
Open Access, Volume 9
Epidermolysis bullosa acquisita of the oral mucosa
Hanna K Laine1,2*; Jaana Rautava1,2,3
1Department of Oral and Maxillofacial Diseases, Clinicum, University of Helsinki, Helsinki, Finland.
2Oral Pathology and Oral Radiology, Institute of Dentistry, University of Turku and Turku University Hospital, Turku, Finland.
3Department of Pathology, Medicum, Faculty of Medicine, University of Helsinki and HUS Diagnostic Center, HUSLAB, Helsinki University Hospital, Helsinki, Finland.
Hanna K Laine
Department of Oral and Maxillofacial Diseases, Faculty of Medicine, P.O. Box 41, FI-00014 University of
Helsinki, Finland.
Email: hanna.k.laine@helsinki.fi
Received : Dec 07, 2023,
Accepted : Dec 26, 2023
Published : Dec 29, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Objective: We report a case of an elderly woman with Epidermolysis Bullosa Acquisita (EBA).
Background: EBA is a chronic Autoimmune Blistering Disease (AIBD) of the skin and mucous membranes that is associated with circulating and tissue-bound autoantibodies to type VII collagen. EBA limited to the oral mucosa has been shown in 5-10% of cases. In the oral cavity, these lesions may present as single or multiple bullas, ulcers, and erosions.
Methods: A 75-year-old Finnish woman with ulceration and bulla formation of the mucous membrane of the oral cavity was referred to the Department of Oral and Maxillofacial Diseases, Turku University Hospital, Turku, Finland. The diagnosis of EBA was made with supporting clinical picture and positive direct immunofluorescence and excluding other AIBDs by serological tests and direct immunofluorescence salt split skin test.
Conclusion: The diagnosis of EBA should be kept in mind despite the rarity of this AIBD.
Keywords: Epidermolysis bullosa acquisita; Mucous membrane of oral cavity; Oral pathology; Elderly patients.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Laine HK (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Laine HK, Rautava J. Epidermolysis bullosa acquisita of the oral mucosa. Open J Clin Med Case Rep. 2023; 2178.
Introduction
Epidermolysis Bullosa Acquisita (EBA) is a rare chronic autoimmune blistering disease of the skin and mucous membranes, with an incidence of 0.2-0.5/million inhabitants/year in Europe [1,2]. The gender distribution is equal and the peak age at time of diagnosis of EBA is over 70 years [3]. However, EBA may occur at any age [3]. EBA is associated with circulating and tissue-bound autoantibodies to type VII collagen, which is the main component of the epithelium’s sublamina densa anchoring fibrils.Bulla formation in the skin and mucosa is due to the destruction of these anchoring fibrils, leading to separation of the epithelium from the underlying connective tissue [1]. Two clinical variants are described: The classical mechanobullous form and the inflammatory form [1,4]. One-third of the patients have the classical mechanobullous EBA subtype. It manifests as blisters and erosions following the friction of skin. Additionally, mucosal membranes may be affected, but this is not a prominent feature [1,2,4]. Two-thirds of EBA cases are classified as the inflammatory form [1]. The inflammatory form of EBA is subdivided into the four classes of bullous pemphigoid-like EBA, Mucous Membrane-like EBA (MM-EBA), IgA-EBA, and Brunsting-Perry-type EBA [4]. The clinical picture of the inflammatory form resembles the bullous pemphigoid and Mucous Membrane Pemphigoid (MMP), and mucosal lesions are present in approximately half of the cases. Mucosal involvement is part of the clinical picture in 60% of both types of EBA at some point of the disease [1]. However, only 5-10% have predominantly mucosal lesions as opposed to skin lesions [1]. In the oral cavity, these lesions may manifest as single or multiple bullas, ulcers, and/or erosions. Here, we present a patient case of an older individual with EBA limited to the Mucous Membranes of the Oral Cavity (MMOC).
