
Open Access, Volume 10
Radical surgery for highly advanced gastric cancer with direct invasion to transverse colon, splenic serosa, and pancreas inducing pancreatic duct infection: A case report
Junichiro Tanaka*; Yuji Kondo; Takako Nirei; Yuichiro Yoshioka; Yoshiro Kubota
Department of Surgery, Kikkoman General Hospital, Chiba, Japan 100 Miyazaki, Noda-city, Chiba 278-0005, Japan.
Junichiro Tanaka
Department of Surgery, Kikkoman General Hospital, Chiba, Japan 100 Miyazaki, Noda-city, Chiba
278-0005, Japan.
Tel: +81-4-7123-5911;
Email: junjunkonnichiwa@yahoo.co.jp
Received : Dec 15, 2023,
Accepted : Jan 03, 2024
Published : Jan 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Background: According to the GLOBOCAN 2020 results, gastric cancer is the fifth most commonly diagnosed cancer, and fourth most common cause of cancer death worldwide. An estimated 6-27% of patients with gastric cancer show invasion of the adjacent organs at diagnosis. In a previous study, curative resection was shown to significantly improve the prognosis of patients without peritoneal or liver metastases. Herein, we present a case of gastric cancer with invasion of the adjacent organs in a patient who underwent curative surgery.
Case presentation: An 80-year-old woman presented with body weight loss and slight fever. Upper gastrointestinal endoscopy revealed Borrmann type 3 gastric cancer extending from the gastric fundus to the corpus. Contrast-enhanced computed tomography (eCT) revealed extensive invasion of the gastric cancer into the transverse colon and pancreas. The eCT also revealed gas in the pancreatic duct, indicating that the gastric lumen was connected to the pancreatic duct because of the tumor. We performed en-bloc tumor resection via total gastrectomy with D2 lymph node dissection, distal pancreatectomy, and partial colectomy. The patient was postoperatively diagnosed with T4b (SI: pancreatic, transverse colon, and splenic serosa), N0 Stage IIIA gastric cancer. The histological type was poorly differentiated adenocarcinoma. Adjuvant chemotherapy was initiated two months after surgery, but was continued for only two months because of severe adverse events. Two years after surgery, the patient remains well.
Conclusion: Advanced gastric cancer with extensive invasion of the adjacent organs but no distant metastasis can be treated with en-bloc tumor resection.
Keywords: Gastric cancer; Direct invasion; Case report; Curative en-bloc resection; Pancreatic duct infection; Prognosis.
Abbreviations: CT: Contrast-Enhanced Computed Tomography; GC: Gastric Cancer; EGD: Esophagogastroduodenoscopy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Tanaka J (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Tanaka J, Kondo Y, Nirei T, Yoshioka Y, Kubota Y. Radical surgery for highly advanced gastric cancer with direct invasion to transverse colon, splenic serosa, and pancreas inducing pancreatic duct infection: A case report. Open J Clin Med Case Rep. 2024; 2180.
Introduction
According to the results of the GLOBOCAN 2020, gastric cancer is the fifth most commonly diagnosed cancer and the fourth most common cause of cancer-related deaths worldwide [1,2]. Approximately 6-27% of patients with Gastric Cancer (GC) display invasion of the adjacent organs at diagnosis [3-9], and prognosis of these patients can be improved with curative surgery [3-7,10]. Of the patients with T4b GC, none with liver metastasis and approximately 15% with peritoneal metastasis undergo curative surgery [11]. Although curative resection does not improve the prognosis of patients with peritoneal or liver metastases, significantly better prognosis has been observed in patients without curative resection [11]. Thus, curative resection of T4b GC without distant metastasis may be linked to good prognosis. Herein, we present a case of GC with adjacent organ infiltration treated with en-bloc resection of the tumor through total gastrectomy combined with distal pancreatosplenectomy and partial colectomy. The present patient also developed infection of the pancreatic duct due to fistulation of the stomach and pancreatic duct caused by tumor invasion, which, to the best of our knowledge, has not been reported previously. This study was conducted in accordance with the SCARE criteria [12].
