
Open Access, Volume 9
Treatment of Crohn’s disease with complex fistula disease using an exclusion diet
Doortje Dirks1*; Benjamin Misselwitz2; Manfred Essig3
1Resident Internal Medicine, Medical Clinic, Hospital Thun, Switzerland.
2Prof. Dr. med. Consultant Gastroenterology, Department of Visceral Surgery and Medicine, Inselspital Bern and Bern University, Switzerland.
3Prof. Dr. med. Clinic Director and Chief Physician, General Internal Medicine, and Gastroenterology Tiefenau Hospital Bern, Switzerland.
Doortje Dirks
Resident Internal Medicine, Medical Clinic, Hospital Thun, Switzerland.
Email: Doortjedirks@me.com
Received : Dec 05, 2023,
Accepted : Dec 22, 2023
Published : Dec 29, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Exclusive Enteral Nutrition (EEN) is considered the standard of care for the treatment of children with Crohns Disease (CD) but it is rarely used in adults. The main reason for this might be severe dietary restrictions, resulting in a reduced quality of life and a lack of compliance with the diet. The development of less restrictive dietary strategies has improved therapy adherence and thus also the success of the therapy in recent years. The therapy of fistulas in CD is generally considered difficult and nutritional therapy for fistulas has not been systematically investigated. We present the case of a patient with fistulizing CD. Immunosuppressive therapy with a biological was complicated by urothelial carcinoma, and an alternative treatment had to be found. In our patient, Crohns Disease Exclusion Diet (CDED) and Partial Enteral Nutrition (PEN) resulted in normal stool consistency and frequency, and one and a half years after the start of the exclusion diet, the patient remains in clinical remission.
Keywords: Crohns disease; Complex fistula disease; Exclusion diet.
Abbreviations: BCG: Bacillus Calmette Guérin; CD: Crohns disease; CDAI: Crohn’s disease activity index; CDED: Crohns disease exclusion diet; DMARD: Disease modifying antirheumatic drugs; EEN: Exclusive enteral nutrition; PEN: Partial enteral nutrition; TNF: Tumor necrosis factor; TURB: Transurethral resection of the urinary bladder.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Dirks D (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Dirks D, Misselwitz B, Essig M. Treatment of Crohn’s disease with complex fistula disease using an exclusion diet. Open J Clin Med Case Rep. 2023; 2177.
Introduction
Fistulas in various locations of the gastrointestinal tract occur frequently in CD and are difficult to treat. Close cooperation between surgeons and gastroenterologist is essential for a successful treatment. The Tumor Necrosis Factor (TNF) inhibitor infliximab is considered the first-line therapy for fistulizing CD [1]. In case of intolerance or failure of this therapy, adalimumab, vedolizumab, ustekinumab, or stem cell therapy with Alofisel® can be considered. Nutritional therapies for CD including EEN, half-elemental diet and CDED + PEN are emerging treatment option for CD. These therapies are highly efficient and well tolerated and have long been used in the therapy of pediatric CD [2]. However, all nutritional therapies, especially EEN are less palatable, and the required dietary restrictions can reduce the quality of life. For these reasons, it has so far been underused in adults [3,4]. CD is a chronic inflammatory condition and a wide range of manifestations and complications. For instance, CD is also a known risk factor for urolithiasis, experienced by our patient due to loss of bile acid and increased absorption of oxalate. Male gender, disease activity and intestinal surgery could be identified as risk factors in a Swiss study, fitting to our patient [5]. Comorbidities, including malignant disease, can limit treatment options in CD. Our understanding regarding the effect of biologicals and immunosuppressant’s on co-existing malignant disease is limited. Most data are mainly derived from rheumatologically studies, due to a high number of patients and long treatment experience for this indication [6-8]. Unfortunately, in almost all studies on Disease-Modifying Antirheumatic Drugs (DMARDs), malignant disease has been an exclusion criterion. In a British and German study with registry data of patients with DMARD-treated rheumatoid arthritis, no increased incidences of malignancies could be found [7,8]. However, data from randomized, placebo-controlled trials are lacking. Current guidelines advise against therapy with biologicals in the presence of malignant disease and an observation period after curative anti-cancer therapy is advised before starting biologicals [6].
