alveolar ridge volumetric changes.
• Timeline: Follow-up of up to 12 months.
• Study Design: Randomised Clinical Trials (RCT), Controlled Clinical Trials (CCT), Prospective/Retrospective Cohort Studies (PCS/RCS), and Case Series (CS).
Exclusion criteria
• Case reports, pre-clinical, animal or in-vitro studies.
• Studies involving human subjects presenting with vertical alveolar ridge defects requiring augmentation.
• Studies involving maxillary sinus floor elevation.
• Studies evaluating procedures aiming to alter horizontal ridge augmentation for purposes other than tooth
Replacement
• Studies evaluating procedures with the sole use of radiographs.
Primary outcomes focused on horizontal bone dimensional changes, while secondary outcomes included complication rates, implant placement effectiveness, and graft loss.
Automated electronic literature searches were performed using general bibliographic databases; National
Library of Medicine (MEDLINE via PubMed), EMBASE (Ovid), and EBSCO Host up to 1st May 2023. These are large citation databases which will encompass a wide distribution of sources of information, sufficient for an effective and comprehensive search.
The searches utilised MESH terms combined via Boolean operators (AND, OR). The following keywords were used.
(“Tent Screw Pole Technique” or “Cortical Tenting” or “Tenting Technique” or “Screw Tenting” or “Tent-Pole” or “Bone screw”) and (“Guided Bone Regeneration” or “GBR”) and (“resorbable membrane” or “non-resorbable membrane” or “collagen membrane” or “titanium-reinforced membrane”) or (“particulate bone graft” or “bone substitute”) and (“alveolar ridge augmentation” or “ridge augmentation” or “horizontal ridge augmentation” or “alveolar bone defect reconstruction” or "bone augmentation" or “severely atrophic ridge”).
Manual literature searches were done for all reference lists related to included studies which were then checked against previous systematic reviews. No search filters were set regarding publication date, language, or type of study. One reviewer screened titles/abstracts based on inclusion/exclusion criteria, with inconclusive articles subjected to full-text review. Data extraction was performed for relevant articles. Data collected included study details, participant characteristics, surgical procedures, and outcomes. Primary outcomes involved changes in alveolar ridge width, while secondary outcomes included implant placement and complication rates.
Regarding the primary outcome of the Ridge Width (RW) change was calculated as RW Follow up minus RW baseline, leading to change in alveolar width (ΔRW):

The percentage (%ΔRW) was calculated as follows:
The secondary outcomes of interest were calculated from the Implant Placement Rate (IPR) relative to the number of implants (Ni) placed in number of grafted (Ngs) sites was calculated as follows:
The percentage of implant complication rate (%CR) was calculated from the number of complications (Nc) and number of grafted sites (Ngs) as follows:
The graft loss rate (GLR) calculated as a percentage from number of grafts lost Ng and number of grafted sites (Ngs) as follows:
Risk of bias for randomised controlled trials was assessed using the Cochrane Risk-of-Bias (RoB2) Tool, and non-randomised trials were assessed with the Risk-of-Bias in Non-Randomised Studies of Intervention (ROBINS-I) Tool. Statistical analysis involved a random-effects model to account for variability.
Results
From the 163 articles identified, 143 underwent screening, and 28 were eligible for full-text evaluation. Ultimately, three articles met the inclusion criteria for the systematic review. Figure 6 shows PRISMA search and selection flowchart using a template extracted from Page et al. 2021.
Table 1 shows a list of important studies but were not used due to the exclusion criteria used for this work.
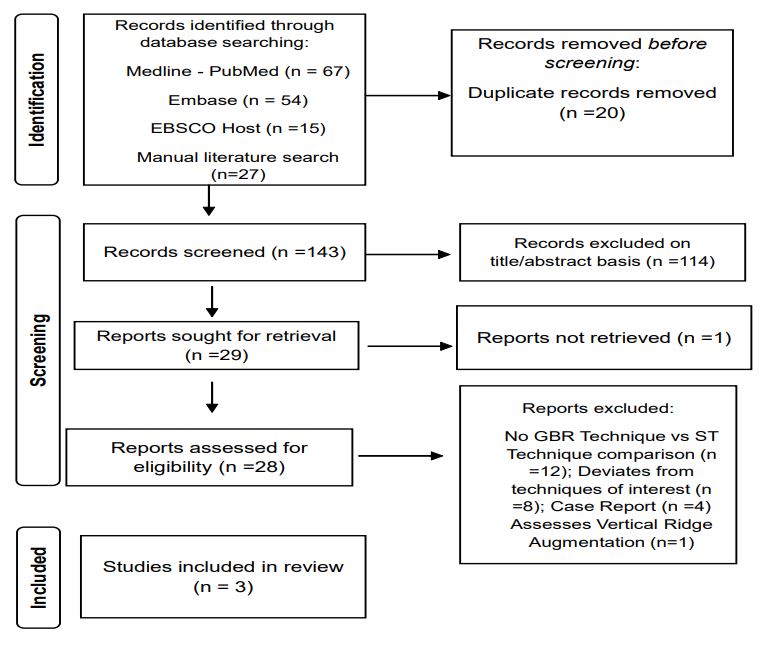
Figure 6: PRISMA search and selection flowchart. Template extracted from
Page et al 2021.