Case Presentation
A 75-year-old Finnish woman was referred to the Department of Oral and Maxillofacial Diseases, Turku University Hospital, Turku, Finland for ulceration and bulla formation of the MMOC. The bullous symptoms had persisted for 18 months. The patient suffered from pain and difficulties with eating and maintaining oral hygiene. Additionally, the patient had had an itching rash on the skin for several months. The patient had glaucoma and hypercholesterolemia. Her medication comprised simvastatin (Simvastatin®), latanoprost (Monoprost®), and acetylsalicylic acid (Primaspan®). The patient was a non-smoker and alcohol consumption was modest. The oral examination revealed ulcers and bullous lesions on the patient’s gingiva and cheek mucosa (Figure 1). Nikolsky’s sign test result on oral mucosa was slightly negative. The patient´s oral hygiene was poor. She had gingivitis with calculus formation, but periodontal pockets >3 mm were not detected. She had a shortened dental arch (missing teeth 13, 15, 18, 22, 24-28, 38, and 45-48). The patient did not have a prosthesis. Clinical view was suggestive for immunobullous disease in addition to traditional gingivitis due to difficulties in maintaining oral hygiene. Dermatological physical examination did not reveal any skin lesions. Two biopsies from the buccal mucosa were taken, one for histopathological examination and the other for immunofluorescence. Additionally, a skin biopsy from the elbow was taken for immunofluorescence examination. The histopathological analysis of the oral cavity specimen revealed hyperkeratotic and hyperplastic stratified epithelium and subepithelial bulla formation. Lamina propria showed inflammation consisting predominantly of lymphocytes. The Direct Immunofluorescence (DIF) examination from oral mucosa showed linear positivity for Immunoglobulin (Ig) G and C3 in the basal membrane and was negative for IgA and IgM. DIF examination of perilesional skin was positive for IgG, IgA, and C3 in the basement membrane of the epidermis. Salt split skin test was positive and showed IgG and C3 linear positive reaction on the dermal side of the bulla (Figure 2). Thorough laboratory examinations consisted of complete blood count, alanine aminotransferase, creatine, and celiac disease blood tests. Laboratory tests showed normal complete blood count evaluation, alanine aminotransferase and creatine within normal limits, and negative celiac disease blood tests. Indirect Immunofluorescence (IIF) examination showed negative circulating skin anti-desmosomal antibodies and anti-skin basement membrane antibody excluding pemphigus and pemphigoid. Additionally, desmosomal glycoproteins, such as desmoglein 1 and 3, and bullous pemphigoid-230 and laminin 332 were negative. Interestingly, the test result was also negative for type VII collagen. The patient was diagnosed with EBA by a multidisciplinary group of medical specialists at Turku University Hospital. For the treatment, Triamcinolone acetonide 0.1% mouthwash (Triamcinolone acetonide 0.1% with methyl parahydroxybenzoate 0.1 mg/ml) was prescribed. The dosage of medication was a 10 ml rinse twice a day for 10 days. In addition, the patient was referred to her own dentist for anti-inflammatory treatment of the gingiva and restorative treatment of dentition. Triamcinolone acetonide 0.1% treatment was found to be beneficial for the symptoms for three months, but lacked a good response for the clinical lesions. The medication was altered to glucocorticoid cream (Dermovat®) with instructions to apply on the lesion area twice a day for 14 days. This treatment was successful in relieving bulla formation and other symptoms (Figure 1). There were no skin lesions or symptoms to treat at this point. Follow-up visits were arranged every six months.