Case Presentation
In 2017, a gentleman in his fifties presents to our unit for the management of fistulizing CD. Past medical history is remarkable for a partial small intestinal resection in his twenties, with the macroscopic and histological diagnosis of CD. Due to a mild course of CD, the patient has remained without medical therapy for many years. Unfortunately, there are no preliminary reports from this time, including endoscopies. In 2017, the patient becomes increasingly symptomatic with complex perianal, perirectal, and transsphincteric fistulas. From April to August 2017, the fistulas are drained surgically several times, and Setons are inserted. A colonoscopy in September 2017 showed several fibrin-covered ulcerations and an impassable inflammatory stenosis in the area of the ileocolostomy. In November 2017, immunosuppressive therapy with infliximab (Remicade®) at 400 mg (4 mg/kg body weight) is started with the second dose after 2 weeks, the third after 4 weeks, and then every 2 months [1]. Following our guidance, the patient stopped his long-standing smoking habit in 2019 [9]. After 1 year of infliximab treatment, anti-drug antibodies are detected (Figure 1A), and the therapy is switched to adalimumab (Humira®) [10]. However, due to more pain and secretion from the fistulae, the therapy is switched back to infliximab (Inflectra®) starting with 500 mg (5 mg/kg body weight) at weeks 0, 2, and then every 6 weeks. Low trough levels (0.6 µg/ ml) prompt an increase in dosage at a shorter interval (800 mg, 8 mg/kg body weight every 4 weeks). Because the patient remains symptomatic with purulent secretions from the fistulas, 100 mg/d azathioprine (Imurek®) is added to the therapeutic regimen in December 2019 [11]. Three months later, in March 2020, sigmoidoscopy shows no macroscopic signs of inflammation in the sigmoideum, a mild edematous proctitis and slightly reddened pseudo-polypoid elevations at the anocutaneous line, without recognizable fistula openings. Infliximab trough levels are now in the supratherapeutic range (20 µg/ml) with no detectable anti-drug antibodies. Fistula activity made surgical drainage and Seton insertion necessary in March and May 2020 (Figures 2A + B with pelvic MRI 04/2020). In September 2020, the patient develops Escherichia coli bacteremia and herpes zoster reactivation (shingles) and azathioprine is stopped. In the following 14 months, the patient remains in clinical remission, with continuing subtherapeutic infliximab levels (Figure 1A+B). In December 2021, the patient develops left-sided renal colic and a CT scan reveals urolithiasis and urinary outflow obstruction, and a double J stent catheter is inserted. In January 2022, cystoscopy with flushing cytology leads to the diagnosis of urothelial carcinoma, which is surgically removed by Transurethral Resection of the Urinary Bladder (TURB). Immunosuppression with infliximab is stopped before the operation. In February 2022, a follow-up resection is performed for stage T1 disease. Adjuvant therapy with Bacillus Calmette-Guérin (BCG) installations is started in March 2022 with plans to continue the therapy for 1-3 years. To avoid interferences with the adjuvant BCG immunotherapy, infliximab is not restarted and we decided against the use of other immunosuppressive therapeutic options. A colonoscopy in March 2022 shows a macroscopic (neo) terminal ileitis with evidence of multiple elongated fibrinous ulcerations in the distal 10 cm of the neoterminal ileum and substenosis in the area of the inflamed ileo-colostomy. Perianal Fistula orifices are visible in distal rectum and proximal anal canal inactive at time of examination (Figures 3A+B). Clinical the patient was still in remission. In April 2022, we start CDED with PEN using a nutritional formula (Modulen®) [12-14]. The patient has been able to integrate the diet well into his daily routine. In October 2023, at the time of writing, 18 months after the start of CDED and PEN, he reports normal stool consistency and frequency with two daily bowel movements. The fistulas continue to secrete blood and pus, but without pain or the need for antibiotics. Surgery and antibiotic treatment for fistulas had last been necessary in June 2022, respectively. CD remission under CDED with PEN was confirmed by a low CRP value (6-11 mg/L, normal range <5 mg/ L, see Figure 1A). Similarly, the Crohn’s Disease Activity Index (CDAI) is at 20 points (Figure 1A), indicating persistent clinical remission. A control endoscopy has not yet taken place.