Table 1:Studies excluded and reasons.
| Excluded article | Reference | Reason for exclusion |
|---|---|---|
|
Caldwell et al. 2015 [41] |
Lateral Alveolar Ridge
Augmentation Using Tenting
Screws, Acellular Dermal
Matrix, and Freeze-Dried Bone Allograft Alone or with Particulate Autogenous Bone. Int J Periodontics Restorative Dent 2015; 35(1): 75-84 |
No GBR vs TS technique comparison |
|
Chasioti et al. 2013 [11] |
Maintaining space in
localized ridge augmentation
using guided bone
regeneration with tenting screw technology. Quintessence Int. 2013 Nov-Dec; 44(10): 763-71. |
Case report |
| Daga et al. 2018 |
Tentpole technique for bone
regeneration in vertically
deficient alveolar ridges:
A prospective study. J Oral Biol Craniofac Res. 2018 Jan-Apr; 8(1): 20-24. |
Assesses Vertical Ridge Augmentation |
|
Deeb et al. 2017 [23] |
Effect of biologic materials
on the outcomes of
horizontal alveolar ridge
augmentation: A retrospective study. Clinical & Experimental Dental Research 2021; 7(2): 147-156. |
No GBR vs TS technique comparison |
|
Doan & Le 2020 [42] |
Efficacy of the Tent-Pole
Technique in Horizontal
Ridge Augmentation. Pesqui.
Bras. Odontopediatria Clin. Integr. 2020; 20: e5643 |
No GBR vs TS technique comparison |
|
Doong-Woon et al. 2015 |
The Role of Two Different
Collagen Membranes for
Dehiscence Defect Around
Implants in Humans. J Oral Implantol 2015; 41(4): 445-450. |
No GBR vs TS technique comparison |
| Durrani et al. 2023 |
Predictable guided bone
regeneration. Journal of
Indian Society of
Periodontology 2023; 27(1): 104-113. |
Case report |
| Farias et al. 2021 |
Horizontal Bone Augmentation
in the Posterior Atrophic
Mandible and Dental
Implant Stability Using the Tenting Screw Technique. Int J Periodontics Restorative Dent 2021; 41(4): e147. |
No GBR vs TS technique comparison |
|
Golob Deeb eta al. 2020 |
Effect of postoperative
steroids on clinical
outcomes and radiographic
findings of horizontal alveolar ridge augmentation: A retrospective study. J Periodontol 2020; 91(7):917-925. |
No GBR vs TS technique comparison |
| Guo et al. 2023 |
Clinical evaluations of
alveolar ridge preservation
in compromised extraction
sockets with cortical-lamina anchoring technique: Case series study. Clin Implant Dent Relat Res. 2023 Feb; 25(1):46-56. |
No GBR vs TS technique comparison |
| Jung et al. 2009 |
A randomized-controlled
clinical trial evaluating
clinical and radiological
outcomes after 3 and 5 years of dental implants placed in bone regenerated by means of GBR techniques with or without the addition of BMP-2. Clin Oral Implants Res. 2009 Jul; 20(7):660-6. |
Deviates from technique
of interest |
| Kakar et al. 2018 |
Lateral alveolar ridge
augmentation procedure using
subperiosteal tunneling
technique: a pilot study. Maxillofacial Plastic & Reconstructive Surgery 2018; 40(1):0-1. |
Deviates from technique
of interest |
|
Khojasteh 2012 [43] |
Localized bone augmentation
with cortical bone blocks
tented over different
particulate bone substitutes: a retrospective study. Int J Oral Maxillofac Implants. 2012 Nov-Dec; 27(6):1481-93. |
Deviates from technique
of interest |
|
Kuoppala et al. 2013 |
Outcome of treatment of
implant-retained overdenture
in patients with extreme mandibular bone resorption treated with bone grafts using a modified tent pole technique. J Oral Maxillofac Surg. 2013 Nov; 71(11):1843-51. |
Deviates from technique
of interest |
| Korpi et al. 2012 |
Long-term follow-up of
severely resorbed mandibles
reconstructed using tent
pole technique without platelet-rich plasma. J Oral Maxillofac Surg. 2012 Nov; 70(11):2543-8. |
Deviates from technique
of interest |
| Korpi et al. 2013 |
Tent-pole approach to treat
severely atrophic fractured
mandibles using immediate
or delayed protocols: preliminary case series. J Oral Maxillofac Surg. 2013 Jan; 71(1):83-9. |
Deviates from technique
of interest |
| Le et al. 2016 |
Treatment of Labial Mucosal
Recession Around Maxillary
Anterior Implants with
Tenting Screws, Particulate Allograft, and Xenogenic Membrane: A Case Report. J Oral Implantol 1 October 2016; 42 (5): 427-431. |
No GBR vs TS technique comparison |
| Le & Hayashi 2022 |
The Aesthetic Contour Graft
- Enhancing peri-implant
soft tissue contours and
pontic sites with guided bone regeneration. Journal of Esthetic & Restorative Dentistry 2022; 34(1):188-203. |
Case report |
| Lin et al. 2022 |
Horizontally ridge
reconstruction using
titanium mesh with tenting
screw vs autologous bone graft: a retrospective study, 29 June 2022, PREPRINT (Version 2) available at Research Square. |
No GBR vs TS technique comparison |
|
Marx et al. 2002 [24] |
Severely resorbed mandible:
predictable reconstruction
with soft tissue matrix
expansion (tent pole) grafts. J Oral Maxillofac Surg. 2002 Aug; 60(8): 878-88; discussion 888-9. |
Deviates from technique
of interest |
| Nevins et al. 2014 |
Recombinant human
platelet-derived growth
factor BB for reconstruction
of human large extraction site defects. Int J Periodontics Restorative Dent. 2014 Mar-Apr; 34(2): 157-63. |
No GBR vs TS technique comparison |
| Reddy et al. 2016 |
Space Maintenance Using
Tenting Screws in Atrophic
Extraction Sockets. J Oral
Implantol. 2016 Aug; 42(4): 353-7. |
Case report |
|
Simon et al. 2010 [34] |
Alternative to the gold
standard for alveolar ridge
augmentation: tenting screw
technology. Quintessence Int. 2010 May;41(5):379-86. |
No GBR vs TS technique comparison |
| Wu et al. 2022 [6] |
Application of a tent-pole
screw technology in
reconstruction of severe
alveolar bone defect: a retrospective study of 30 patients. Journal of Shanghai Jiao Tong University (Medical Science). 2022; 42 (6) 768-777) |
No GBR vs TS technique comparison |
Table 2: Included study data extraction table.
