
Open Access, Volume 9
A rare case of severe isolated temporomandibular joint involvement in juvenile idiopathic arthritis
Vassilis Psarras
Orofacial Pain Clinic, School of Dentistry, National & Kapodistrean University of Athens, Greece.
Email: vpsarras@dent.uoa.gr
Received : Nov 25, 2023,
Accepted : Dec 18, 2023
Published : Dec 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Juvenile idiopathic arthritis is an inflammatory condition of unknown etiology. Early temporomandibular joint involvement may be asymptomatic or with mild symptomatology, despite radiological signs of substantial joint damage. Early diagnosis and management is of substantial importance, because orofacial symptoms due to temporomandibular joint arthritis may be disabling and interfere with impaired quality of life or even dentofacial abnormalities. When temporomandibular joint involvement is the first and only manifestation - a very rare event – it is easy to remain undiagnosed. It is noteworthy that the current body of published material on isolated arthritis of the temporomandibular joint is limited to 2 case reports and a multinational cohort of pediatric rheumatology centers.
Case presentation: A 14-year-old Caucasian girl presented with orofacial pain and painful limited opening of the mouth, for a month. A crepitation sound could be detected from the left temporomandibular joint, which is considered pathognomonic sign of structural alterations of the joint. The panoramic radiograph depicted significantly atypical image of the temporomandibular joint. The cone beam computed tomography revealed significant degenerative alterations. Since, the medical history was free and there was no mention of fall or injury, the rheumatologic control was deemed necessary. The diagnosis set was that of Juvenile idiopathic arthritis. Systemic therapy and a stabilization splint were administered resulting in significant improvement in the patient’s signs and symptoms.
Conclusions: There are very few cases, where the temporomandibular joint is the initial sole joint affected. Diagnosing could be challenging, necessitating detailed patient history, standardized high level clinical examination, and proper imaging techniques. When making treatment decisions for Juvenile Idiopathic Arthritis, it is important to take into account factors related to the temporomandibular joint.
Keywords: Juvenile idiopathic arthritis; Temporomandibular joint arthritis; Temporomandibular joint involvement; Treatment; Craniomandibular disorders; Case report.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Psarras V (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Psarras V. A rare case of severe isolated temporomandibular joint involvement in juvenile idiopathic arthritis. Open J Clin Med Case Rep. 2023; 2174.
Introduction
Juvenile idiopathic arthritis (JIA) is a disorder characterized by inflammation, the cause of which is still unknown. The prevalence rate is 70 per 100,000 individuals in the pediatric and adolescent population [1]. The prevalence of arthritis involvement in the temporomandibular joint (TMJ) range from 40% to 93%, depending on the examination method employed and the subtypes of JIA studied [2].
TMJ involvement in JIA has been consistently undervalued in the past. This is primarily due to the fact that early TMJ arthritis often presents as either asymptomatic or with mild symptoms, even in the presence of significant joint damage as displayed by radiological evidence [3]. As the disease advances, a considerable number of patients encounter orofacial function impairment. The primary manifestations are restricted maximal opening capacity, discomfort or pain during maximal mouth opening and mastication (often affecting both the TMJ and the masseter muscle regions) and TMJ morning stiffness. The inflammatory process and associated orofacial signs and symptoms have the potential to persist into adulthood [4-6].
Once the JIA diagnosis has been established and orofacial symptoms have manifested, the identification of TMJ arthritis becomes a relatively straightforward task. Nevertheless, in cases where the TMJ is affected as the initial and sole joint, -a rather uncommon occurrence- it can be challenging to set proper diagnosis. It is noteworthy that the current body of literature about isolated TMJ arthritis comprises two case reports [7,8] and a multinational cohort study, conducted across pediatric rheumatology clinics [9]. The timely identification and treatment of TMJ arthritis is crucial as it can cause disruption to daily activities and significant impairment of the patient`s quality of life [10,11]. Stoustroup et al reporting follow-up data from 351 JIA patients, at 36 months following the initial clinical examination and 5 years after the onset of JIA, found that the cumulative incidence of orofacial symptoms were 8% and 53% at these respective time points. Thirty five percent (35%) of the participants exhibited dentofacial abnormalities, such as mandibular asymmetry, mandibular posterior rotation, or micrognathia and retrognathia, with a strong association to the prevalence of orofacial dysfunction [12].