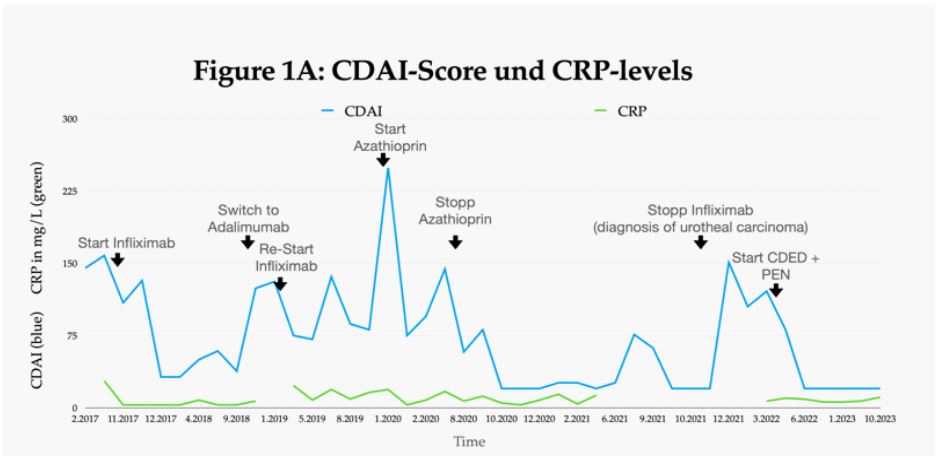
Figure 1A: CDAI-Score and CRP-levels from 02/2017-05/2023 (black arrows Treatment-Changes)
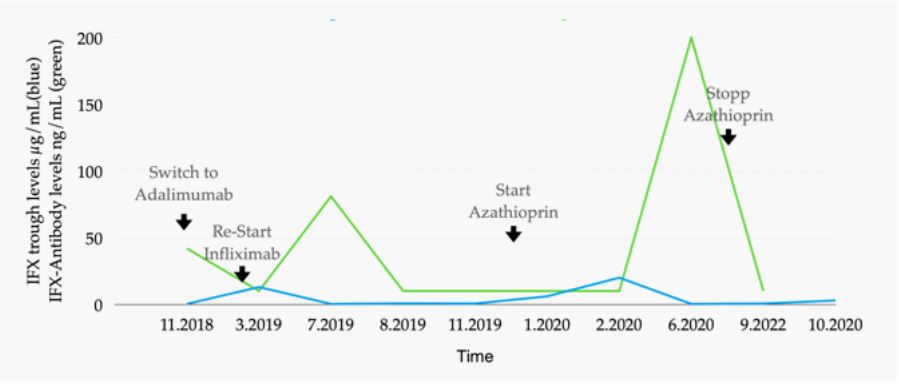
Figure 1B: Infliximab trough-levels and Infliximab antibodies from 11/2028 to 10/2020
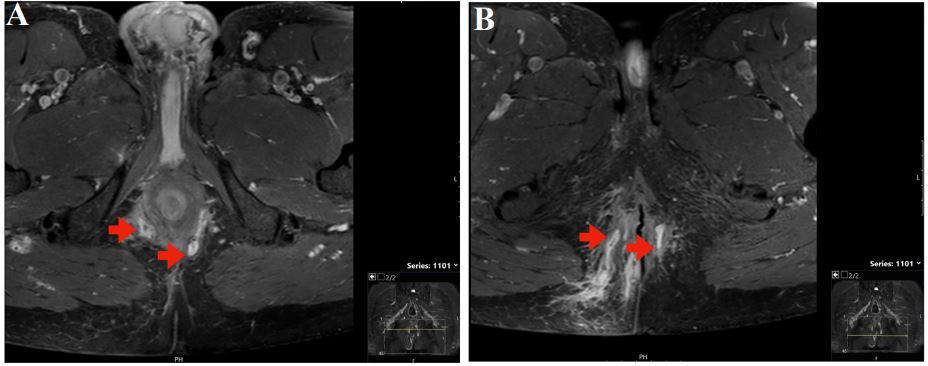
Figure 2A+B: Perianal fistulas (red arrows) in MRI of the pelvis in 04/2020.