| Author/Year | Group | No of patients |
No. of grafted sites |
Membrane used |
Particulated bone graft/ bone substitute |
No. of implants used |
No of complications |
No. of grafts lost |
Follow- up/ months |
|---|---|---|---|---|---|---|---|---|---|
|
Cesar Neto et al 2020 |
ST GBR |
10 18 |
22 22 |
Collagen (BioGide*) Collagen (BioGide*) |
DBBM (Bio-Oss*) DBBM (Bio-Oss*) |
22 22 |
3 1 |
0 0 |
6-8 |
|
Deeb et al 2017 [22] |
ST GBR |
35 31 |
35 31 |
Collagen (BioGide*) ePTFE |
FDBA (Puros)+DNNM(Bio- Oss) FDBA (Puros)+DNNM(Bio- Oss) |
33 22 |
4 16 |
3 12 |
6 |
| Johar 2019 | ST GBR |
50 50 |
50 50 |
ePTFE ePTFE |
50 50 |
3 0 |
0 0 |
6 |
RCT: Randomised Controlled Trial; RCS: Retrospective Cohort Study; ePTFE: Expanded Polytetrafluoroethylene; FDBA: Freeze-Dried Bone Allograft; DBBM: Deproteinised Bovine Bone Mineral; ST: Screw-Tenting technique; GBR: Guided Bone Regeneration technique; NR: Not Recorded.
Included in the systematic review were 3 articles (see Table 2 for data extraction) consisting of 1 randomised clinical trial (RCT) (Johar, 2019) and 2 retrospective cohort studies (RCS) (Cesar Neto et al. 2020 and Deeb et al. 2017).
Was considered to have a ‘Some concerns’ risk of bias, whereas Cesar [22] were at a ‘Moderate’ risk of bias (see Figures 7 & 8 and Appendices sections 2.1, 2.2 and 2.3 for detailed individual study risk of bias tool assessments).
Regarding eligibility criteria, [23] and Cesar Neto et al. 2020 included a pre-operative assessment to ascertain horizontal ridge defects in healthy complication-free individuals 18 years or older, smoking less than 10 cigarettes/day and requiring implant therapy. Similarly, Johar 2019 included healthy complicationfree individuals with horizontal ridge defects with at least 6 months of healing but more specifically with an age range between 20 and 50 years of age who were excluded if there was any history of smoking.
[23] Failed to specify participant characteristics regarding mean age, range, and gender ratios. Neto et al. 2020 enrolled participants with an age range of 19-79 and mean ages of 51.95±18.50 and 52.77±13.09 for females and males respectively consisting of 64.3% females and 35.7% males in a ratio of approximately 2:1. Johar 2019 enrolled participants with an age range of 20-42 and mean ages of 28.78±6.32 and 27.62±5.42 for females and males respectively consisting of 50% females and 50% males in a ratio of 1:1, showing a slightly younger studied cohort in comparison. See Table 3 below for narrative breakdown of included studies.
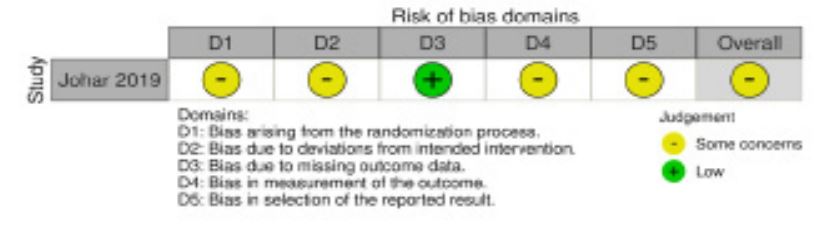
Figure 7: Randomised risk of bias following RoB2 tool guidelines using the
robvis package.
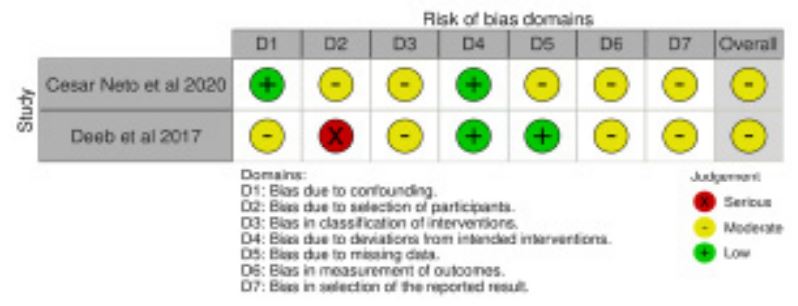
Figure 8: Non-randomised studies risk of bias following ROBINS-I tool guidelines using the robvis package.