Case Presentation
An eighty-year-old woman presented with the symptoms of abdominal pain, slight fever of 37-38°C, and body weight loss. Upper Gastrointestinal (GI) examination performed one month prior to presentation revealed a gastric tumor, while Esophagogastroduodenoscopy (EGD) showed a type 3 tumor in the gastric fundus and corpus (Figure 1a). However, food residues covering the tumor surface prevented precise observation. Colonoscopy revealed an irregular surface elevation in the splenic flexure of the colon (Figure 1b), in which an adenocarcinoma was detected by biopsy. Contrast-enhanced computed tomography (eCT) revealed advanced GC with extensive invasion of the transverse colon, spleen, and pancreas (Figure 2a,b). Peritoneal dissemination and lymph node metastasis were suspected. The eCT image also showed gas in the pancreatic duct, indicating fistulation from the stomach to the pancreatic duct due to tumor invasion (Figure 2b). This fistula was presumed to be the cause of the patient’s low-grade fever. Thus, relatively rapid surgery was performed to control bacterial infection of the pancreatic duct and ensure resection of the advanced GC. Open surgery was performed, and extensive invasion of the GC into the pancreas and transverse to the descending colon was detected. Fortunately, no obvious peritoneal dissemination was observed. Therefore, a total gastrectomy with D2 lymphadenectomy combined with distal pancreatectomy, partial colectomy, and cholecystectomy was performed. Cholecystectomy was added as it is performed along with total gastrectomy as the standard procedure in our institute. The resected gastric tumor measured 160×80 mm (Figure 3a). Pathological tests revealed a poorly differentiated adenocarcinoma of the stomach invading the pancreas, transverse colon, and splenic serosa (Figure 3b-e). No metastasis was identified in the dissected lymph nodes or peritoneum. The pathological cancer stage was IIIA, according to both the TNM Classification of Malignant Tumours-8th edition [13] and the 15th edition of the Japanese Classification of Gastric Carcinoma[14]. Approximately two months after surgery, we initiated adjuvant chemotherapy with tegafur/gimeracil/oteracil, which was discontinued after only two months due to severe adverse events. Two years after surgery, the patient remains alive without relapse.
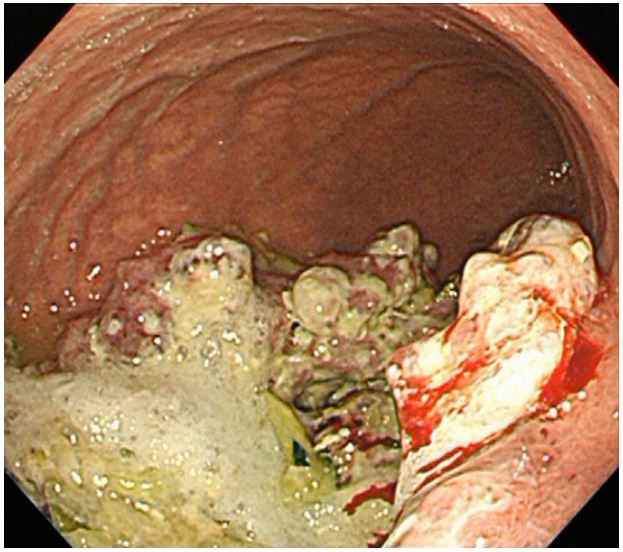
Figure 1a: EGD showing a large type 3 tumor in the fundus and corpus of the stomach. The surface of the tumor
was largely covered with food residue which prevented
detailed observation.
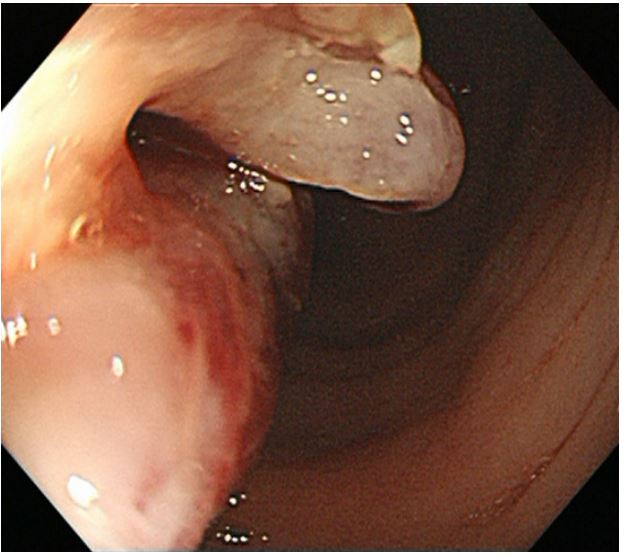
Figure 1b: Colonoscopy showing an irregular surfaced
elevation in the splenic flexure of the colon.