We present a rare case (the third published, at least according to our knowledge) of a 14-yearold adolescent who exhibited TMJ involvement as the sole joint affected. The first manifestation of TMJ involvement prompted further examination, which eventually led to the diagnosis of juvenile idiopathic arthritis (JIA). This case has been based on the CARE reporting guidelines [13] written informed consent was obtained from the patient’s legal guardian.
Case Presentation
A 14-year-old girl presented to the office, complaining of orofacial pain, mostly at the left side of the face and painful limited opening of the mouth, for a month (Figure 1). The severity of the symptoms impaired the individual’s ability to engage in regular school activities, necessitating the administration of analgesics (paracetamol), which failed to provide notable relief. The comprehensive history of the patient revealed the presence of clicking sounds emanating from the TMJ, which ceased around one year ago. The patient disclosed the presence of bruxism, encompassing both nocturnal and daytime episodes, in addition to engaging in parafunctional activities such as cheek, lip, object, and nail-biting. She described herself as anxious and quite nervous (grade 8, on a scale from 0=calm to 10=very nervous), while her social relationships at school and within the family were characterized as medium (grade 5-on a scale from 0 =very good, to 10=very bad).
The clinical examination of the patient comprised of the palpation of the TMJ and the main muscles of the stomatognathic system (Table 1). During the TMJ examination, the maximum opening was 28 mm and painful (Figures 2 and 3). During opening the jaw deviated to the left. Finally, the maximum laterotrusion to the left was limited to 5 mm, in contrast to 10 mm to the right, which is considered normal (Table 2). An important clinical finding was the presence of crepitation sound from the left TMJ, a pathognomonic sign of structural alterations of the joint.
On presentation, the patient had a panoramic radiograph, where the TMJ depicted rather atypical (Figure 4). The diagnostic process could not rely on this x-ray, due to the overlaps with other anatomical elements in the region; this additional imaging techniques deemed necessary [14]. The Cone beam computed tomography (CBCT) which was selected in this instance, revealed on the right side that the condyle was centrally positioned, while erosive lesions were seen in the upper anterior region of the condyle at the medial pole. Microerosions at the outer pole could not be ruled out. Early to moderate degenerative alterations were consistent with this image (Figure 5).
On the left side, the condyle was posteriorly displaced, although the joint space remained within the expected range. An extensive erosive lesion, approximately about 5 mm in diameter was evident in the posterior- superior portion of the condyle. This lesion occupied the whole middle third of the condyle head and was surrounded by a sclerotic margin. This image was indicative of a higher degree of degenerative alterations (Figure 6).
During opening, the right condyle exhibited displacement sliding on the posterior part of the articular eminence, although not to a fully extent, suggesting diminished range of motion (Figure 7). The left condyle performed only rotational movement around its hinge axis, without any displacement sliding on the posterior part of the articular eminence. This finding is compatible with a clearly limited opening movement (Figure 8). Despite our persistent questions no incident of injury or fall was reported by the patient that can justify that the structural changes and the limitation of movement could be of traumatic etiology.
Subsequently, the consultation of a pediatric rheumatologist was sought to assess the potential presence of a systemic health condition. Given the absence of a blood test for diagnosing JIA, the identification of this ailment in certain children and/or adolescents who present with first complaints of pain and joint swelling can pose challenges. In the context of rheumatoid arthritis (RA), it is commonly observed that adults exhibit a positive rheumatoid factor (RF) blood test result, whereas children diagnosed with JIA tend to exhibit a negative RF blood test result. Indeed in our case, the laboratory immunology testing revealed normal levels of complement C3, C4, and total C, as well as a negative result for rheumatoid factor. The diagnosis of JIA is typically established through the examination of physical manifestations, analysis of medical records, assessment of personal medical history, and consideration of recent pathological events. The physical examination findings encompass the presence of limping, stiffness upon awakening, hesitancy to utilize a limb, decreased degree of activity, persistent fever, and further accompanying symptoms [15]. In our case, the intensity of the clinical condition combined with the joint`s destruction depicted to the CBCT image, necessitated the administration of systemic treatment. Systemic administration of cortisone and methotrexate initially, and a biological agent (adalimumab) was the approach taken.