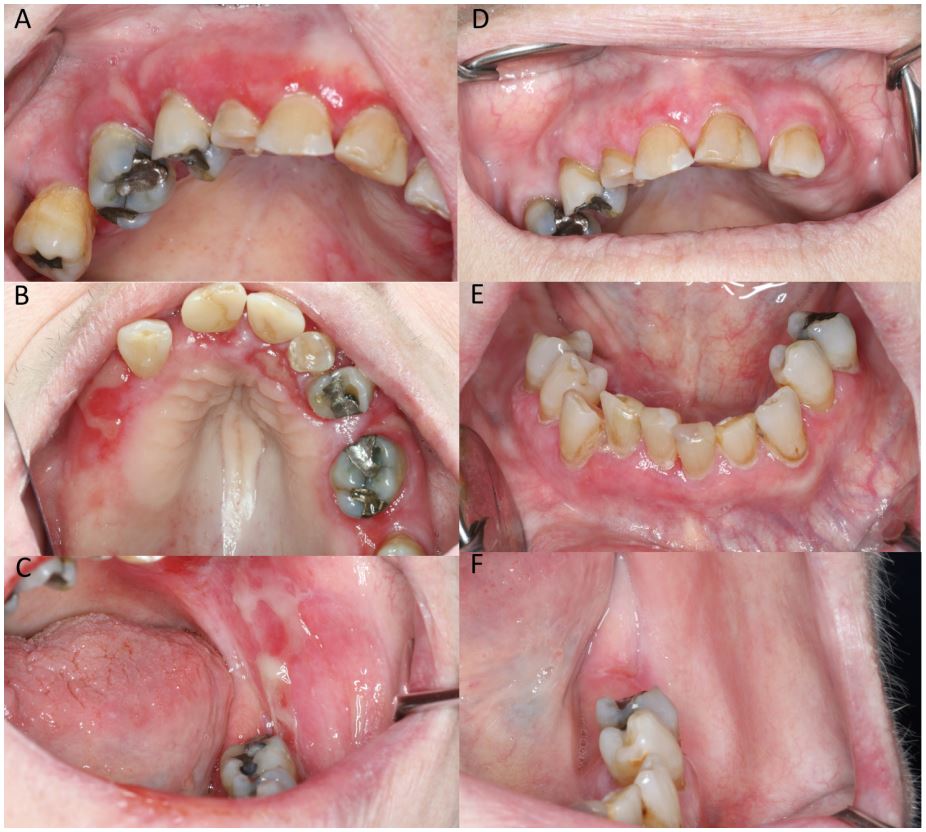
Figure 1: (A-C) Blistering and ulceration of mucous membranes of the oral cavity at the first visit. (D-F)
The mucous membranes after successful treatment.
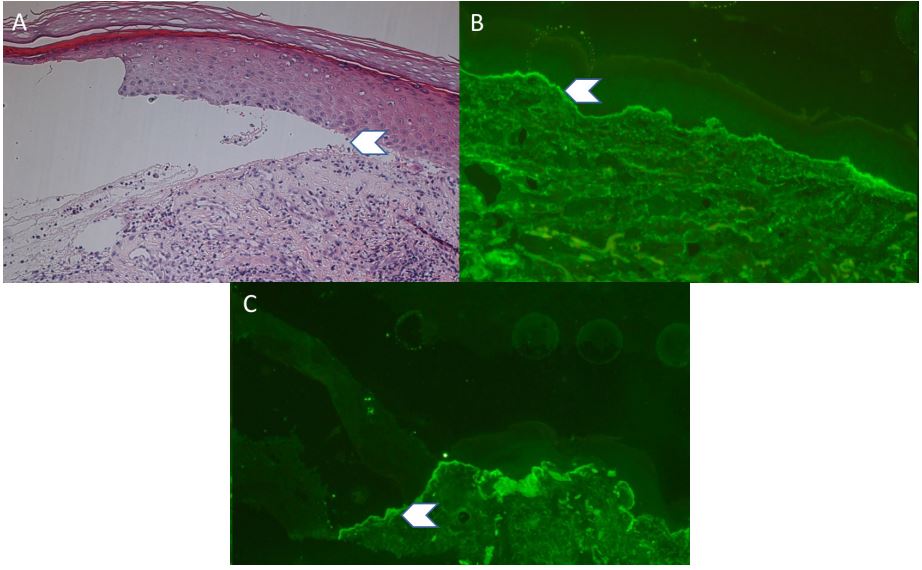
Figure 2: (A) Histology of the skin biopsy showing subepidermal blister formation and chronic inflammatory cells in the dermis (arrow). (B&C) Direct immunofluorescence examination of the skin. B, Immunoglobulin G immunodeposits in the basement membrane of the skin (arrow). (C) Immunoglobulin G
immunodeposits on the dermal side of the bulla in the salt split skin test (arrow). Magnification A-C x200.