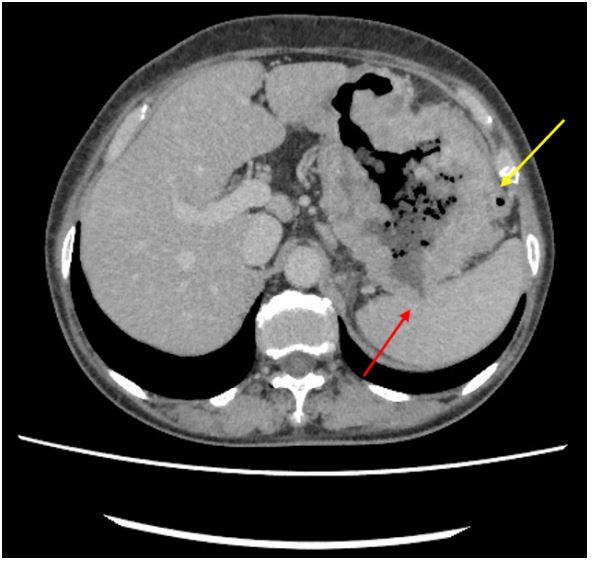
Figure 2a: Invasion of gastric cancer to the splenic serosa (red arrow) and transverse colon (yellow arrow) was
suspected based on eCT results.
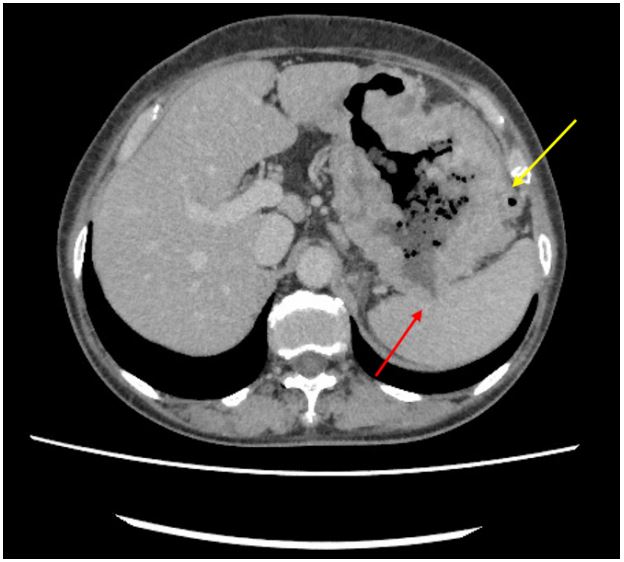
Figure 2b: Gastric cancer invasion to the pancreatic body
and tail (red arrow). Air can be seen in the pancreatic
duct (yellow arrow).
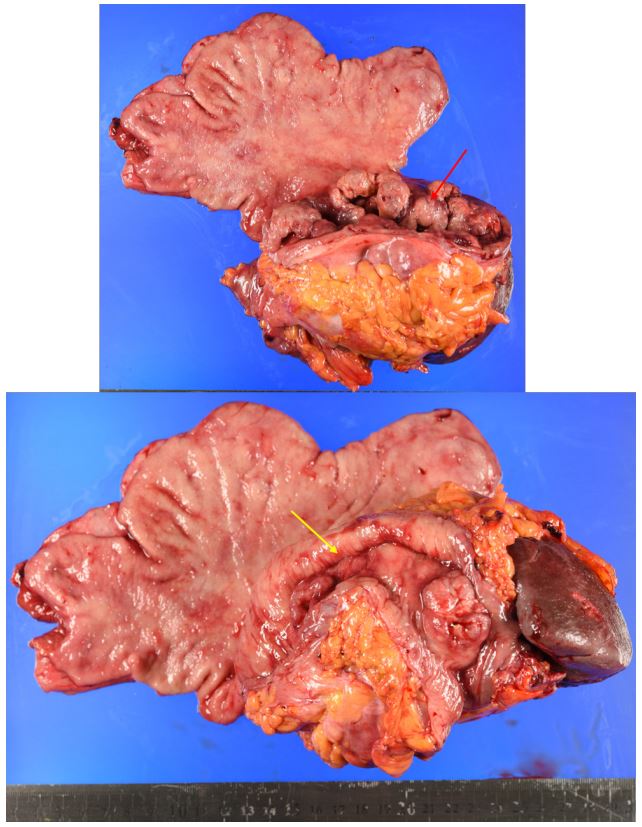
Figure 3a: Macroscopic view of the en-bloc resected specimen including the stomach, spleen, transverse colon,
pancreatic body, and tail. The primary gastric cancer lesion and invasion to the transverse colon are highlighted
with red and yellow arrow, respectively.