In some instances, the symptoms and dysfunction of the TMJ may be attributed to excessive mechanical loading in the joints, which could originate from prior inflammation of the TMJ [16]. Considering the fact that the temporomandibular joint (TMJ) is a relatively small joint that bears a substantial functional and dysfunctional load, relying solely on systematic treatment many times is inadequate for the relief of signs and symptoms of the craniomandibular system. The stabilizing splint used was a custom-made device, made of heat-polymerised acrylic resin, constructed in the laboratory, after detailed impressions of both the upper and lower dental arches (Figure 9). The height of the splint was based on a clinical assessment, on an effort that the masticatory muscles experience minimal tension and the TMJ`s were minimally loaded. The splint was constructed without any occlusal guiding interdentations, resulting in a flat design. The initial occlusal adjustment aimed to ensure equal and uniform contacts between the splint and the opposing teeth across the entire length of the splint; the splint was also adjusted in consecutive appointments, as the clinical condition improved, in order to provide a stable occlusal relationship. The patient was provided with instructions to utilize the splint throughout the sleeping hours, at the very least. During the first weeks, further use of the splint was advised, taking into consideration the patient`s clinical evaluation. The patient was given instructions for the self-regulation of day-bruxism and the modifying of certain orofacial behaviors and parafunctional habits that exert excessive strain on her craniomandibular system (such as cheek, lip, object, and nail biting). Additionally, she was given kinesiotherapy, comprise of light resistance exercises to enhance muscular coordination. The application of the splint should be tailored to the specific needs of each patient, taking into consideration the pain and the accompanied symptoms. In any case, the use of the splint should not exceed the two months, because the young patient had not completed her dento-alveolar development.

Figure 1: The patient’s response upon being directed to
point out the spot of greatest discomfort by means of a
finger

Figure 2: The patient in maximum opening.

Figure 3: The maximum opening using the upper and
lower incisor edges, as reference points was limited (28
mm, when the normal is >40 mm) and painful.

Figure 4: The panoramic X-ray is a diagnostic imaging
technique used in dentistry that provides a broad angle
of the teeth and jaws. Both sides of the TMJ are also depicted. Atypical morphology can be noticed in the temporomandibular joints, despite their potential overlap with
other anatomical structures.
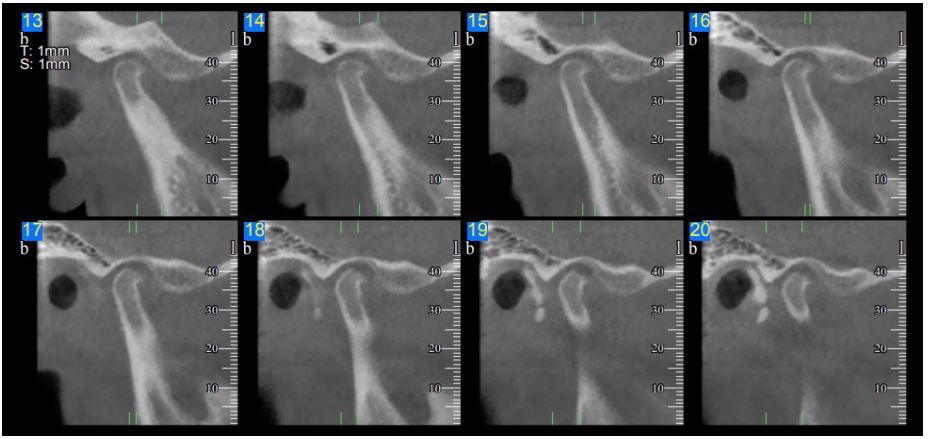
Figure 5: The cone beam computed tomography (CBCT) image of the right TMJ in close mouth position. The condyle was
centrally positioned, while erosive lesions were seen in the upper anterior region of the condyle at the medial pole. Microerosions at the outer pole could not be ruled out. Early to moderate degenerative alterations were consistent with this image.
