
Open Access, Volume 9
A rare case of Jackhammer esophagus presenting with reflux-like symptoms in Guizhou, China
Jie Yang3*; Yurong Huang1; Dongmei Chen1; Wangliu Yang2; Junjie Rao2; Canyu Zhan2; Lei He2; Gengqing Song4
1Department of Gastroenterology, Liupanshui People’s Hospital, Liupanshui City, 553000, Guizhou Province China.
2Guizhou Medical University, Guiyang City, 550004, Guizhou Province China.
3Department of Gastroenterology, The Affiliated Hospital of Guizhou Medical University, Guiyang City, 550004, Guizhou Province China.
4Department of Gastroenterology and Hepatology, Metrohealth Medical Center, Case Western Reserve University, Cleveland, OH, USA.
Jie Yang
Department of Gastroenterology, The Affiliated Hospital of Guizhou Medical University, Guiyang City,
550004, Guizhou Province China.
Tel: 216-778-4123;
Email: Yangjielaila@163.com
Received : Oct 05, 2023,
Accepted : Dec 20, 2023
Published : Dec 29, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Jackhammer Esophagus (JE) is a rare esophageal motility disorder characterized by hyperdynamic contraction of the distal esophagus. High-Resolution Esophageal Manometry (HREM) remains the diagnostic benchmark. Clinically, JE manifests as dysphagia, chest pain, and symptoms suggestive of gastroesophageal reflux [1] often leading to misdiagnosis as Gastroesophageal Reflux Disease (GERD). Treatment approaches lack unified guidelines, with notable variability in outcomes. Initial management typically favors medical interventions [2]. This article examines the diagnostic and therapeutic journey of a JE case and provides insights into recent advancements in its diagnosis and management.
Keywords: Jackhammer esophagus; Dysphagia; High-resolution esophageal manometry; Hyperdynamic contraction.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Yang J (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Yang J, Huang Y, Chen D, Yang W, Rao J, Zhan C, He L, et al. A rare case of Jackhammer esophagus presenting with refluxlike symptoms in Guizhou, China. Open J Clin Med Case Rep. 2023; 2175.
Case Presentation
A 51-year-old female presented with a year-long history of chest pain, heartburn, and dysphagia, often triggered by swallowing saliva. Interestingly, her dysphagia improved post-meal, without accompanying nausea or vomiting. She denied palpitation or shortness of breath. The symptoms are moderate in severity. Cardiac workups were normal. History and personal history were unremarkable. Cardiopulmonary abdominal examination was unrevealing. Prior Esophagogastroduodenoscopy (EGD) suggested mild esophagitis and chronic gastritis. Despite being on Proton Pump Inhibitor (PPI) treatments like omeprazole and lansoprazole twice daily, her symptoms showed minimal improvement. Notably, esophageal manometry and a 24-hour pH impedance test had not been conducted. A repeated EGD revealed chronic non-atrophic gastritis with bile reflux, GERD with Los angel grade A esophagitis and a small hiatal hernia (Figure 1). HREM displayed DCI > 8000 mmHg-s-cm in 3 out of 10 swallows. The resting pressure of Upper Esophageal Sphincter Pressure (UESP) and Lower Esophageal Sphincter Pressure (LESP) recorded normal pressures. The manometric findings were consistent with a hypercontractile/Jackhammer esophagus diagnosis (Figure 2). 24-hour pH-impedance monitoring, conducted after a week without PPIs, indicated a normal total acid exposure time (0.1%). The symptom index was negative for heartburn or regurgitation, suggesting functional heartburn. Upper GI series identified a small mound-like dense barium shadow in the upper esophagus, raising suspicions of a small esophageal diverticulum (Figure 3). Chest CT findings were normal. The Self-Rating Anxiety Scale (SAS) produced a score of 56 points, indicative of mild anxiety. Conversely, the Self-Rating Depression Scale (SDS) score of 50 points was within normal limits. Diagnosis conclusions were: 1. Jackhammer esophagus; 2. Functional heartburn; 3. Mild anxiety. For two months, the patient underwent treatment with Rabeprazole (20 mg, bid), Flupentixol and melitracen (Deanxit, 10.5 mg bid) for anxiety and functional heartburn. Post-treatment, her chest pain, heartburn, and dysphagia were resolved. The SAS showed an improvement to the normal range at 34 points. She decided to stop the medication given her symptoms resolved. Upon symptom resolution, she ceased medication. However, a milder form of dysphagia returned 10 days post-medication discontinuation, with no other issues. She managed symptoms through dietary and lifestyle adjustments. We advised 6-12 months of periodic observations, with potential HREM repetition. A year later, she remained intermittent mild symptoms, opted to defer the HREM test, and preferred ongoing clinical observation.