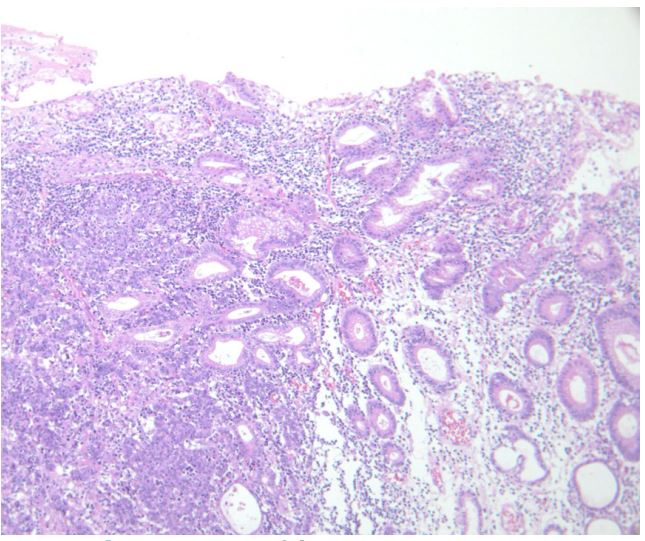
Figure 3b: H&E image of the primary gastric cancer
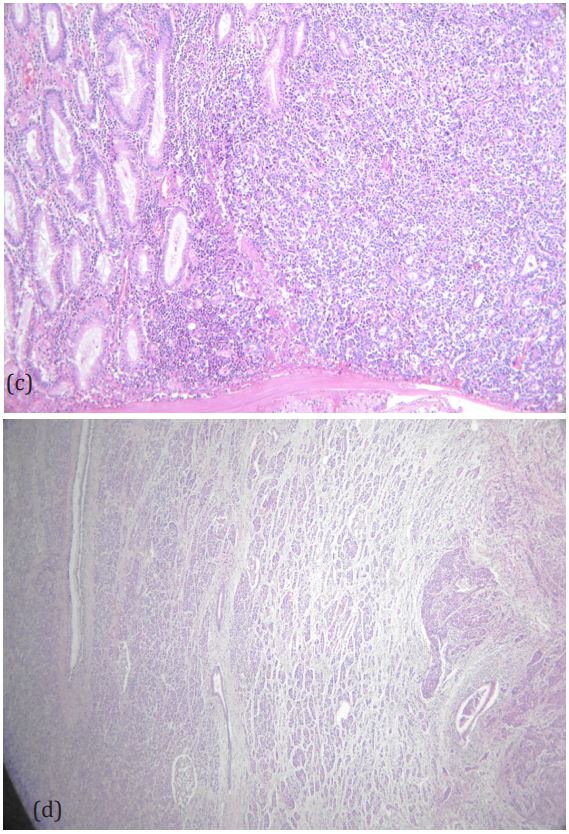
Figure 3c,d: Invasion of the gastric cancer to the transverse colon (c), pancreas (d).
