
Open Access, Volume 9
Back pain as a manifestation of Langerhans cell histiocytosis
Fátima Escalona Martín1*; María Toledano Macías2; Pablo Fuentes López3
1Resident in Medical Oncology, University Hospital of Fuenlabrada, Spain.
2Internal Medicine Physician, University Hospital of Fuenlabrada, Spain.
3Anatomopathologist, University Hospital of Fuenlabrada, Spain.
Fátima Escalona Martín
Resident in Medical Oncology, University Hospital of Fuenlabrada, Spain.
Email: fatima.escalona@salud.madrid.org
Received : Nov 17, 2023,
Accepted : Dec 13, 2023
Published : Dec 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Martín FE (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Martín FE, Macías MT, López PF. Back pain as a manifestation of Langerhans cell histiocytosis. Open J Clin Med Case Rep. 2023; 2171.
Background
Langerhans cell histiocytosis (LCH) is a neoplastic histiocytic disorder characterized by a broad spectrum of clinical manifestations, ranging from single organ lesions to a multi-systemic disease. Even though it is more common during the childhood, the incidence in adults is less defined and it may be misdiagnosed due to its clinical heterogeneity [1]. Main sites involved are bones (skull, vertebral bodies), lungs (typically in adult smokers) and skin (common in children). It is also important to assess the involvement of risk organs (liver, spleen or haemopoietic system) to determinate the severity of the diseas [2]. The definitive diagnosis requires a confirmation through histological and immunochemistry examinations, and molecular tests are also recommended to identify BRAF mutations and to estimate the prognosis and decide between different treatment strategies [3].
Objective: To highlight the main clinical manifestations of LCH and the importance of thinking in this pathology in case of clinical and radiological compatibility to achieve a correct diagnosis and give the patient targeted therapies.
Case Report
A 55-year-old man presented to an Internal Medicine physician after months of uncontrolled back pain despite of multiple therapies failure, asthenia, loss of weight and fever. Smoker, diagnosed of interstitial lung disease years ago, under follow-up by Pneumology and diagnostic doubts between bronchiolitis associated to tobacco smoking and pulmonary LCH, asymptomatic without specific treatment. Blood tests were unremarkable, with negative hepatitis serology and other infectious agents’ tests. Computer tomography of the chest showed centrilobular micronodules and cystic lesions in both lungs, with predilection for the mild and upper zones (Figure 1). These findings were consistent with the interstitial lung disease already known. A magnetic resonance of the spine showed multiple lytic bone lesions suggesting metastasis (Figure 2), so the study was completed with a PET scan that confirmed hypercaptation areas (Figure 3) in multiple vertebral bodies, scapula, pelvis, and costal arches.

Figure 1: Lung TC shows centrilobular micronodules
and cystic with predilection for the mild and upper
zones.
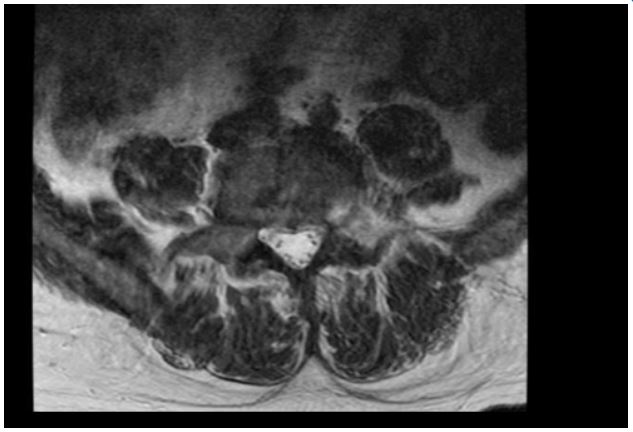
Figure 2: Lytic bone lesions in spine RM.
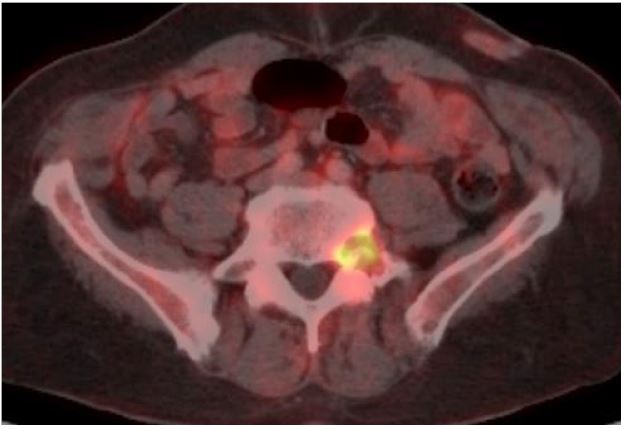
Figure 3: PET TC with hypercaptation of a lytic lesion
in L5.
A biopsy of one vertebral lesion confirmed the diagnosis of vertebral LCH. Histopathologic evaluation revealed clonal proliferation of histiocytoid cells with irregular nuclei with folding, grooves and indentations that remained Langerhans cells (Figure 4a), surrounded by lymphoplasmacytic infiltrate with eosinophils. The atypical cells were S100, CD1a and Langerin positive with immunochemistry (Figures 4b, 4c), and BRAF V600 mutation was confirmed (Figure 4d). The study was amplified with a skull TC that was unremarkable, so it was considered low-risk (BRAF mutation, no organic dysfunction or risk organ involvement).