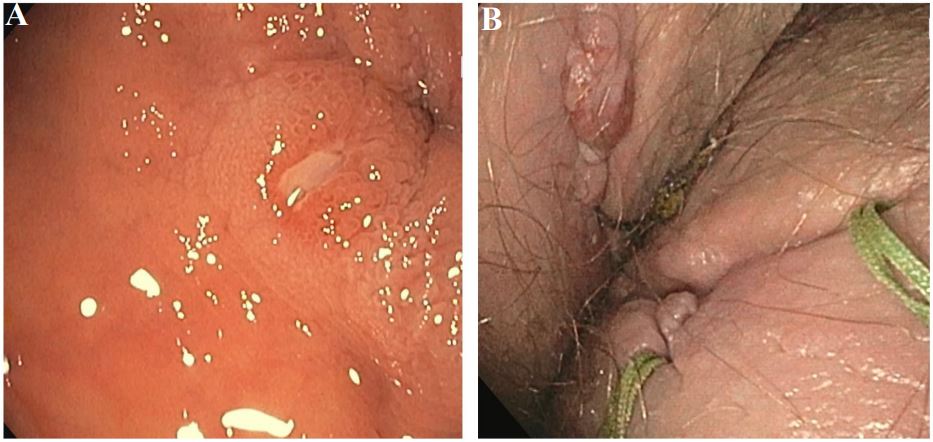
Figure 3: Colonoscopy 03/2022. (A) Fistula entrance endoluminal. (B) Fistula exits with sentons.
Nutritional therapy for Crohn’s disease
As early as 1973, Voitk et al. found that enteral nutrition had a positive effect on the activity of Crohn’s disease. Enteral nutrition had initially been started to improve the nutrition of patients before planned surgery; however, with nutritional therapy, Crohn’s disease often improved so much that surgery was no longer deemed necessary [15]. In current clinical practice for CD, nutritional therapy can either be provided by EEN, half-elemental nutrition, or less restrictive CDED + PEN. EEN is a nutritional therapy with abstention from all food intake except for a special nutritional drinking powder that is taken orally or administered via a nasogastric tube for 6-12 weeks. After that, a non-restrictive diet is reintroduced, often with a transitional phase of a few weeks of partial enteral nutrition and a free oral diet [2,3,16]. In half-elemental nutrition, 50% of the calories are provided by the powdered drink. The other half may be consumed as a regular meal. This therapy can be used as a maintenance therapy for CD [18]. CDED + PEN is a feasible nutritional therapy for CD and supporting online tools are available [12-14]. In CDED, there are compulsory foods, accepted foods, and forbidden foods that must not be consumed. A defined fraction of the calories is covered by a nutritional formula designed for the treatment of CD (Modulen®). CDED consists of a 3-phase program:
In phase 1 (weeks 1-6), 50% of the daily diet is covered by nutrition powder (Modulen). Compulsory foods are chicken breast, egg, banana, apple, and potato. Additionally accepted foods are white rice and selected fruits and vegetables.
In phase 2 (weeks 7-12), the rules are relaxed. Now only 25% of the daily calorie requirement must be covered by the nutritional formula. All compulsory foods and permitted foods from the 1st phase remain, but the list of permitted foods is considerably expanded.
The 3rd phase (after week 12) is the maintenance phase, which should be extended by the patient for as long as possible. Nutritional restrictions are now further lifted: There are no compulsory, only recommended dishes, and the list of permitted foods is even further expanded. Only 25% of calories are covered by Modulen®. Moreover, on 1-2 days of each week, no nutritional limitations apply [14].