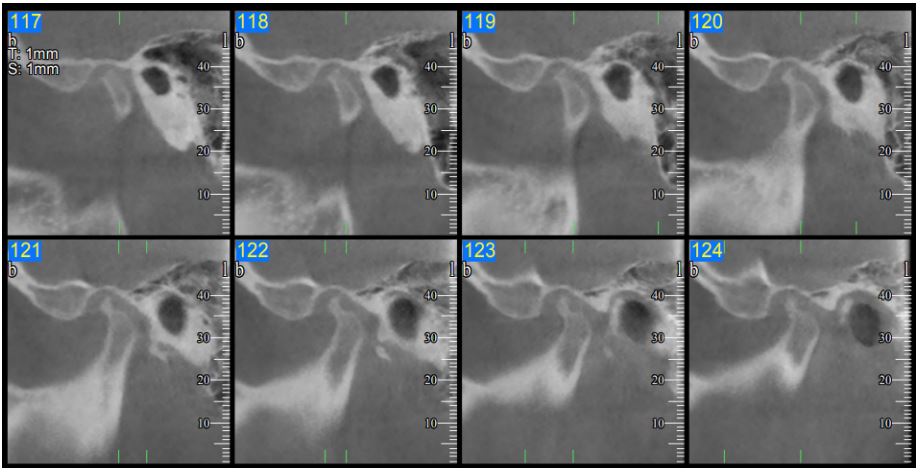
Figure 6: The cone beam computed tomography (CBCT) image of the left TMJ in close mouth position. The condyle was
posterior displaced, and an extensive erosive lesion (arrow), approximately about 5 mm in diameter was evident in the posterior- superior portion of the condyle. This lesion occupied the whole middle third of the condyle head and was surrounded
by a sclerotic margin. This image was indicative of extensive degenerative alterations.
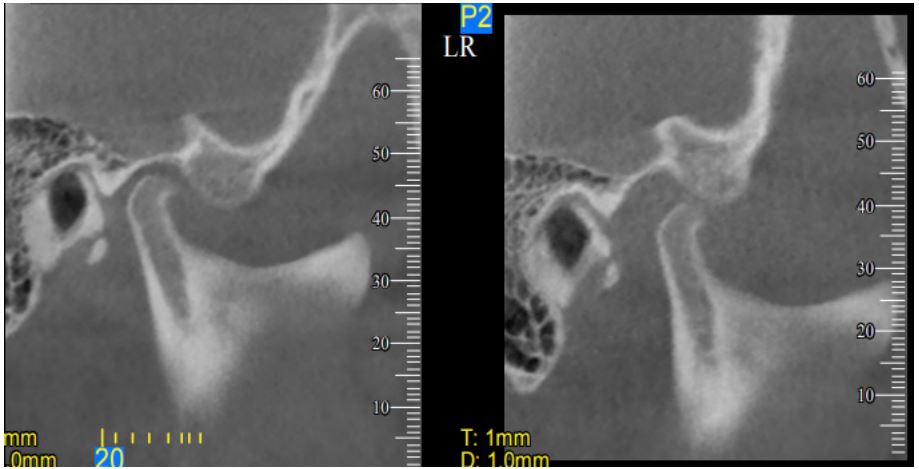
Figure 7: The cone beam computed tomography (CBCT) image of the right TMJ in close (left) and open (right) mouth position (close view). During opening, the right condyle exhibited displacement sliding on the posterior part of the articular
eminence, although not to a fully extent, suggesting diminished range of motion.
