
Open Access, Volume 9
Scoliosis correction surgery in a patient with unilateral pulmonary agenesis: A case report and review of literature
Youssef Khabir1*; Dan Wang1; Junwei Pan1; Xiaozong Duan1; Maher Al Hussan2
1Department of Orthopedic Surgery, First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, China.
2Department of General Surgery, First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, China.
Youssef Khabir
Department of Orthopedic Surgery, First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan,
China.
Email: josefkhabir@gmail.com
Received : Nov 16, 2023,
Accepted : Dec 11, 2023
Published : Dec 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Secondary scoliosis is caused by diseases wherein there is a lack of support for the spine, resulting in unequal pressures on the sides of the spinal cord. Secondary scoliosis is usually due to a neuromuscular disorder such as cerebral palsy, poliomyelitis, spina bifida, or a muscular dystrophy and is rarely secondary to pulmonary abnormalities. In this paper, we will specifically focus on the spine deformities associated with pulmonary diseases. We report a case of an adolescent female presenting with shoulder imbalance and marked scoliosis with a history of pulmonary agenesis. The patient underwent scoliosis correction surgery with instrumentation and fusion. Postoperatively, the patient showed improvement in the Cobb angle as well as marked improvement in her respiratory function. This review may raise awareness of the association between severe scoliosis and childhood lung absence and stimulate further prospective research efforts.
Keywords: Pulmonary agenesis; Secondary scoliosis; Absent right lung; Thoracogenic scoliosis; Pleural scoliosis; Post pneumonectomy like syndrome.
Abbreviations: VEPTR: Vertical Expandable Prosthetic Titanium Rib; TLSO: Thoracic-lumbo-sacral orthosis; IPP: Intrapleural pressure.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Khabir Y (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Khabir Y, Wang D, Pan J, Duan X, Maher Al H. Scoliosis correction surgery in a patient with unilateral pulmonary agenesis: A case report and review of literature. Open J Clin Med Case Rep. 2023; 2170.
Introduction
Congenital unilateral lung agenesis is a rare condition in which there is a complete absence of one lung. In addition to the associated bronchus and pulmonary vasculature, it is also associated with longterm progressive inadequacy of lung function due to poor lung growth. Unilateral pulmonary agenesis can be an isolated finding or present in conjunction with cardiac, gastrointestinal, genitourinary, and skeletal malformations [1]. In this case, the patient is not presented with any other congenital malformations; however, an imbalance in the left and right intrathoracic volume or lung pressure-volume compliance may be the root cause of the development of scoliosis. Major surgeries pose significant risks to patients with normal pulmonary function, let alone patients with half the lung function. Limited cases of scoliosis correction surgery performed on patients with unilateral pulmonary agenesis exist in the current literature. This report reviews her case in detail, as well as the scarce literature available regarding scoliosis secondary to pulmonary agenesis.
Case Presentation