Discussion
Several studies support the efficacy of nutritional therapy for CD: In a Meta-analysis from 2007 Dziechciarz et al analysed 11 RCT’s and found similar efficacy for EEN and corticosteroids in the therapy of children with CD [2]. A review article from Mitrev et al published in 2021 could identify 79 studies about EEN in adult CD patients. In their results, nutritional therapy could improve clinical, biomarker, endoscopic and radiologic measures of disease activity. It was also beneficial for adult patients with fistulas and strictures with potential avoidance of surgery. In comparison to corticosteroids, they found the latter to be potentially more effective as induction therapy, but EEN superior in mucosal healing beyond clinical remission [3]. CDED + PEN resulted in similar corticosteroid-free remission rates (75% vs. 59% with EEN) and higher compliance to the therapy regime (97.5% vs. EEN 73.6%) [12,13]. A long-term randomizedcontrolled study from Japan compared half-elemental nutrition to an unrestricted diet in 51 patients (mean age 28.9-30.8 years) with Crohn’s disease. The study was stopped prematurely after 2 years due to the significantly lower relapse rates for the half-elemental diet (34.6% vs. 64.0% with free diet) [18]. Fistulas are a typical manifestation of CD, which can be difficult to treat. Considering that only limited data on nutritional therapy for adult patients with CD are available, [3,4,13,16], it is not surprising that data regarding nutritional therapy in adult patients with fistula disease are scarce [17,19-22]. In 1990, an english study included 12 patients with perianal fistula in a trial with EEN for 8 weeks. In this study, nine patients achieved clinical remission but eight relapsed after going back to normal food [19]. For CD nutritional treatment of adults with fistulizing CD, we identified four case series [17]. In the first 33 patients with entero-cutaneus or entero-enteric fistulas complicated by abscesses were included, 43% also having perianal disease. After 12 weeks of EEN (completed by 31 patients), 27 achieved full remission. Patients with entero-cutaneous fistulas had a closure rate of 75%. How the perianal lesions responded to therapy was not described. The second included 48 patients with entero-cutaneous fistulas. They were also treated with 12 weeks EEN. In 62.5% of patients, fistula closure could be observed. Another prospective, Chinese study from 2018 included 29 adult CD patients. The patients received long-term oral EEN. Seven of these patients also had perianal disease. The authors describe a «turn for the better» in six of those patients with the remaining patient needing additional treatment for an unclosed fistula [20]. Moreover, a small Indian study from 2019 treated six adult patients with CD and non-response to anti-TNF therapy with EEN for 12 weeks. Two of these patients had perianal fistulas for which drainage could be reduced by 50% at week 8 but no remission could be achieved at 12 weeks. Two patients with entero-enteric fistulas had complete healing after 12 weeks, objectified by MR-enterography [21]. Finally, a New Zealand pilot study of EEN and PEN in young adult CD patients reported favorable results for three patients with perianal fistulas. However, no detailed information on the outcome of these patients was provided [22].
Conclusion
Treatment of CD continuous to pose challenges for some patients. For instance, the long disease course of CD makes comorbidity likely, which further limits therapeutic options. In our case, long-term smoking resulted in the development of an urothelial carcinoma and the need for BCG therapy for which immunosuppression is considered a contraindication. Fortunately, in our patient lasting clinical and biochemical remission of fistulizing Crohn’s disease could be achieved with nutritional therapy alone without immunosuppressive therapy. Concepts for nutritional therapy in CD have been developed during the last 50 years, but despite good data from pediatric patients, it is only rarely used in adults. Despite some efforts, the mode of action of nutritional therapies is unknown, which remains a limitation. New more open diet models, such as the CDED + PEN, lifted some restrictions in all phases of the therapy. Further research in this area should aim to make diet regimes to be even simpler since fewer restrictions would increase compliance with therapy, especially in adults. Thus, nutritional therapy could become a feasible and commonly used component of CD treatment, either as monotherapy or as an adjunct to biologicals or immunosuppression.
Competing interests: BM has received research grants from BMS, Nestle, MSD. He has served on an advisory board and/or received speaking fees and/or traveling fees from Falk, Abbvie, iQONE, Takeda, BMS, Gilead, Takeda and MSD. The other authors have no conflict of interest to declare.
References
- Present DH, Rutgeerts P, Targan S, Hanauer SB, Mayer L, et al. Infliximab for the treatment of fistulas in patients with Crohn’s disease. PMID: 10228190.
- Dziechciarz P, Horvath A, Shamir R, Szajewska H. Meta-analysis: Enteral nutrition in active Crohn’s disease in children. PMID: 17767463.
