
Open Access, Volume 9
Focal hepatic hot spot sign: Clinical image
Meryem Benmoussa*; Amine Naggar; Omar El Aoufir; Fatima Zohra El Amrani; Laila Jroundi
Radiology Department, Ibn Sina Hospital, Morocco.
Meryem Benmoussa
Radiology Department, Ibn Sina Hospital, Morocco.
Tel: +212659209483;
Email: benmoussa.mer93@gmail.com
Received : Dec 01, 2023,
Accepted : Dec 21, 2023
Published : Dec 29, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Benmoussa M (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Benmoussa M, Naggar A, El Aoufir O, El Amrani FZ, Jroundi L. Focal hepatic hot spot sign. Open J Clin Med Case Rep. 2023; 2176.
Description
A 51‐year‐old women was hospitalized to start chemotherapy for small cell lung cancer diagnosed one months earlier. She underwent Computed Tomography (CT) of the chest and abdomen to re‐evaluate the progression of the lung tumour. Contrast-enhanced CT of the chest indicated an invasive anterior left lung tumour that caused an obstruction of the Superior Vena Cava (SVC) (Figure 1). Contrast-enhanced CT of the abdomen revealed an intense focal wedge-shaped homogeneous enhancement area in the quadrate lobe of the liver, which is known as the hot spot sign (Figure 2). Focal hepatic hot spot sign was first described by Ishikawa in 1983. The sign can be observed on technetium 99m (99mTc) Sulphur colloid scans or on contrast, material enhanced CT scans [1]. Hot spot sign is caused by portosystemic venous shunting between the superior vena cava and the left portal vein via the internal mammary and paraumbilical veins along the ligamentum teres, secondary to superior vena cava obstruction. The hot spot is created by areas of focally increased blood flow that result from this shunting [2]. Stanford and colleagues classified SVC syndrome into four types - type I and type II referred as supra-azygous partial and near complete obstruction of SVC with antegrade flow in azygous vein. Type III is defined as complete obstruction of SVC with reversal of azygous blood flow and type IV as complete obstruction of SVC and azygous system with development of chest wall collaterals [3]. This sign has been reported in Budd-Chiari syndrome, the causes of SVC syndrome (neoplasms of the thorax as lung carcinoma and lymphoma, Vasculo‐Behcet’s disease, fibrosing mediastinitis, and luetic aneurysm), and masses of the liver (abscess, haemangioma, focal nodular hyperplasia, and hepatocellular carcinoma) [4].
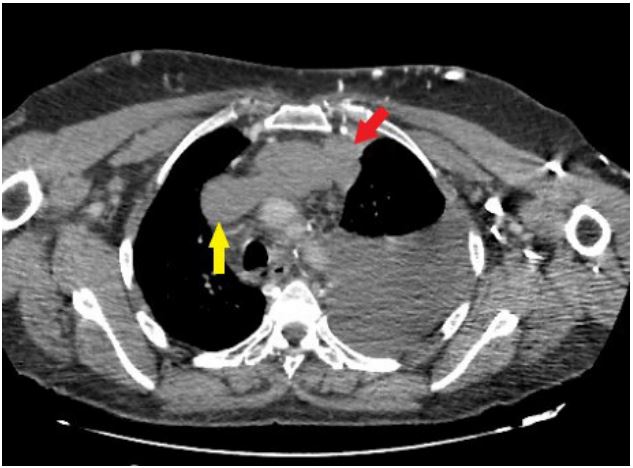
Figure 1:
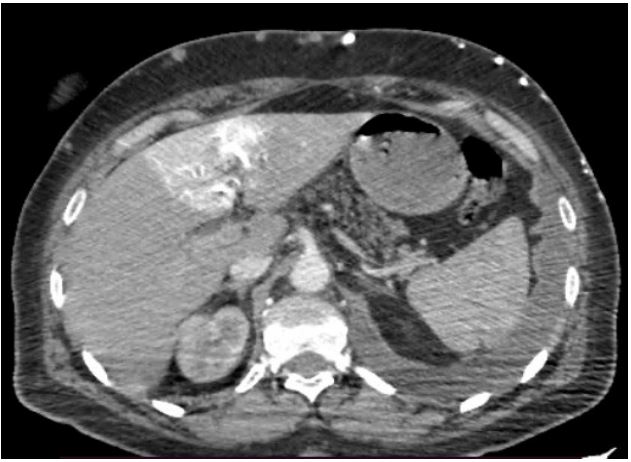
Figure 2:
References
- Dickson AM. The focal hepatic hot spot sign. Radiology. 2005; 237: 647-648.
- Hoang VT, Vo NQ, Trinh CT, et al. The focal hepatic hot spot sign with lung cancer in computed tomography. Respirol Case Rep. 2020; 8: 00671.
- Stanford W, Jolles H, Ell S, Chiu LC. Superior vena cava obstruction: A venographic classification. AJR Am J Roentgenol. 1987; 148: 259-62.
- Sureka B, Sullere A, Singh Khera P. CT quadrate lobe hot spot sign. Middle East J. Dig. 2018; 10: 192-193.