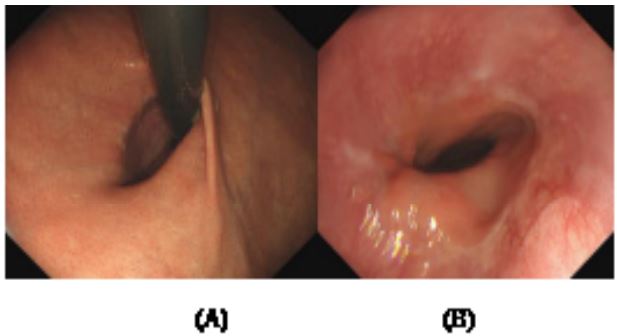
Figure 1: (A) Small Hiatal hernia. (B): Reflux esophagitis (grade A).
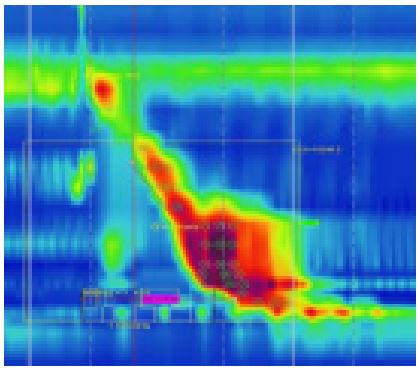
Figure 2: HRM plot showing hypercontractility of
the esophageal body in the upright position.

Figure 3: Esophageal diverticulum?.
Discussion
JE is identified in approximately 4% of patients undergoing esophageal manometry [3]. It is the underlying cause in about 4.5% of non-obstructive dysphagia cases. The exact pathogenesis of JE remains elusive, but potential mechanisms include excessive cholinergic activity, asynchronous contractions of esophageal smooth muscle, Esophagogastric Junction (EGJ) outflow obstruction, and increased thickness of the esophageal muscle layer [4]. Previously termed ‘nutcracker esophagus’, the condition was officially renamed JE with the introduction of the Chicago 3.0 criteria [5]. In the Chicago 4.0 criteria, JE is manometrically defined by ≥20% DCI exceeding 8000 mmhg.s.cm, a normal distal latency, and associated clinical manifestations like dysphagia and chest pain. Mechanical obstructions, such as achalasia or distal esophageal spasm, must be ruled out before confirming the diagnosis [6]. In this case, DCI > 8000 mmHg-s-cm was found in 3 out of the 10 swallows in HREM, which met the diagnostic criteria of JE. To date, the literature cites over 500 reported cases of JE [1]. While JE diagnosis hinges on high-resolution esophageal manometry, HREM equipment in China is primarily located within tertiary medical centers. Consequently, access in less developed areas like Guizhou remains limited. As a result, JE case reports from China, and notably from Guizhou Province, are infrequent, making the incidence uncertain. This particular case is only the second documented in Guizhou Province [7]. Underscoring the equipment scarcity in the region. This highlights the significance of esophageal manometry for diagnosing patients presenting with unexplained chest pain and dysphagia. Dysphagia was the most common symptom of JE (64%), followed by reflux symptoms (46%), and 1/3 patients had chest pain [2]. Although JE is characterized by typical esophageal motility disorders, the relationship between JE symptoms and esophageal anomalies as seen on HREM is still unclear. Kristo et al [8] revealed a strong correlation between DCI contractility and JE symptoms, with both chest pain and dysphagia linked to increased body contractility. Heregods, et al [9] identified dysphagia as being connected to intense contractions of the LES, potential outflow obstruction indicators, and an exceptionally high DCI (>8000 mmHg-s-cmI). In the patient’s HREM, there was a notable increase in DCI value during simulated physiological swallowing. The esophageal body exhibited intense, uncoordinated contractions, which seemed to correlate with her dysphagia. Interestingly, her dysphagia primarily manifested during saliva swallowing but eased after food consumption. This divergence between heightened DCI during swallowing and symptom relief post-eating suggests that JE symptoms might not be solely due to heightened esophageal contractions.