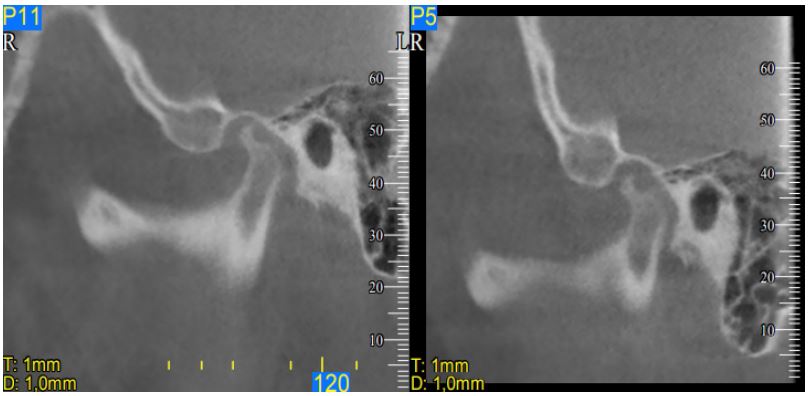
Figure 8: The cone beam computed tomography (CBCT) image of the left TMJ in close (left) and open (right) mouth position
(close view). During opening, the condyle performed only rotational movement around its hinge axis, without any displacement sliding on the posterior part of the articular eminence. This finding is compatible with a clearly limited opening movement. Compare to the right side. Notice also the extent of the erosion.

Figure 9: The patient with the stabilization splint in the emouth. The height of the splint was based on a clinical assessment,
on an effort that the masticatory muscles experience minimal tension and the TMJ`s were minimally loaded.
Table 1: Clinical examination of the orofacial and the neck muscles. The absence of pain is recorded with a dash (-), the presence of sensitivity with one +, the presence of pain with two ++ and the presence of intense pain with three +++ depending on its intensity.
| Orofacial muscles | Right | Left |
|---|---|---|
| Temporalis anterior | - | ++ |
| Temporalis middle | - | - |
| Temporalis posterior | - | - |
| Tendon of the temporalis | +++ | ++ |
| Masseter -superficial | - | +++ |
| Masseter -deep | - | - |
| Medial pterygoid | - | - |
| Lateral pterygoid | - | +++ |
| Sternoclidomastoid | - | - |
| Trapezius | - | - |
| Occipital region of the neck | - | - |
Table 2: Clinical examination of the TMJ function. Move- ments of the mandible with or without pain compared to the minimum normal values. The absence of pain is recorded with a dash (-), the presence of sensitivity with one +, the presence of pain with two ++ and the presence of intense pain with three +++ depending on its intensity.
| Clinical examination – TMJ function | mm | Normal range | Pain |
|---|---|---|---|
| Maximum mandibular protrusion | 6 | >7 | - |
| Maximal mouth opening capacity | 28 | >40 | ++ |
| Maximul laterotrusion (right) | 10 | >7 | - |
| Maximul laterotrusion (left) | 5 | >7 | + |
| Mouth opening deviation | 2.5mm |
Discussion
JIA is a relatively common rheumatic condition in children and adolescents. As the condition advances, it can give rise to a notable decline in the overall well-being of the young individuals. In patients who have not yet reached skeletal maturity, JIA has the potential to adversely affect the growth and development of the facial region, leading to the manifestation of dentofacial deformities. Specifically, it could result in the destruction of the growth centers in the TMJs. This can lead to facial asymmetry when the affected joint is on the opposite side of the face, and to a distinct bird-like facial appearance when both joints are affected, which occurs in approximately one-third of cases [17,18].
The process of diagnosing the condition remains challenging and should encompass a comprehensive patient history, and a systematic clinical examination. The use of gadolinium-enhanced magnetic resonance imaging (Gd-MRI) is considered the gold standard for the detection of active TMJ arthritis [19], since it has the capability to identify both inflammatory and osseous alterations. It presents specific difficulties when applied to younger individuals; mostly due to the extended duration of the examination. The presence of metal braces, a quite common event in children and adolescents at such an age, can cause interference during the imaging process. Cone-beam computed tomography (CBCT) is a three-dimensional morphometric imaging technique, not as efficient in detecting active TMJ arthritis as the MRI. However, it provides a comprehensive analysis of osseous changes and it surpasses other methods in assessing dentofacial morphology [20].