Table 3: Included study narrative synthesis.
| Author/Year of publication | ||||||
|---|---|---|---|---|---|---|
| Debb et al. 2017 [23] | Cesar Neto et al. 2020 | Johar 2019 | ||||
| Follow-up & Study design |
6 month follow-up retrospective cohort study; No dropouts |
6-8 month follow-up retrospective cohort study; 2 dropouts (TS) |
6 month follow-up randomised controlled study; no dropouts |
|||
| Participants | ||||||
| Setting | Treated at the Department of Oral and Maxillofacial Surgery at the Virginia Commonwealth University School of Dentistry, USA between 6th November 2013 to 25th March 2016, by senior level residents under direct supervision by the director of the graduate implants program. |
Treated at a private practice in Sao Paulo, Brazil between 2013 and 2018, by a single operator. |
Treated at King Abdulaziz University clinics in Jeddah, Saudi Arabi between 2010 and 2015, by a single operator. |
|||
| Eligibility criteria | Pre-operative CBCT assed to characterise defect dimensions, adults 18 years or older who had undergone HRA with TS, GBR, or Tunnel Technique. Excluded if a component of VRA was performed, if HRA was performed with simultaneous implant inversion, or if additional methods were used like PRP or BMP |
Systematically healthy ASA I/II adults 18 years or older, under periodontal maintenance with at least 1 site of less than 4mm bone width at 1mm below crest level or requiring GBR for enough ridge width to accommodate an implant angulation to allow for a screw- retained restoration. Excluded if presence of periodontal disease, pregnancy/lactation, smoking 10 daily cigarettes or more, bone metabolic disease, medication affecting bone metabolism, biphosphates in the last 4 years, history of malignancy, radio/chemotherapy for malignancy in the past 5 years |
Edentulous area with horizontal ridge deficiency Siebert Class I in need of implant therapy. Time after extraction of minimum of 6 months. Age range 20-50 years old. Absence of periodontal disease. Excluded if presence of Diabetes Type I/ II, history of smoking, history of metabolic bone or collagen disease, medication affecting bone/collagen metabolism like cortisone or bisphosphonates, pregnancy, history of failed prior ridge augmentation procedure. |
|||
| Characteristics | ||||||
| Age | ||||||
| Range | NR | 19-79 | 19-79 | 20-42 | 20-42 | |
| Mean (SD) | NR | 51.95±18.50 | 52.77±13.09 | 28.78±6.32 | 27.62±5.42 | |
| Sex F:M (%) | NR | 18F(64.3%): 10M(35.7%) | 25F(50%): 25M(50%) | |||
| Number of participants |
35 | 31 | 18 (16) | 10 | 50 | 50 |
| Number of grafted sites |
35 | 31 | 24 (22) | 22 | 50 | 50 |
| Site location (Maxilla: Mandible) |
NR | NR | 9:13 | 12:10 | NR | NR |
| Intervention | ||||||
| Group Test: Control | ST | GBR | ST | GBR | ST | GBR |
| Membrane used | Collagen (Bioguide*) |
e-PTFE (Cytoplast *) | Collagen (Bioguide*) | Collagen (Bioguide*) | e-PTFE (NR) | e-PTFE (NR) |
| Membrane fixation | No | Screws | No | No | Tacks | Tacks |
| Bone graft/Bone substitute used |
FDBA (Puros*) & DBBM (Bios- Oss *) 1:1 mix ratio |
FDBA (Puros*) & DBBM (Bios-Oss *) 1:1 mix ratio |
Autogenous from adjacent sites and DBBM (Bios-Oss *) (Mix ratio NR) |
Autogenous from adjacent sites and DBBM (Bios-Oss *) (Mix ratio NR) |
Autogenous from maxillary tuberosity and DBBM (Bios-Oss *) (Mix ratio NR) |
Blood clot only |
| Tenting screw used/n | Pro-FixTM/2-4 | None | NeodentTM/1 | None | NR | None |
| Tenting screw dimension/mm |
NR length, 1.5 diameter 3.5 screwhead diameter |
8-10 length, 1.5 diameter 3.5 screwhead diameter |
NR | |||
| Tenting screw location/mm |
Placed 3-6 away from buccal bone |
Placed 1 from crest and 4 away from buccal bone |
NR | |||
| Pre-operative measures |
Intra-venous 2 g Amoxicillin or 900 mg Clindamycin |
1 hour pre-op 2 g Amoxicillin & 4 mg Dexamethasone |
None | |||
| Surgical procedure | LA ± I/V, full thickness crestal incision and trapezoidal flap reflection. E-PTFE membrane secured palatally/lingually with tack, FDBA/DBBM mix application, then e-PTFE membrane secured over with tacks and tension free closure for GBR group. Tenting screw placement, then FDBA/DBBM mix application and collagen membrane coverage and tension free closure for TS group. |
Mid-crestal incision and trapezoidal flap reflection one tooth away from defect. Soft tissue remnants removed, decortication of buccal bone, autogenous/DBBM mix application for both groups, tenting screws applied for TS group only, membrane placement and tension free closure. When needed, lingual/palatal sites grafted as well. |
LA (xylocaine 2%), crestal incision and trapezoidal flap reflection. Decortication of buccal bone, autogenous/DBBM mix application for TS group, none for GBR group, then membrane tackling and tension free closure. |
|||
| P o s t - o p e r a t i v e measures |
Amoxicillin 500 mg x 3/day 1 week If allergic, then Clindamycin 300 mg x4/day 1 week Reviews at 1 week, 1 month, 6months |
Amoxicillin 875 mg x 2/day 1 week Nimesulide (NSAID) 100 mg x2/day 3 days Sodium Dipyrone 500 mg x4/day 2 days Chlorhexidine 0.12% x3/day 3 weeks Sutures removed 2-3 weeks later |
Antibiotics for 1 week (dose/intake regime not specified) Ibuprofen (dose/intake regime not specified) Chlorhexidine (dose/intake not specified) Suture removal (intervals not specified) |