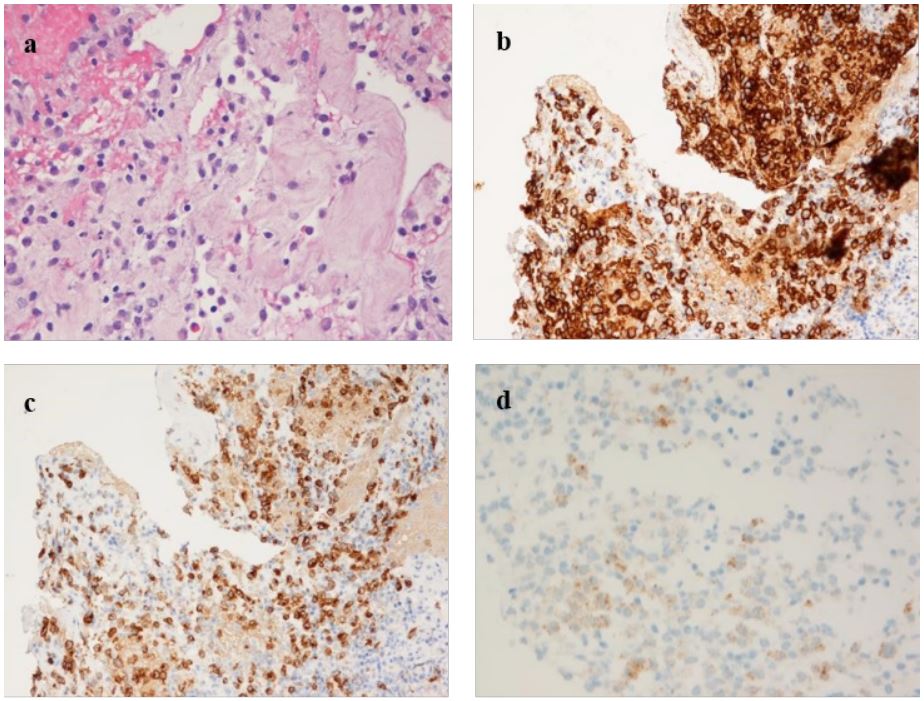
Figure 4: a. Hematoxilin-eosin stain. Typical findings of Langerhans cells: irregular nuclei with grooves and indentations
(“coffee beans” cells), surrounded by an infiltration of eosinophils.
b, c. Inmunochemistry studies. CD1a (b) and Langering stain (c).
cytoplasmic staining of the proliferating Langerhans cells.
d. Expresion of BRAF mutation in tumoral cells.
Once the diagnosis was low-risk LCH with pulmonary and bone involvement, the patient was derived to Hematology and
received targeted treatment with a BRAF inhibitor, vemurafenib, according to its extension and histopathology findings.
Discussion
LCH is often difficult to discriminate from other disorders because of its wide range of clinical manifestations, and it is divided into single and multisystem types [4]. In our patient the leading symptom was back pain, and the previous findings of pulmonary LCH made us think of bone involvement of the same process. Finally, a biopsy of one lesion in a vertebral body led us to the diagnosis and this case was considered a multysistemic type. Bone involvement is the most frequent site in children and lung involvement is common in adults, as smoking is considered a main risk factor [1,4] and our patient was smoker. Histological examination showed atypical cells with irregular nuclei with grooves and indentations (called “coffee beans”), and were S100 and CD1a positive with immunochemistry, which are typical findings [5]. BRAF V600E mutation is the most common alteration, detected in our case, and it correlates with the pattern of disease (detected in most patients with high-risk disease, in 50% of multisystem disease without highrisk organ involvement, and in less than 20% of single-system disease) [2]. Besides, several studies have described excellent symptomatic and radiographic improvement of BRAF inhibitors like vemurafenib or dabrafenib [5]. The management of those without BRAF mutation depends on the extension of the disease, ranging from watch-and-wait to local and systemic therapies including chemotherapy (methotrexate + cytarabine, or claridibine) [5]. This pathology still supposes a great challenge specially when involvement of high-risk organs, reactivation and associated neurodegeneration, so this suggests the need for new lines of investigation.
Acknowledgement: We thank Jorge Cabezudo Pedrazo (Radiologist, Hospital Universitario de Fuenlabrada) for his work during the diagnosis
References
- Rodriguez-Galindo C, Allen CE. Langerhans cell histiocytosis. Blood. 2020; 135(16): 13191331. doi: 10.1182/blood.2019000934. PMID: 32106306.
- Rodriguez-Galindo C. Clinical features and treatment of Langerhans cell histiocytosis. Acta Paediatr. 2021; 110(11): 2892- 2902. doi: 10.1111/apa.16014. Epub 2021 Jul 7. PMID: 34192374.
- Astigarraga I, García-Obregón S, Pérez-Martínez A, Gutiérrez-Carrasco I, Santa-María V, Iturrate CR, Reggiori ML, Carrillo TM, Torrent M; Grupo de Histiocitosis de la Sociedad Española de Hematología y Oncología Pediátricas (SEHOP). Langerhans cell histiocytosis. Advances in pathogenesis and clinical practice. An Pediatr (Engl Ed). 2022; 97(2): 130. e1-130.e7. 10.1016/j.anpede.2022.05.005. Epub 2022 Jul 20. PMID: 35869015.
- Aissa S, Knaz A, Aissa A, Abdessayed N, Hayouni A. Adult Langerhans’ cell histiocytosis with multisystem bone and lung involvement: About a case. Tunis Med. 2022; 100(7): 561-563. PMID: 36571746; PMCID: PMC9703999.
- Go RS, Jacobsen E, Baiocchi R, Buhtoiarov I, Butler EB, Campbell PK, et al. Histiocytic Neoplasms, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2021; 19(11): 1277-1303. doi: 10.6004/jnccn.2021.0053. PMID: 34781268.