Orofacial complaints demonstrate temporal fluctuation; the stabilizing splint offers a palliative effect rather than a curative one on these symptoms. However, studies have reported that the functional benefits of the orofacial system by the use of a stabilization splint for the management of TMJ arthritis-related orofacial symptoms in JIA were similar to, and in some cases surpass, the level of functional improvement of intra-articular TMJ steroid injection [21]. Another study demonstrated similar positive outcomes in terms of mouth opening and orofacial symptoms following the implementation of an orthopedic splint [22]. These orthopedic splints have the potential to reduce orofacial symptoms associated with JIA-TMJ and promote the normalization of mandibular and dentofacial development in patients who are still undergoing skeletal growth.
Even young patients frequently complain of symptoms related to the TMJ and the craniomandibular system. Sometimes, such common symptoms (such as sounds, pain, deviation and/or difficulty in opening of the mouth) may underlie serious problems of the patient`s general health. The dentist should be cautious and conduct a comprehensive evaluation when patients present with symptoms, such as TMJ and/or muscular pain.
Conclusion
The prevalence of juvenile idiopathic arthritis (JIA) affecting the TMJ is higher than previously believed. TMJ arthritis could result in long-lasting impairment of orofacial health and quality of life and dentofacial deformities, which may persist into adulthood. The suspicion and identification of TMJ involvement is usually easier when the systemic condition has previously been diagnosed. If TMJ arthritis is not recognized or treated adequately for a considerable period of time, starting from the initial TMJ involvement until the appearance of clinical signs and symptoms, it is inevitable that the condition may worsen. Unfortunately, there are rare cases, where the TMJ is the sole joint affected, with symptoms that closely resemble those of various other dysfunctional conditions. In such cases, setting proper diagnosis is challenging. A comprehensive approach that encompasses a detailed patient history, a standardized clinical examination, and the utilization of proper imaging techniques is necessary.
References
- Thierry S, Fautrel B, Lemelle I, Guillemin F. Prevalence and incidence of juvenile idiopathic arthritis: a systematic review. Joint Bone Spine. 2014; 81: 112-117.
- Pantoja LLQ, de Toledo IP, Pupo YM, Porporatti AL, De Luca Canto G, Zwir LF, Guerra ENS. Prevalence of degenerative joint disease of the temporomandibular joint: a systematic review. Clin Oral Investig. 2019; 23: 2475-2488.
- Arabshahi B, Cron RQ. Temporomandibular joint arthritis in juvenile idiopathic arthritis: the forgotten joint. Curr Opin Rheumatol. 2006; 18: 490-495.
- Engstrom AL, Wanman A, Johansson A, Keshishian P, Forsberg M. Juvenile arthritis and development of symptoms of temporomandibular disorders: a 15-year prospective cohort study. J Orofac Pain. 2007; 21: 120-6.
- Muller L, Kellenberger CJ, Cannizzaro E, Ettlin D, Schraner T, Bolt IB, et al. Early diagnosis of temporomandibular joint involvement in juvenile idiopathic arthritis: a pilot study comparing clinical examination and ultrasound to magnetic resonance imaging. Rheumatology (Oxford). 2009; 48: 680-5.
- Stoustrup P, Kristensen KD, Verna C, Kuseler A, Herlin T, Pedersen TK.Orofacial symptoms related to temporomandibular joint arthritis in juvenile idiopathic arthritis: smallest detectable difference in self- reported pain intensity. J Rheumatol. 2012; 39: 2352-8.
- Martini G, Bacciliero U, Tregnaghi A, et al. Isolated temporomandibular synovitis as unique presentation of juvenile idiopathic arthritis. J Rheumatol. 2001; 28(7): 1689-92.
- Scolozzi P, Bosson G, Jaques B. Severe isolated temporomandibular joint involvement in juvenile idiopathic arthritis. J Oral Maxillofac Surg. 2005; 63(9): 1368-71.