|||
| Outcomes | ||||||
| Methods of measurement |
CBCT 6 months post-operative to asses for implant placement. Success determined based on graft material consolidation and the ability to place implant of appropriate size without further grafting |
All CBCTs obtained pre-operative and 6-8 month postoperative. iCAT Classic* unit used by single calibrated examiner. Baseline grid drawn on DICOM sections of baseline image with vertical line at bucco- oral centre of ridge. Horizontal lines drawn perpendicular to this at 1, 3, 5, 7 mm levels from bone crest |
Initial measurements at implant site at bone crest and 10mm Apical Change in Ridge Width/mm of relevance for comparison across studies. ΔRW ( Apical Late measurement – Apical Initial measurement). Change in Percentage/Δ% in measurements adjusted for Age and initial measurement. (Later measurement – Initial measurement/ Initial measurement) x100 |
|||
| Primary Outcome Mean (Standard Deviation) |
Implant placement rate/% (Implant placed n / Sample size, n)x100 |
Ridge Width (RW)/mm at 1, 3, 5 & 7 mm ridge levels (RWx) Change in Rudge Width (ΔRW)/mm at (RWx final – RWx baseline) RW1 and ΔRW1 (at 1mm ridge level) of relevance for comparison across studies |
Apical and Cervical Initial and Alte measurements/mm. Apical Change in Ridge Width/mm of relevance for comparison across studies. ΔRW (Apical Late measurement – Apical Initial measurement). Change in Percentage/Δ% in measurements adjusted for Age and initial measurement. (Late measurement – Initial measurement/Initial measurement) x100 |
|||
| Secondary Outcomes | Membrane exposure ± wound dehiscence rate, n (%). (Membrane exposure ± wound dehiscence rate / Sample size) x100. Graft loss, n (%). (Graft loss/Sample size) x100. Courses of antibiotics, median (range). Postoperative visits, median (range). |
Change in lingual Ridge Width (ΔLRW)/mm at 1, 3, 5, & 7mm ridge levels (LRWx final – LRWx baseline) |
Membrane exposure ± wound dehiscence rate, n(%). Implant placement rate/% (Implant placed, n / Sample size, n) x100 |
|||
ePTFE: Expanded Polytetrafluoroethylene; FDBA: Freeze-Dried Bone Allograft; DBBM: Deproteinised Bovine Bone Mineral; ST: Screw-Tenting Technique; GBR: Guided Bone Regeneration Technique; NR: Not Recorded; LA: Local Anaesthetic; I/V: Intra-Venous; CBCT: Cone Beam Computed Tomography.
Primary outcomes: Horizontal ridge bone gain: The measurement methods employed by the studies differed, with [23] utilising post-operative CBCTs to assess implant eligibility and with success being determined by the ability to place an implant without the need of further grafting. But, as this study focused more on one of the secondary outcome measures, this being implant placement rate, this included study failed to collate data for the primary outcome of interest cesar compared pre- and post-operative CBCTs, and measured ridge widths at the bone crest with a surgical stent further standardised with an automated poly-gauge at augmentation surgery and then at implant placement time 6-months later. The mean ΔRW (horizontal bone gain) varied between 2.47 and 4.76 mm, showcasing the impact of technique variation. Conversion to percentages revealed consistently enhanced effects with titanium screws, with ST-T groups consistently demonstrating greater bone gains than GBR-T groups-see Table 4.
Findings can be collated into mean ΔRW horizontal ridge bone gains of 4.76.02±2.57 mm for the ST-T and 2.47±3.16 mm for the GBR-T groups (Table 6).
Table 4: Mean (SD)/mm primary outcomes for GBR-T.
| GBR | Johar 2019 | Cesar Neto et al. 2020 | Mean |
|---|---|---|---|
| WRBasline | 3.81±0.24 | 3.28±1.57 | 3.55±1.55 |
| RWFollow-up | 7.50±0.46 | 4.54±2.62 | 6.02±2.66 |
| ∆RW | 3.69±0.84 | 1.25±3.05 | 2.47±3.16 |
| %∆RW |
102.32 (97.81–106.83) |
n/a n/a |
n/a n/a |
Table 5: Mean (SD)/mm primary outcomes for ST-T.
| GBR | Johar 2019 | Cesar Neto et al. 2020 | Mean |
|---|---|---|---|
| WRBasline | 3.66±0.22 | 3.18±1.57 | 3.42±1.59 |
| RWFollow-up | 9.45±0.35 | 6.09±2.99 | 8.18±3.01 |
| ∆RW | 5.79±0.75 | 3.72±2.46 | 4.76±2.57 |
| %∆RW |
170.46 (166.16-174.79) |
n/a n/a |
n/a n/a |
Table 6: Summary of Mean (SD) primary outcomes.
| ST | GBR | |
|---|---|---|
| WRBasline | 3.42±1.59 | 3.55±1.55 |
| RWFollow-up | 8.18±3.01 | 6.02±2.66 |
| ∆RW | 4.76±2.57 | 2.47±3.16 |
Secondary outcomes: Cesar Neto et al. (2020) and Johar (2019) reported 100% implant placement rates for both ST-T and GBR-T [23] presented slightly lower rates, with 94.29% for ST-T and 70.97% for GBR-T, suggesting potential technique-specific variations in implant success – see Table 7.
Cesar reported complication rates of 13.64% (ST-T) and 4.55% (GBR-T), while [22] had rates of 11.43% (ST-T) and 51.61% (GBR-T). Reported a 6.00% complication rate for ST-T and none for GBR-T, highlighting the need for a nuanced understanding of complications associated with each technique – see Table 8.
Cesar Neto et al. (2020) and Johar (2019) recorded no graft losses, while [23] reported rates of 8.57% (ST-T) and 38.71% (GBR-T) – (Table 9). The variability in graft loss rates underscores the need for a meticulous examination of the factors contributing to graft stability.