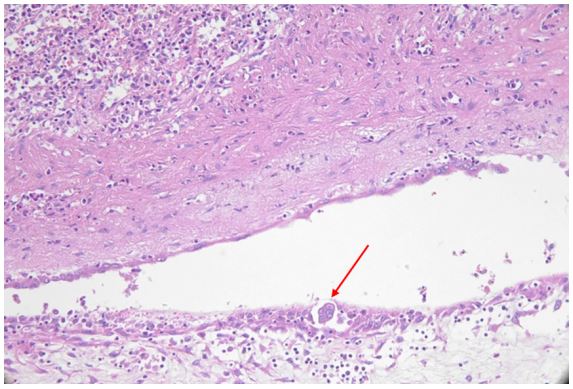
Figure 3e: Cancer in the adhesional tissue on the surface
of the spleen (red arrow).
Discussion
In approximately 10-20% of patients with GC undergoing resection, the tumor extends beyond the serosal layer into the adjacent organs[10,11,15]. Such patients require extensive en-bloc resection of the invaded organs[10,11,16-18]. Combined therapy, including perioperative chemotherapy, has been shown to achieved a favourable outcome[19,20]. However, such advanced cancers are often associated with other incurable diseases such as peritoneal, haematogenous, and/or distant lymph node metastases [9,11]. The treatment of advanced GC is particularly challenging owing to technical difficulties, severe morbidity after surgery, and poor correlation between combined resection and survival [11].
In the present case, gas was observed in the pancreatic duct, which was thought to be due to direct invasion of the pancreatic duct by gastric cancer. Because infection of the pancreatic duct was suspected, preoperative chemotherapy was not indicated, and immediate infection control through tumor resection was required. Preoperative examinations were performed promptly, and surgery was performed one week after admission. Complications such as pancreatic and anastomotic leakage are serious problems following GC surgery combined with resection of adjacent organs [21], but fortunately no postoperative complications were observed in this case, and the patient was discharged from the hospital 22 days after surgery. A subset of patients with locally advanced gastric cancer present without remote dissemination [20,22], which is believed to indicate a more favourable disease biology than regional or distant dissemination early in the disease course [6,8]. This less aggressive nature can ensure a good prognosis, and indeed the present patient is still alive without relapse 2 years after surgery. Saito et al. reported that combined resection was effective in patients without peritoneal or liver metastases when curative surgery was performed, and that the best indications for combined resection were localised tumors, irrespective of the extent of lymph node metastasis and the number of invaded organs [11]. Our case did not show any metastasis to the liver, peritoneum, or lymph nodes, which is consistent with this report. To the best of our knowledge, there have been no prior reports of pancreatic duct infections due to gastric cancer invasion. Thus, our case highlights the legitimacy of combined resection of an infected pancreas to control both cancer and infection.
Although R0 resection is an important factor in the long-term prognosis of locally advanced GC, its indications are controversial because of the technical difficulty and high complication rate, and no clear guidelines have yet been established. More cases need to be accumulated to clarify the indications for surgery in such cases.
Conclusion
Advanced gastric cancer, with extensive invasion into the adjacent organs but no distant metastasis, can be treated with en-bloc resection of the primary tumor. Even in cases of infection due to tumor invasion, a relatively good prognosis can be achieved with en-bloc tumor resection.
Declarations
Acknowledgments: The authors would like to thank Masayuki Nakano for his assistance in the pathological analyses. We would like to thank Editage (www.editage.jp) for English language editing.
Informed consent: Written informed consent was obtained from the patient for the publication of this case report and the accompanying images. A copy of the written consent form is available for review upon request to the editor-in-chief of this journal.
Ethical approval: The Ethics Committee of Kikkoman General Hospital, to which the authors belong, does not require an ethics review of case reports of medical procedures performed within the normal scope of care provided that written consent is obtained from the individual patient.
Conflict of interest statement: The authors have no conflicts of interest to declare.
Funding: The author have not received any specific grants from funding agencies in the public commercial or not-for-profit sector.
References
- H Sung, J Ferlay, RL Siegel, M Laversanne, I Soerjomataram, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021; 71(3): 209-49.
- GLOBOCAN 2020. New Global Cancer Data. 2020. https://www.uicc.org/news/globocan-2020-new-global-cancer-data.
- N Nakamura, S Kinami, J Fujita, D Kaida, Y Tomita, et al. Advanced gastric cancer with abdominal wall invasion treated with curative resection after chemotherapy: A case report. J Med Case Rep. 2021; 15(1): 230.