A 15-year-old female came to our hospital complaining of shoulder imbalance, where the right side is higher than the left. She was diagnosed with scoliosis four years ago, and no sort of treatment was done. Her medical history was significant for congenital right lung agenesis with dextrocardia and left lung hyperinflation. She was symptomatic and could not tolerate normal daily physical activity. The severity of the spine curvature further exacerbated her pulmonary limitation, which led to her symptoms. Due to the patient’s concern over the appearance of her back and the long-term negative impact of signs and symptoms on her health, she was advised to undergo surgery. Considering all the risks related to the surgery and her medical history, the patient agreed to undergo the surgery, which was performed at the First Affiliated Hospital of Zhengzhou University. Before the surgery, due to her history of unilateral lung agenesis, she had to go through vast and thorough testing and laboratory investigations to determine if she could tolerate a major surgery. Physical examination revealed a tall, underweight girl with normal vital signs. Shortness of breath upon exertion with no other comorbidity or past surgical intervention. In addition, an electrocardiogram shows signs of tachycardia. Cardiac ultrasound revealed that the heart is on the right side with no signs of right lung parenchyma. Bronchoscopy showed that the larynx and vocal cords are normal, the trachea is twisted and deformed with no obstruction, and there is an abrupt ending of the right main bronchus at the Carina. The lung function test showed reduced total lung volume, reduced residual gas volume, reduced functional residual capacity, and decreased vital capacity. A chest X-ray performed at admission showed opacity on the right thorax, together with deviation of the trachea and mediastinum to the right. Scoliosis at the upper thoracic spine with a Cobb angle of 43.33 (Figure 1A). Chest computed tomography CT showed collapse of the right lung with respiratory dead spaces, compensatory hyperinflation, and herniation of the left lung to the opposite side. The heart and mediastinum are displaced so far to the right that they can easily be mistaken for situs inversus (FigURE 2A). After successful anesthesia, the surgical team proceeded with placing the patient on the prone side with adequate padding on both sides, leaving the abdomen hanging free. Next, a 25-cm skin incision is made from approximately the seventh cervical vertebra to the ninth thoracic. Then the underneath fascia is incised, the muscles are stripped until both facet joints are visible, and the laminae are fully exposed. With the help of a 3D-printed model of the patient’s spine, 17 trial screws left C7, left T2-T9 and right C7, right T2-T4, right T6-T9 were safely implanted, and correct placement was confirmed with fluoroscopy (Figure 1B). Instrumentation is then used to reduce the curvature of the spine. This involves placing permanent screws at each vertebral level mentioned above, and then a contoured rod is attached to these screws at each level and correction is performed. Left T1, right T1, and right T5 pedicles were particularly narrow, which made it difficult to place the screws (Figure 2B). Once the instrumentation was placed securely and a satisfactory correction was achieved, a final tightening was done. Lastly, the incision is washed, closed and dressed. Postoperatively, the patient was in good condition, with perfect vital signs and no pulmonary complications. Post-operative radiographs showed an improved Cobb angle of 17.8 degrees (Figure 1C), as well as marked improvement in her respiratory function, as evidenced by her ability to be extubated and resume activities of daily living. The patient was discharged 11 days after surgery and was advised to wear a thoracic-lumbo-sacral orthosis TLSO brace for 3 months and come for regular follow-ups.
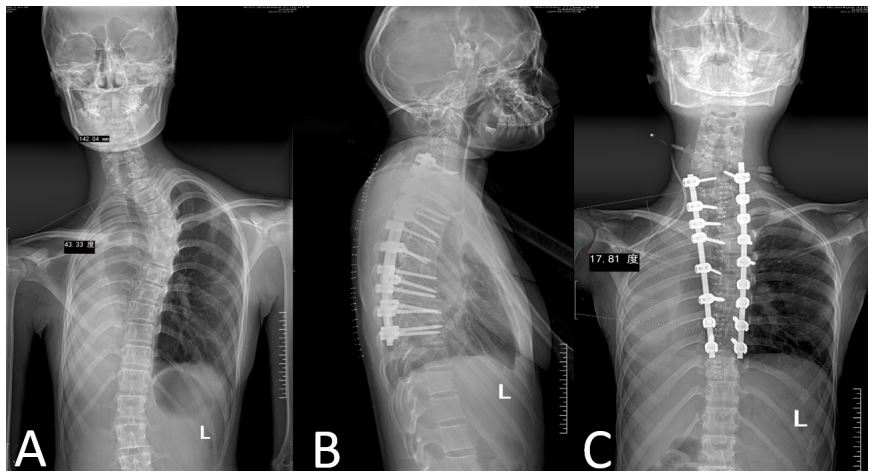
Figure 1: Chest Radiograph (A) showing homogenous opacity of the tight hemithorax with gross shifting of the
mediastinum to the left and scoliosis with convexity to the left. (B) Pedicle screws placement at each level. (C)
Postoperative radiograph show improved scoliosis Cobb angle and wider right intercostal spaces.