Table 7: Summary of included study implant placement rates.
|
Cesar Net et al. 2020 |
Deeb et al. 2017 [23] | Johar 2019 | Mean |
|---|---|---|---|
| ST (%) | 100.00 | 94.29 | 100.00 |
| GBR (%) | 100.00 | 70.79 | 100.00 |
Table 8: Summary of included study complication rates.
| Cesar Net et al. 2020 | Deeb et al. 2017 [23] | Johar 2019 | |
|---|---|---|---|
| ST (%) | 13.64 | 11.43 | 6.00 |
| GBR (%) | 4.55 | 51.61 | 0.00 |
Table 9: Summary of included graft loss rates.
| Cesar Net et al. 2020 | Deeb et al. 2017 [23] | Johar 2019 | |
|---|---|---|---|
| ST (%) | 0.00 | 8.57 | 0.00 |
| GBR (%) | 0.00 | 38.71 | 0.00 |
In pooled data, the ST-T group demonstrated higher implant placement rates (98.10%) compared to the GBR-T group (91.30%). Complication rates were 9.30% for ST-T and 16.50% for GBR-T, and graft loss rates were 2.80% for ST-T and 11.70% for GBR-T.
Discussion
Primary outcome: Horizontal ridge bone gain: A mean ΔRW of 4.76±2.57 mm was found when using the ST-T compared to 2.47±3.16 mm when using the GBR-T demonstrating greater horizontal bone gains with the adjunctive use of titanium screws. These mean values encompass the results extracted from Johar 2019 and Cesar Neto et al. 2020.
Johar 2019 yielded ΔRWs of 5.79±0.75 mm for the ST-T group and 3.69±0.84 mm for the GBR-T group, demonstrating a significant difference in horizontal bone gains. There was a statistically significant difference in participant age and initial measurements in favour of the ST-T group, which was considered a confounding factor. Age affects healing potential [44] thus contributing to potentially skewed results, nevertheless regression analysis was performed to take this into consideration. Consequently, on converting to percentages, %ΔRWs of 170.46% (166.16-174.79) for the ST-T group and 102.32% (97.81-106.83) for the GBR-T group, also demonstrated an enhanced effect of titanium tenting screw use considering age and initial measurement disparities.
Similarly, Cesar Neto et al. 2020 yielded ΔRWs of 4.76±2.57 mm for the ST-T group and 1.25±3.05 mm for the GBR-T group, corroborating the findings obtained by Johar 2019. It could be construed that titanium tenting screws exert graft support and stability thus contributing to greater horizontal bone gains.
The main aim of GBR is to maintain adequate space to allow for osteogenesis to take place unhindered [5]. An animal study by [45] indicated in their findings that space maintenance and membrane coverage are essential in GBR using collagen resorbable membranes, pointing out that membrane collapse leads to reduced regenerative capability. Another animal study by showed that wound closure displaces the bone substitute which in turn leads to coronal collagen membrane collapse. Tacking pins and bone block substitutes were found to enhance this graft displacement.
Johar 2019 yielded greater horizontal bone gains compared to Cesar Neto et al. 2020 in both ST-T and GBR-T groups. This is most likely due to the use of more rigid and stable non-resorbable membranes as opposed to the resorbable collagen membranes used in Cesar Neto et al. 2020. When comparing the ST-T group results of both studies, the tenting screws exert a further effect on horizontal bone gains irrespective of membrane type. The added effect of titanium tenting screws has been shown here to further improve this sought-after stability.
Following from this, although [25] comes with its limitations due to lack of a true control group as well as inexistent clinically and/or radiographically CBCT-derived measurements of ΔRW, they indirectly compared collagen resorbable membrane use without fixation in the ST-T group with non-resorbable membrane use with fixation in the GBR-T group [18] aimed to discern if collagen resorbable membrane fixation led to superior clinical bone gains and determined that regeneration was greater with fixation, albeit with no statistical difference so evidence supporting this was weak. Hence, in [23], greater implant placement rates in the ST-T group (without fixation) group relative to the GBR-T group (with fixation) may infer that tenting screws enhanced resorbable membrane stability with no fixation to the extent that greater horizontal bone gains were achieved than with non-resorbable membrane use with fixation.
These findings could also potentially focus the use of non-resorbable membranes for more severe ridge defect situations whereby tenting screws and resorbable membranes could be intended to solve other specific defects. Given the higher rates of complications associated with non-resorbable membranes [10], this could avoid unnecessary morbidity for the patient requiring certain horizontal ridge defect augmentations.
This could be part of the reason why [38] found and suggested ST-T as being most useful in horizontal bone augmentation. When evaluating their included studies involving ST-T [24,33,11,40] for both vertical and horizontal ridge augmentation, they all involved the use of a resorbable membrane or acellular dermal matrix.
According to Urban et al. 2021 and within the limitations of scarcity of relevant RCTs, the Khoury technique involving cortical bone tenting and the ‘sausage’ GBR-T, are both similarly effective at horizontal bone augmentation. Balci Yuce & Taşdemir 2022 compared GBR-T with block grafting for horizontal ridge augmentation and both achieved similar results in terms of bone gain and complications. Block grafting was found to be more time consuming and costly. From this perspective if the adjunctive use of screw tenting is beneficial for GBR, it could be that in certain cases, its clinical bone gains could potentially surpass those of block grafting not only from the standpoint of clinical bone gain but also of complication rates.
Secondary outcomes: Implant placement rate: ST-T groups generally showed higher rates, although membrane type may influence outcomes. The nuanced details of implant placement, such as the number of screws used, warrant further exploration to elucidate their impact on success rates.
Complication Rate: GBR-T had higher rates, potentially linked to non-resorbable membrane use and graft material excess. The inclusion of thick and thin gingival biotypes and meticulous recording of site locations could unveil additional insights into the factors influencing complication rates.
Graft Loss Rate: Rates were higher in GBR-T, especially in [22], possibly due to variable operator skillsets. A more in-depth exploration of the operator's experience and skill level in handling graft materials could contribute to a more nuanced understanding of graft stability. Demonstrated strengths in sample size, defined controls, and reproducible measurements. In contrast, [22] lacked a true control group, potentially impacting the reliability of the results. Johar (2019) faced challenges with confounding variables and a significant increase in ridge measurements, suggesting possible biases that need to be acknowledged and addressed in future research.