Discussion
EBA is a rare autoimmune bullous disease, and cases limited to the oral cavity account for only 5-10% [1]. EBA has two separate clinical variants: the classical mechanobullous form and the inflammatory form [4]. Our patient case presents MM-EBA of the inflammatory form, manifesting multiple blisters and erosions exceptionally only in the MMOC. Other forms of EBA have predominantly skin lesions. However, MM-EBA patients could have lesions in MMOC, pharynx, esophagus, epiglottis, conjunctiva, genitalia, anus, and bronchi [4,5]. To our knowledge, this is the first case report of EBA presenting exclusively blisters and ulceration in the MMOC. Recently, criteria for diagnosing EBA have been updated by the International Bullous Diseases Group [4]. The criteria include (1) clinical picture supporting bullous disorder, (2) detection of subepidermal or subepithelial blister by histology, (3) positive DIF microscopy of perilesional skin or mucous membrane with linear IgG, C3, IgA, and/or IgM deposits in the basement membrane area, and (4) positive serological test to confirm serum autoantibodies against type VII collagen. Sometimes a patient lacks detectable levels of circulating autoantibodies and serological confirmation is not possible. New sophisticated tests, such as u-serration pattern analysis by DIF, direct immunoelectron microscopy demonstration of immunodeposits within anchoring fibrils in the dermoepidermal junction zone, and in vivo bound immunodeposits in the basement membrane by fluorescence overlay antigen mapping technique, give convincing test results. Unfortunately, these examinations are not routinely available in every laboratory [4,5]. If serology is not available for the diagnosis, besides definite clinical picture and positive DIF, the salt split skin test should support EBA [4]. In the method, a perilesional skin sample is incubated in a concentrated salt solution that separates the epithelium from the connective tissue. DIF and IIF examinations then show deposition of IgG autoantibodies against type VII collagen on the floor of the bulla (u-shape). This is in contrast to bullous pemphigoid, MMP, and linear IgA diseases in which the positive immunofluorescence pattern is on the roof of the bulla (n-shape) [6]. However, in anti-laminin 332 MMP and anti-p200 pemphigoid, autoantibodies bind to the dermal side in the salt split skin test [7,5]. In our case, the multidisciplinary team made the diagnosis of EBA according to the clinical and histological picture and positive DIF and salt split skin test (Figures 1 and 2). Laminin 332 was negative by serology, excluding anti-laminin 332 MMP. EBA and anti-p200 pemphigoid patients may present similarities in clinical picture, but anti-p200 pemphigoid limited to mucosal lesions has not been described in the literature [5,8]. Although laboratory testing to rule out anti-p200 pemphigoid was not performed, the clinical picture in our patient case supports the diagnosis of EBA. Serology alone may be convincing enough to establish an EBA diagnosis [4]. However, in the serologic tests detectable circulating autoantibodies and even misdiagnosis are possible in 50% of cases [8,9-11]. In our case, according to the serology collagen type VII was negative, but the salt split skin test and the clinical picture support EBA. Due to the rarity of EBA, there is a lack of randomized controlled trials on the treatment modalities. The golden standard in treatment for disease control of autoimmune diseases is systemic and local corticosteroids [12-14]. Other reported options are steroid-sparing agents such as colchicine, diaminodiphenyl sulfone, methotrexate, azathioprine, cyclosporine, mycophenolate mofetil, and cyclophosphamide [2,14]. In our case, the patient benefitted from local corticosteroids, although how EBA will behave in the future and will it spread remain unknown. Good oral hygiene and health are mandatory for healing of MMOC with any autoimmune bullous disease [9]. Infection and immune dysregulation may play a role in chronic inflammatory condition, and they may share common pathophysiological processes [15]. In psoriasis patients, for instance, maintaining good oral health helps to control their disease [15]. In our patient, the combination of professional antiinflammatory treatment and topical corticosteroid use led to good mucosal response.