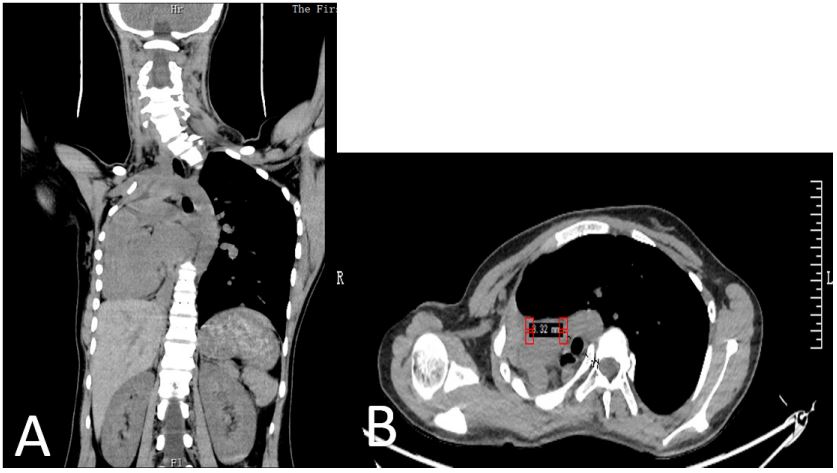
Figure 2: CT (A) show complete absence of the right lung with Dextrocardia. (B) CT axial cut at T5 show narrow
pedicle at the right side.
Table 1: Distribution of cases.
| Cases | Gender | Side of agenesis | Scoliosis development | gender | Side of agenesis |
|---|---|---|---|---|---|
| 58 isolated pulmonary agenesis cases |
• 28 F • 30 M |
13 L 15 R 10 L 20 R |
• Yes=46 • No=12 |
20 F 26 M 7 F 5 M |
15 L 31 R 8 L 4 R |
Discussion
Pulmonary agenesis is a rare malformation usually seen alone or in association with other anomalies [2]. The exact incidence and prevalence of lung agenesis are also unknown; however, recent literature has quoted an estimated incidence of 1.22 per 100,000 new births [3]. The deformity occurs either on one side or on both sides, with equal incidence between the right lung and left lung. Unilateral lung agenesis or lung absence is classified depending upon the stage of development of the primitive bud into three variants by [4]:
Type 1. Agenesis is complete absence of pulmonary parenchyma and bronchus and absence of the pulmonary artery on the affected side.
Type 2. Aplasia is complete absence of pulmonary parenchyma but with a rudimentary bronchus.
Type 3. Hypoplasia is variable amounts of pulmonary parenchyma, bronchi, and supporting vessels are present.
Our patient will be classified as type 1 with complete right lung absence, but aside from scoliosis, we could not find any other congenital anomaly. The Incidence and prevalence of scoliosis developing in patients with pulmonary agenesis are unknown due to the lack of enough cases to conduct cohort studies. Here we conducted a review of the preexisting literature to determine the incidence of developing scoliosis in patients with isolated lung agenesis. Cases of pulmonary agenesis were ascertained from the literature using past case reports and previous literature reviews. Each case was reviewed for the presence of scoliosis and other associated malformations. A total of 267 cases were extracted, including our case of pulmonary agenesis; there were more female affected. 87 with isolated lung agenesis were included, whereas [180] were excluded due to their association with other skeletal congenital abnormalities, which could be the cause of the scoliosis. Of the 87 included cases, another 29 were also excluded because of not enough details to confirm scoliosis. 12 (04 with right lung agenesis and 08 with left lung agenesis) cases did not develop scoliosis and the remaining 46 (31 with right lung agenesis and 15 with left lung agenesis) presented with marked scoliosis (Table 1). 79.31% of isolated pulmonary agenesis developed scoliosis at some point of their life. The youngest was 4 months old, and the oldest 65 was years old with a higher incidence in males. 88.57% of the right sided pulmonary agenesis developed scoliosis, whereas 65.21% of the left sided pulmonary agenesis developed scoliosis. This could be explained by the position of the heart on the left side, which substitutes the absent lung immediately without the decreases the severity of the mediastinal shift. It was observed that all the included cases showed the same scoliosis features; the curve was at the proximal thoracic spine. Right side involvement: the curve was convex towards the left side and vice versa, with crowding of the ribs on the affected side. The same features were observed in patients with post pneumonectomy syndrome, which is a complication that follows the removal of one lung especially in young patients. A study following 18 children who underwent pneumonectomy reported that scoliosis development is just a matter of time [5]. In addition, another study reported 90% mild scoliosis development high up in the thoracic spine with convexity towards the unoperated side after lung removal [6] Which is consistent with our scoliosis findings. Therefore, it is safe to conclude that pulmonary agenesis patients also suffer from post pneumonectomy like syndrome. The exact Pathogenesis of scoliosis development in post pneumonectomy syndrome or pneumonectomy like syndrome is unknown; however, we believe it is purely mechanical. Since the absence of one lung on one