Several factors contribute to the variability observed across the studies. Decortication techniques, differing measurement methods, allocation concealment, confusion bias, information bias, variable graft/ membrane combinations, site specificity, and the absence of histological findings collectively influence the interpretation of results. A thorough understanding of these sources of variability is crucial for contextualizing and generalizing the findings.
Conclusion
Based on the limited compiled evidence, both the GBR-T and the ST-T can achieve horizontal bone gains with subsequent effective and complication free second-stage implant placements.
The adjunctive use of tenting screws is a simple surgical treatment option which according to the literature is easy to execute enabling graft adaptation on alveolar ridge insofar as it uses screws and particulated bone. It can be inferred that screw tenting can offer additional benefits to space maintenance leading to an increase in horizontal clinical bone gain. Nevertheless, this is based on a limited range of moderate risk-of-bias evidence with heterogeneity within and between the included studies. Variable interventions were performed by different clinicians with a range of surgical skillsets and training in different clinical environments. A range of biomaterials were also utilised with different instruments so interpretation must be done cautiously.
In future the research could focus on the potential effects of tenting screw use in simultaneous immediate/early implant placement with guided bone regeneration in comparison to delayed second-stage implant placement relative to the grafted sites of interest. If screw tenting can enhance clinical bone gain at this stage, the omission of a second surgery would be much appreciated by clinicians and patients. This review of screw tenting in vertical alveolar ridge augmentation could also help discern if the use of procedures involving autologous block grafting with greater morbidity rates, could be replaced in certain situations giving way to less invasiveness and potential complications.
References
- Retzepi M, Donos N. Guided Bone Regeneration: Biological principle and therapeutic applications. Clin Oral Implants Res. 2010; 21(6): 567-76.
- Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics. Restorative Dent. 2003; 23(4): 313-23.
- Urban IA, Montero E, Monje A. Effectiveness of vertical ridge augmentation interventions: A systematic review and metaanalysis. J Clin Periodontol. 2019; 46: 319-339.
- Laney WR. Glossary of oral and maxillofacial implants. Berlin: Quintessence Publishing Co Ltd. 2007; 1-212.
- Wang HL, Boyapati L. “PASS” principles for predictable bone regeneration. Implant Dent. 2006; 15(1): 8-17.
- Yang Ze, Wu C, Shi H, Luo X, Sun H, et al. Advances in Barrier Membranes for Guided Bone Regeneration Techniques. Front Bioeng Biotechnol. 2022; 10: 921576.
- Chiapasco M, Casentini P, Zaniboni M. Bone augmentation procedures in implant dentistry. International Journal of Oral & Maxillofacial Implants. 2009; 24: 237-259.
- Simion M, Jovanovic SA, Trisi P, Scarano A, Piatelli A. Vertical ridge augmenation around dental implants using a membrane technique and autogenous bone or allografts in humans. Int J Periodontics Restorative Dent. 1998; 18: 8-23.
- Lindhe J, Lang NP, Karring T. Clinical Periodontology and Implant Dentistry (5th edition). Oxford: Blackwell Munksgaard. 2008. Louis PJ, Gutta R, Said-Al-Naief N, Bartolucci AA. Reconstruction of the maxilla and mandible with particulate bone graft and titanium mesh for implant placement. J Oral Maxillofac Surg. 2008; 66(2): 235-45.
- Schliephake H, Dard M, Planck H, Hierlemann H, Stern U. Alveolar ridge repair using resorbable membranes and autogenous bone particles with simultaneous placement of implants: an experimental pilot study in dogs. Int J Oral Maxillofac Implants. 2000; 15(3): 364-73.
- Chasioti E, Chiang TF, Drew HJ. Maintaining space in localized ridge augmentation using guided bone regeneration with tenting screw technology. Quintessence Int. 2013; 44(10): 763-71.
- Wallace S, Gellin R. Clinical evaluation of freeze-dried cancellous block allografts for ridge augmentation and implant placement in the maxilla. Implant Dent. 2010; 19: 272-9.
- Elgali I, Omar O, Dahlin C, Thomsen P. Guided bone regeneration: materials and biological mechanisms revisited. Eur J Oral Sci. 2017; 125(5): 315-337.
- Wang W, Yeung KW. Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact. Mater. 2017; 2: 224-247.
- Kolk A, Handschel J, Drescher W, Rothamel D, Kloss F, et al. Current trends and future perspectives of bone substitute materials-From space holders to innovative biomaterials. J. Cranio Maxillofac. Surg. 2012; 40: 706-718.
- Nyman S, Karring T. Regeneration of surgically removed buccal alveolar bone in dogs. J Periodontal Res. 1979; 14(1): 86-92.
- Cucchi A, Vignudelli E, Napolitano A, Marchetti C, Corinaldesi G. Evaluation of complication rates and vertical bone gain after guided bone regeneration with non-resorbable membranes versus titanium meshes and resorbable membranes. A randomized clinical trial. Clin Implant Dent Relat Res. 2017; 19(5): 821-832.
- Wessing B, Lettner S, Zechner W. Guided Bone Regeneration with Collagen Membranes and Particulate Graft Materials: A Systematic Review and Meta-Analysis. Int J Oral Maxillofac Implants. 2018; 33(1):87-100.
- Zhao R, Yang R, Cooper PR, Khurshid Z, Shavandi A, Ratnayake J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules. 2021 May 18;26(10):3007.
- Elgali I, Omar O, Dahlin C, Thomsen P. Guided bone regeneration: Materials and biological mechanisms revisited. Eur J Oral Sci. 2017; 125(5): 315-337.
- Carpio L, Loza J, Lynch S, Genco R. Guided bone regeneration around endosseous implants with anorganic bovine bone mineral. A randomized controlled trial comparing bioabsorbable versus non-resorbable barriers. J Periodontol. 2000; 71(11): 1743-9.