Around 40% of JE patients present with symptoms reminiscent of GERD [10], causing potential diagnostic confusion. Some hypothesize that acid reflux may play a role in JE’s onset since suppressing gastric acid can amplify high-pressure peristalsis [11,12]. Conversely, an alternative perspective suggests that JE is unrelated to pathological acid exposure but is linked to cholinergic overactivity and vagus nerve dysfunction [10]. Supporting this latter theory, our patient showed no signs of pathological acid reflux. Given the overlap of GERD symptoms, esophageal hypersensitivity, and mental health comorbidities in JE, many experts advocate for medical therapy as the primary treatment modality for JE. The goal is to manage predominant symptoms and reduce abnormal esophageal contractions. PPIs have been effective in alleviating both chest pain and dysphagia. Additionally, treatments like calcium channel blockers, nitrates, and phosphodiesterase inhibitors have been used to modulate contractile activity [4]. PPIs have the potential to alleviate hypercontractile dysphagia associated with JE. Yet, questions remain regarding the ideal treatment duration, effectiveness, recurrence rate, and duration of maintenance therapy. Moreover, while empirical PPIs therapy can be effective, it might obscure a JE diagnosis. This is illustrated by the extended, sometimes ineffective, use of PPIs in this case until diagnosis was made via HREM. Thus, for patients with persistent GERD symptoms, prompt HREM and 24-hour pH impedance monitoring should be considered to evaluate PPIs effectiveness. Nifedipine is recognized as a potential therapeutic option for JE symptoms [13]. Several studies have shown Deanxit to be beneficial for JE patients with EGJ Outflow Obstruction (EGJOO) unresponsive to combined PPIs and nifedipine treatment [14]. Funaki Y et al [15] found steroid therapy effective in a few allergy-related JE cases, including EoE. Interestingly, the combination of PPIs and Deanxit led to the resolution of heartburn and chest discomfort and marked improvement in dysphagia, hinting at a possible link between mental disorders and JE. After two years, a quarter of JE-diagnosed patients were seen to progress to achalasia type III. Impaired relaxation of the EGJ emerged as the primary risk factor for this progression [16]. An elevated Integrated Relaxation Pressure (IRP), either alone or coupled with EGJOO, stands as a pivotal marker in predicting achalasia’s development from JE, and hence, the potential need for Peroral Endoscopic Myotomy (POEM). A meta-analysis indicated that 73.6% of JE-diagnosed patients showed clinical symptom improvement post-treatment. Within this group, endoscopic treatments comprised 79%, medical treatments 63%, and POEM boasted a clinical success rate of 82% [12]. Successful POEM applications in pediatric JE cases have also been noted [17]. Beyond pharmacological treatments, endoscopic POEM holds a key position in JE management. Given the patient’s moderate IRP, careful consideration is essential when contemplating POEM or surgical measures. Considering the nuances of JE pressure readings, some international experts have proposed a modified POEM technique to address issues like ineffective esophageal motility and sigmoid esophagus that may arise from the standard POEM method. This refined technique involves determining the level of esophageal hypertension via HREM, conserving the lower esophageal sphincter, and only partially removing the outer layer of the ringed muscle, rather than a full removal. Postoperatively, all symptoms were resolved within a year without complications [18]. Although POEM remains the primary endoscopic treatment for this ailment, other strategies, such as endoscopic carnitine injection and balloon dilation, have been considered [19,20]. These alternative approaches are less technically demanding and associated with fewer complications, but their efficacy falls short of that achieved with POEM. Esophageal diverticula, possibly associated with JE, can occur in the upper, middle, or lower segments of the septum. Symptoms in affected individuals often improve post-esophageal diverticulum resection and esophageal myotomy, which usually brings the DCI value back within normal range [21-23]. However, it is important to note that esophageal diverticulum is more prevalent than JE. Further evidence is required to establish a causal relationship between JE and esophageal diverticulum, or vice versa. The patient’s diagnosis of Reflux Esophagitis (RE) was classified as Los Angeles grade A. Extensive research has indicated that Los Angeles grade C or D in RE is associated with an elevated occurrence of pathological acid reflux, whereas grade A typically exhibits minimal acid exposure and physiological acid reflux is prevalent. Consequently, the endoscopic observations of Los Angeles Class A esophagitis do not align with the presence of GERD characterized by pathological acid reflux. In essence, it can be concluded that endoscopic RE with grade A, does not necessarily signify the presence of GERD [24]. In conclusion, JE is a relatively rare condition manifested by chest pain, dysphagia and symptoms resembling reflux. It can potentially evolve into achalasia type III. The primary diagnostic tool for JE is HREM. At present, there’s no standardized treatment protocol for JE, with pharmacotherapy often being the first line of intervention. For JE patients without elevated IRP, a modified POEM might be an appropriate endoscopic surgical alternative. Effective JE management necessitates an ongoing approach to chronic disease care, coupled with comprehensive follow-ups to refine therapeutic results. Future studies should aim to better comprehend the pathophysiological underpinnings of esophageal hypermotility and more clearly define the association between heightened esophageal body contractions and JE.
References
- Achem SR, Vazquez-Elizondo G, Fass R. Jackhammer Esophagus: Current Concepts and Dilemmas. J Clin Gastroenterol. 2021; 55: 369-379.
- Wahba G, Bouin M. Jackhammer esophagus: A meta-analysis of patient demographics, disease presentation, high-resolution manometry data, and treatment outcomes. Neurogastroenterol Motil. 2020; 32: e13870.