- Hügle B, Spiegel L, Hotte J, Wiens S, Herlin T, Cron RQ, Stoll ML, Vinod S, Stoustrup P, Pedersen TK, Twilt M.J. Isolated arthritis of the temporomandibular joint as the initial manifestation of juvenile idiopathic arthritis. J Rheumatol. 2017; 44(11): 1632-5.
- Isola G, Perillo L, Migliorati M, Matarese M, Dalessandri D, Grassia V, et al. The impact of temporomandibular joint arthritis on functional disability and global health in patients with juvenile idiopathic arthritis. Eur J Orthod. 2019; 41: 117-24.
- Frid P, Nordal E, Bovis F, Giancane G, Larheim TA, Rygg M, et al. Temporomandibular Joint Involvement in Association With Quality of Life, Disability, and High Disease Activity in Juvenile Idiopathic Arthritis. Arthritis Care Res. 2017; 69: 677-86.
- Stoustrup P, Glerup M, Bilgrau AE, Küseler A, Verna C, Christensen AE, Kristensen KD, Nørholt SE, Twilt M, Herlin T, Pedersen TK. Cumulative incidence of orofacial manifestations in early juvenile idiopathic arthritis: a regional, three-year cohort study. Arthritis Care Res 2020; 72(7): 907-16.
- Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D. The CARE guidelines: consensus-based clinical case reporting guideline development. Global Adv Health Med. 2013; 2(5): 38-43.
- Chih-Mong Tsai, Fang-Yu Wu, Jyh-Wen Chai, Mu-Hsiung Chen, Chih-Ting Kao. The advantage of cone-beam computerized tomography over panoramic radiography and temporomandibular joint quadruple radiography in assessing temporomandibular joint osseous degenerative changes. J Dent Sci 2020; 15(2): 153-162.
- Giancane G, Consolaro A, Lanni S, Davì S, Schiappapietra B, Ravelli A. Juvenile Idiopathic Arthritis: Diagnosis and Treatment. Rheumatol Ther. 2016; 3(2): 187-207.
- Stoustrup P, Pedersen TK, Nørholt SE, Resnick CM, Abramowicz S. Interdisciplinary management of dentofacial deformity in juvenile idiopathic arthritis. Oral Maxillofacial Surg Clin N Am. 2020; 32(1): 117-34.
- Hu Y, Billiau AD, Verdonck A, Wouters C, Carels C. Variation in dentofacial morphology and occlusion in juvenile idiopathic arthritis subjects: A case-control study. Eur J Orthod. 2009; 31: 51-8.
- Carvalho RT de, Braga FSFF, Brito F, Capelli Junior J, Figueredo CM, Sztajnbok FR. Temporomandibular joint alterations and their orofacial complications in patients with juvenile idiopathic arthritis. Rev Bras Reumatol. 2012; 52: 907-11.
- Stoustrup P, Resnick CM, Pedersen TK, Abramowicz S, Michelotti A, Küseler A, Verna C, Kellenberger CJ, Nordal EB, Caserta G, Jankovska I, Halbig JM, et al. Standardizing terminology and assessment for orofacial conditions in juvenile idiopathic arthritis: international, multidisciplinary consensus-based recommendations. J Rheumatol. 2019; 46(5): 518-22.
- Stoustrup P, Iversen CK, Kristensen KD, Resnick CM, Verna C, Nørholt SE, Abramowicz S, Küseler A, Cattaneo PM, Herlin T, Pedersen TK Assessment of dentofacial growth deviation in juvenile idiopathic arthritis: reliability and validity of three-dimensional morphometric measures. PLoS One 2018; 13: 0194177.
- Stoustrup P, Kristensen KD, Küseler A, Verna C, Herlin T, Pedersen TK. Management of temporomandibular joint arthritis-related orofacial symptoms in juvenile idiopathic arthritis by the use of a stabilization splint. Scand J Rheumatol. 2014; 43: 137-45.
- Isola G, Ramaglia L, Cordasco G, Lucchese A, Fiorillo L, Matarese G.The effect of a functional appliance in the management of temporomandibular joint disorder in patients with juvenile idiopathic arthritis. Minerva Stomatol. 2017; 66(1): 1-8.