- Boyne PJ: Maxillofacial surgery, in Habal MB, Reddi AH (eds): Bone Grafts and Bone Graft Substitutes. Philadelphia, PA, W.B. Saunders. 1992; 291.
- Deeb GR, Tran D, Carrico CK, Block E, Laskin DM, et al. How Effective Is the Tent Screw Pole Technique Compared to Other Forms of Horizontal Ridge Augmentation? J Oral Maxillofac Surg. 2017; 75(10): 2093-2098.
- Marx RE, Shellenberger T, Wimsatt J, Correa P. Severely resorbed mandible: predictable reconstruction with soft tissue matrix expansion (tent pole) grafts. J Oral Maxillofac Surg. 2002; 60(8): 888-9.
- Le B, Rohrer MD, Prasad HS. Screw “tent-pole” grafting technique for reconstruction of large vertical alveolar ridge defects using human mineralized allograft for implant site preparation. J Oral Maxillofac Surg. 2010; 68: 428-35.
- Khoury F, Antoun A, Missika P. Bone Augmentation in Oral Implanto- logy. Berlin, London: Quintessenz. 2007.
- Thor A. Reconstruction of the anterior maxilla with platelet gel, autogenous bone, and titanium mesh: a case report. Clin Implant Dent Relat Res. 2002; 4(3): 150-5.
- Simion M, Jovanovic SA, Tinti C, Benfenati SP. Long-term evaluation of osseointegrated implants inserted at the time or after vertical ridge augmentation. A retrospective study on 123 implants with 1-5-year follow-up. Clin Oral Implants Res. 2001; 12(1): 35-45.
- Fugazzotto PA. Report of 302 consecutive ridge augmentation procedures: technical considerations and clinical results. Int J Oral Maxillofac Implants. 1998; 13(3): 358-68.
- Hempton TJ, Fugazzotto PA. Ridge augmentation utilizing guided tissue regeneration, titanium screws, freeze-dried bone, and tricalcium phosphate: Clinical report. Implant Dent. 1994; 3(1): 35-7.
- Buser D, Dula K, Belser U, Hirt HP, Berthold H. Localized ridge augmentation using guided bone regeneration. I. Surgical procedure in the maxilla. Int J Periodontics Restorative Dent. 1993; 13(1): 29-45.
- Becker W, Becker BE, McGuire MK. Localized ridge augmentation using absorbable pins and e-PTFE barrier membranes: A new surgical technique. Case reports. Int J Periodontics Restorative Dent. 1994; 14(1): 48-61.
- Mengel R, Flores-de-Jacoby L. Implants in regenerated bone in patients treated for generalized aggressive periodontitis: a prospective longitudinal study. Int J Periodontics Restorative Dent. 2005; 25(4): 331-41.
- Simon BI, Chiang TF, Drew HJ. Alternative to the gold standard for alveolar ridge augmentation: tenting screw technology. Quintessence Int. 2010; 41(5): 379-86.
- Le B, Burstein J, Sedghizadeh PP. Cortical tenting grafting technique in the severely atrophic alveolar ridge for implant site preparation. Implant Dent. 2008; 17(1): 40-50.
- Khoury F, Hanser T. Three-Dimensional Vertical Alveolar Ridge Augmentation in the Posterior Maxilla: A 10-year Clinical Study. Int J Oral Maxillofac Implants. 2019; 34(2): 471-480.
- Wessing B, Urban I, Montero E, Zechner W, Hof M, et al. A multicenter randomized controlled clinical trial using a new resorbable non-cross-linked collagen membrane for guided bone regeneration at dehisced single implant sites: interim results of a bone augmentation procedure. Clin Oral Implants Res. 2017; 28(11):e218-e226.
- Elnayef B, Monje A, Gargallo-Albiol J, Galindo-Moreno P, et al. Vertical Ridge Augmentation in the Atrophic Mandible: A Systematic Review and Meta-Analysis. Int J Oral Maxillofac Implants. 2017; 32(2): 291-312.
- Pourdanesh F, Esmaeelinejad M, Aghdashi F. Clinical outcomes of dental implants after use of tenting for bony augmentation: A systematic review. Br J Oral Maxillofac Surg. 2017; 55(10): 999-1007.
- Becker W, Becker BE, McGuire MK. Localized ridge augmentation using absorbable pins and e-PTFE barrier membranes: A new surgical technique. Case reports. Int J Periodontics Restorative Dent. 1994; 14(1): 48-61.
- Caldwell GR, Mills MP, Finlayson R, Mealey BL. Lateral Alveolar Ridge Augmentation Using Tenting Screws, Acellular Dermal Matrix, and Freeze-Dried Bone Allograft Alone or with Particulate Autogenous Bone. Int J Periodontics Restorative Dent. 2015; 35(1): 75-84.
- Le B, Burstein J, Sedghizadeh PP. Cortical tenting grafting technique in the severely atrophic alveolar ridge for implant site preparation. Implant Dent. 2008; 17(1): 40-50.
- Khojasteh A, Behnia H, Shayesteh YS, Morad G, Alikhasi M. Localized bone augmentation with cortical bone blocks tented over different particulate bone substitutes: a retrospective study. Int J Oral Maxillofac Implants. 2012; 27(6): 1481-93.
- Clark D, Nakamura M, Miclau T, Marcucio R. Effects of Aging on Fracture Healing. Curr Osteoporos Rep. 2017; 15(6): 601-608.
- Oh TJ, Meraw SJ, Lee EJ, Giannobile WV, Wang HL. Comparative analysis of collagen membranes for the treatment of implant dehiscence defects. Clin Oral Implants Res. 2003; 14(1): 80-90.