Conflict of interest: The authors have no conflicts of interest to declare.
Author contributions: HL and JR participated in treating the patient, designed the case report, wrote and edited the manuscript, and approved the final version of the manuscript.
References
- Vorobyev A, Ludwig RJ, Schmidt E. Clinical features and diagnosis of epidermolysis bullosa acquisita. Expert Rev Clin Immunol. 2017; 13: 157-169.
- Koga H, Prost Squarcioni C, Iwata H, Jonkman MF, Ludwig RJ, et al. Epidermolysis bullosa acquisita: The 2019 update. Front Med (Lausanne). 2019; 5: 362.
- Hubner F, Recke A, Zillikens D, Linder R, Schmidt E. Prevalence and age distribution of pemphigus and pemphigoid diseases in Germany. J Invest Dermatol. 2016; 136: 2495-2498.
- Prost Squarcioni C, Caux F, Schmidt E, et al. International bullous diseases group: Consensus on diagnostic criteria for epidermolysis bullosa acquisita. Br J Dermatol. 2018; 179: 30-41.
- Kridin K, Ahmed AR. Anti-p200 pemphigoid: A systematic review. Front Immunol. 2019; 10: 2466.
- Kridin K, Kneiber D, Kowalski EH, Valdebran M, Amber KT. Epidermolysis bullosa acquisita: A comprehensive review. Autoimmun Rev. 2019; 18: 786-795.
- Chiorean R, Danescu S, Virtic O, et al. Molecular diagnosis of anti-laminin 332 (epiligrin) mucous membrane pemphigoid. Orphanet J Rare Dis. 2018; 13: 111.
- Meijer JM, Diercks GF, Schmidt E, Pas HH, Jonkman MF. Laboratory diagnosis and clinical profile of anti-p200 pemphigoid. JAMA Dermatol. 2016; 152: 897-904.
- Carey B, Setterfield J. Mucous membrane pemphigoid and oral blistering diseases. Clin Exp Dermatol. 2019; 44: 732-739.
- Buijsrogge JJ, Diercks GF, Pas HH, Jonkman MF. The many faces of epidermolysis bullosa acquisita after serration pattern analysis by direct immunofluorescence microscopy. Br J Dermatol. 2011; 165: 92-98.
- Terra JB, Jonkman MF, Diercks GF, Pas HH. Low sensitivity of type VII collagen enzyme-linked immunosorbent assay in epidermolysis bullosa acquisita: Serration pattern analysis on skin biopsy is required for diagnosis. Br J Dermatol. 2013; 169: 164-167.
- Kim JH, Kim YH, Kim SC. Epidermolysis bullosa acquisita: A retrospective clinical analysis of 30 cases. Acta Derm Venereol. 2011; 91: 307-312.
- Kim JH, Kim SC. Epidermolysis bullosa acquisita. J Eur Acad Dermatol Venereol. 2013; 27: 1204-1213.
- Iwata H, Vorobyev A, Koga H, et al. Meta-analysis of the clinical and immunopathological characteristics and treatment outcomes in epidermolysis bullosa acquisita patients. Orphanet J Rare Dis. 2018; 13: 153.
- Qiao P, Shi Q, Zhang R, et al. Psoriasis patients suffer from worse periodontal status-A meta-analysis. Front Med (Lausanne). 2019; 6: 212.