- Jia Y, Arenas J, Hejazi RA, Elhanafi S, Saadi M, et al. Frequency of Jackhammer Esophagus as the Extreme Phenotypes of Esophageal Hypercontractility Based on the New Chicago Classification. J Clin Gastroenterol. 2016; 50: 615-8.
- De Bortoli N, Gyawali PC, Roman S, et al. Hypercontractile Esophagus From Pathophysiology to Management: Proceedings of the Pisa Symposium. Am J Gastroenterol. 2021; 116: 263-273.
- Kahrilas PJ, Bredenoord AJ, Fox M, et al. The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil. 2015; 27: 160-74.
- Yadlapati R, Kahrilas PJ, Fox MR, et al. Esophageal motility disorders on high-resolution manometry: Chicago classification version 4.0©. Neurogastroenterol Motil. 2021; 33: e14058.
- Huan Yao, Yuxin Xie, Jianyi Guo, Hong Wang, Guoqing Shi. A case of Jackhammer esophagus treated with nifedipine. Hainan Medical journal. 2020; 31: 2708-2710.
- Kristo I, Schwameis K, Paireder M, Jomrich G, Kainz A, et al. Dysphagia severity is related to the amplitude of distal contractile integral in patients with Jackhammer esophagus. Neurogastroenterol Motil. 2018; 30: e13276.
- Herregods TV, Smout AJ, Ooi JL, Sifrim D, Bredenoord AJ. Jackhammer esophagus: Observations on a European cohort. Neurogastroenterol Motil. 2017; 29.
- Woo M, Liu A, Wilsack L, et al. Gastroesophageal Reflux Disease Is Not Associated with Jackhammer Esophagus: A Casecontrol Study. J Neurogastroenterol Motil. 2020; 26: 224-231.
- Mallet AL, Ropert A, Bouguen G, et al. Prevalence and characteristics of acid gastro-oesophageal reflux disease in Jackhammer oesophagus. Dig Liver Dis. 2016; 48: 1136-41.
- Kristo I, Schwameis K, Maschke S, et al. Phenotypes of Jackhammer esophagus in patients with typical symptoms of gastroesophageal reflux disease responsive to proton pump inhibitors. Sci Rep. 2018; 8: 9949.
- Sirinawasatien A, Sakulthongthawin P. Manometrically jackhammer esophagus with fluoroscopically/endoscopically distal esophageal spasm: A case report. BMC Gastroenterol. 2021; 21: 222.
- Li JY, Zhang WH, Huang CL, Huang D, Zuo GW, et al. Deanxit relieves symptoms in a patient with jackhammer esophagus: A case report. World J Gastrointest Endosc. 2017; 9: 590-593.
- Funaki Y, Ogasawara N, Kawamura Y, et al. Markedly Effective Steroid Treatment of Three Patients with Allergy-related Jackhammer Esophagus. Intern Med. 2020; 59: 633-639.
- Huang L, Pimentel M, Rezaie A. Do Jackhammer contractions lead to achalasia? A longitudinal study. Neurogastroenterol Motil. 2017; 29.
- Ramos RI, Guidi M, Kakisu MH, Rocca AM, Sakai P. Peroral endoscopic myotomy in pediatric jackhammer esophagus. Rev Esp Enferm Dig. 2018; 110: 464-465.
- Choi YI, Kim KO, Park DK, Chung JW, Kim YJ, et al. Clinical outcomes and safety of high-resolution manometry guided superficial partial circular muscle myotomy in per-oral endoscopic myotomy for Jackhammer esophagus: Two cases report. World J Clin Cases. 2019; 7: 2322-2329.
- Marjoux S, Brochard C, Roman S, et al. Botulinum toxin injection for hypercontractile or spastic esophageal motility disorders: may high-resolution manometry help to select cases. Dis Esophagus. 2015; 28: 735-41.
- Pelletier AL, Pospai D, Merrouche M. Balloon against Jackhammer Disorder. Case Rep Gastroenterol. 2013; 7: 467-9.
- Fujinaga A, Shibata T, Etoh T, et al. Laparoscopic transhiatal surgery for an epiphrenic esophageal diverticulum derived from a jackhammer esophagus: A case report. Surg Case Rep. 2020; 6: 151.
- Sachdeva S, Singh AK, Kumar M, George R. Jackhammer esophagus: Rare cause of esophageal diverticulum. Dig Liver Dis. 2021; 53: 1051-1052.
- Khullar OV, Shroff SR, Sakaria SS, Force SD. Midesophageal Pulsion Diverticulum Resulting From Hypercontractile (Jackhammer) Esophagus. Ann Thorac Surg. 2017; 103: e127-e129.
- Ghisa M, Barberio B, Savarino V, et al. The Lyon Consensus: Does It Differ From the Previous Ones. J Neurogastroenterol Motil. 2020; 26: 311-321.