- DK Dhar, H Kubota, M Tachibana, S Kinugasa, R Masunaga, et al. Prognosis of T4 gastric carcinoma patients: an appraisal of aggressive surgical treatment. J Surg Oncol. 2001; 76(4): 278-82.
- A Kobayashi, T Nakagohri, M Konishi, K Inoue, S Takahashi, et al. Aggressive surgical treatment for T4 gastric cancer. J Gastrointest Surg. 2004; 8(4): 464-70.
- F Carboni, P Lepiane, R Santoro, R Lorusso, P Mancini, et al. Extended multiorgan resection for T4 gastric carcinoma: 25-year experience. J Surg Oncol. 2005; 90(2): 95-100.
- H Isozaki, N Tanaka, N Tanigawa and K Okajima. Prognostic factors in patients with advanced gastric cancer with macroscopic invasion to adjacent organs treated with radical surgery. Gastric Cancer. 2000; 3(4): 202-10.
- RC Martin, DP Jaques, MF Brennan and M Karpeh. Extended local resection for advanced gastric cancer: increased survival versus increased morbidity. Ann Surg. 2002; 236(2): 159-65.
- I Kodama, H Takamiya, K Mizutani, Ohta, K. Aoyagi, K Kofuji. Gastrectomy with combined resection of other organs for carcinoma of the stomach with invasion to adjacent organs: clinical efficacy in a retrospective study. J Am Coll Surg. 1997; 184(1): 16-22.
- D Korenaga, T Okamura, H Baba, A Saito and K Sugimachi. Results of resection of gastric cancer extending to adjacent organs. Br J Surg. 1988; 75(1): 12-5.
- H Saito, S Tsujitani, Y Maeda, K Fukuda, K Yamaguchi, et al. Combined resection of invaded organs in patients with T4 gastric carcinoma. Gastric Cancer. 2001; 4(4): 206-11.
- R A. Agha, T Franchi, C Sohrabi, G Mathew, A Kerwan, et al. The SCARE 2020 Guideline: Updating Consensus Surgical CAse REport (SCARE) Guidelines. Int J Surg. 2020; 84: 226-30.
- UIC Cancrum. TNM Classification of Malignant Tumours-8th edition. Geneva: UICC. 2016.
- JGC. Association. Japanese classification of gastric carcinoma 15th edition. Tokyo: Kanehara. 2017.
- Y. Kodama K. Sugimachi K. Soejima T. Matsusaka and K. Inokuchi. Evaluation of extensive lymph node dissection for carcinoma of the stomach. World J Surg. 1981; 5(2): 241-8.
- MH Shiu, DN Papacristou, C Kosloff, G Eliopoulos. Selection of operative procedure for adenocarcinoma of the midstomach. Twenty years’ experience with implications for future treatment strategy. Ann Surg. 1980; 192(6): 730-7.
- HW Scott, Jr RB Adkins, Jr and JL. Sawyers. Results of an aggressive surgical approach to gastric carcinoma during a twentythree-year period. Surgery. 1985; 97(1): 55-9.
- HJ Wanebo, BJ Kennedy, J Chmiel, G Steele, JrD Winchester and R Osteen. Cancer of the stomach. A patient care study by the American College of Surgeons. Ann Surg. 1993; 218(5): 583-92.
- SE Al-Batran, N Homann, C Pauligk, TO Goetze, J Meiler, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet. 2019; 393(10184): 1948-57.
- JG Aversa, LP Diggs, BL Hagerty, DA Dominguez, PHG Ituarte, et al. Multivisceral Resection for Locally Advanced Gastric Cancer. J Gastrointest Surg. 2021; 25(3): 609-22.
- F Pacelli, G Cusumano, F Rosa, D Marrelli, M Dicosmo, et al. Multivisceral resection for locally advanced gastric cancer: an Italian multicenter observational study. JAMA Surg. 2013; 148(4): 353-60.
- DG Power, MA Schattner, H Gerdes, B Brenner, AJ Markowitz, et al. Endoscopic ultrasound can improve the selection for laparoscopy in patients with localized gastric cancer. J Am Coll Surg. 2009; 208(2): 173-8.