- Mitrev N, Huang H, Hannah B, Kariyawasam VC. Review of exclusive enteral therapy in adult Crohn!s disease. PMID: 34580154.
- De Sire R, Nardone OM, Testa A, Calabrese G, Caiazzo A, et al. Exclusive Enteral Nutrition in Adult Crohn’s Disease: an Overview of Clinical Practice and Perceived Barriers. PMID: 35002274.
- Fagagnini S, Heinrich H, Rossel JB, Biedermann L, Frei P, et al. Risk factors for gallstones and kidney stones in a cohort of patients with inflammatory bowel diseases. PMID: 29023532.
- Schmalzing M, Strangfeld A, Tony HP. Medikamentöse Therapie der rheumatoiden Arthritis bei Malignomanamnese. DOI: 10.1007/s00393-015-0034-6.
- Dixon WG, Watson KD, Lunt M, Mercer LK. British Society For Rheumatology Biologics Register Control Centre Consortium, Hyrich KL, and Symmons DPM: Influence of anti-tumor necrosis factor therapy on cancer incidence in patients with rheumatoid arthritis who have had a prior malignancy: Results from the British Society for Rheumatology Biologics Register. PMID 20535785.
- Strangfeld A, Hierse F, Rau R, Burmester GR, Krummel-Lorenz B, et al. Risk of incident or recurrent malignancies among patients with rheumatoid arthritis exposed to biologic therapy in the German biologics register. RABBIT PMID: 20064207.
- Birrenbach T, Böcker U. Inflammatory bowel disease and smoking: A review of epidemiology, pathophysiology, and therapeutic implications. PMID: 15626903.
- Colombel JF, Sandborn WJ, Rutgeerts P, Enns R, Hanauer SB, et al. Adalimumab for Maintenance of Clinical Response and Remission in Patients With Crohn!s Disease: The CHARM Trial PMID 17241859.
- Colombel JF, Sandborn WJ, Reinisch W, Matzaris GJ, Kornbluth A, et al. for the SONIC Study Group: Infliximab, Azathioprine, or Combination Therapy for Crohn’s Disease. PMID: 30267864.
- Levine A, Wine E, Assa A, Boneh RS, Shaoul R, et al. Crohn´s Disease Exclusion Diet Plus Partial Enteral Nutrition Induces Sustained Remission in a Randomized Controlled Trial. PMID 31170412.
- Yanai H, Levine A, Hirsch A, Boneh RS, Kopylov U, et al. The crohn`s disease exclusion diet for induction and maintenance of remission in adults with mild-to-moderate Crohn`s disease (CDED-AD) an open label, pilot, randomized trial. PMID 34739863.
- Modu Life, Nestle Health Science. https://mymodulife.com/experts/
- Voitk J, Echave V, Feller JH, Brown RA, Gurd FN. Experience with elemental diet in the treatment of inflammatory bowel disease. Is this primary therapy?. PMID: 4198183.
- Hansen T, Duerksen DR. Enteral Nutrition in the Management of Pediatric and Adult Crohn!s Disease. PMID: 29701656.
- Adamji M, Day AS. An overview of the role of exclusive enteral nutrition for complicated Crohn!s disease. PMID: 30508476.
- Takagi S, Utsunomiya K, Kuriyama S, Yokoyama H, Takahashi S, et al. Effectiveness of an “half elemental diet! #as maintenance therapy for Crohn’s disease: A randomized-controlled trial. PMID: 17059514.
- Teahon K, Bjarnason I, Pearson M, Levi AJ. Ten years’ experience with an elemental diet in the management of Crohn’s disease. PMID: 2083858.
- Chen JM, He LW, Yan T, Guo XF, Hu PJ, et al. Oral exclusive enteral nutrition induces mucosal and transmural healing in patients with Crohn’s disease. PMID: 31217981.
- Sood A, Singh A, Sudhakar R, Midha V, Mahajan R, et al. Exclusive enteral nutrition for induction of remission in anti-tumor necrosis factor refractory adult Crohn!s disease: The Indian experience. PMID: 32092799.
- Wall CL, Gearry RB, Day AS. Treatment of Active Crohn’s Disease with Exclusive and Partial Enteral Nutrition: A Pilot Study in Adults. PMID: 30221149.