side leads to the absence of intrapleural pressure (IPP) on the same side. In addition, different studies suggested that an asymmetrical IPP distribution between a left and right hemithorax could induce forces via the rib cage, which cause displacement and rotation of the spine [7]. Most of the scoliosis cases in patients with pulmonary agenesis were managed conservatively. To our knowledge, our case is the first to be managed surgically with spinal instrumental fusion. Other documented surgical managements of scoliosis in patients with pulmonary agenesis are VEPTR expansion thoracoplasty, with an attempt to expand the constricted thorax rather than direct correction of the scoliosis alone, showed promising results in controlling the spinal deformity [8-10]. Thus, expansion thoracostomy and VEPTR insertion with serial lengthening can be considered early for the management of scoliosis. In addition, Cephalad translocation of diaphragm was also performed in a number of cases, but it failed to stop the development of scoliosis [11]. Several studies showed early post pneumonectomy syndrome can be management by mediastinal positioning and prosthetic implants [12-14]. Therefore scoliosis can be prevented and more invasive and expansive surgeries can be prevented. Shen et al., reported that [18] patients underwent pneumonectomy, and the empty space was filled with saline-filled breast prostheses showed no signs of scoliosis even after a long follow-up [15]. As with our case, other cases documenting surgical treatment for other conditions showed that lung agenesis patients are well compensated and pose no challenges during anesthesia [16-19]. However, anesthetic preoperative management should consist of a thorough survey of other systems, particularly the cardiovascular and renal systems. The patient should otherwise be managed like any other patient with a limited pulmonary reserve.
Conclusion
In summary, although scoliosis development in individuals with pulmonary agenesis is rare nonetheless it is inevitable and it could range from a balanced scoliosis with a very low risk of progression to an aggressive and rapidly progressive one. Therefore, scoliosis screening in patients who have lung agenesis is needed. Similar to post pneumonectomy syndrome following pneumonectomy, patients with post pneumonectomy-like syndrome can be successfully managed by early mediastinal positioning and prosthetic implants. More research with a longer follow period is necessary to determine the exact incidence, pathogenesis, risk factors, and prevention of scoliosis in patients with pulmonary agenesis.
Declarations
Ethics approval and consent to participate: No ethical committee approval was required for this case report by the Department, because this article does not contain any studies with human participants or animals.
Informed consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Data and materials: The data used to support the findings of this study are available from the corresponding author upon request.
References
- Maltz DL, Nadas AS. Agenesis of the lung. Presentation of eight new cases and review of the literature. Pediatrics 1968; 42: 175-88.
- Abbey P, Narula MK, Anand R. Congenital Malformations and Developmental Anomalies of the Lung. Curr Radiol Rep 2014; 2: 71. https://doi.org/10.1007/s40134-014-0071-y.
- Thomas M, Robertson N, Miller N, Rankin J, McKean M, Brodlie M. Congenital Lung Agenesis: Incidence and Outcome in the North of England. Birth Defects Res. 2017; 109: 857-9. https://doi.org/10.1002/bdr2.1011.
- Boyden EA. Developmental anomalies of the lungs. The American Journal of Surgery 1955; 89. https://doi.org/10.1016/0002-9610(55)90510-9.
- Kosar A, Orki A, Kiral H, Demirhan R, Arman B. Pneumonectomy in Children for Destroyed Lung: Evaluation of 18 Cases. Annals of Thoracic Surgery. 2010; 89. https://doi.org/10.1016/j.athoracsur.2009.10.007.
- Jacobsen S, Rosenklint A, Halkier E. Post-pneumonectomy scoliosis. Acta Orthop. 1974; 45. https://doi.org/10.3109/17453677408989697.
- Schlager B, Niemeyer F, Galbusera F, Wilke HJ. Asymmetrical intrapleural pressure distribution: a cause for scoliosis? A computational analysis. Eur J Appl Physiol. 2018; 118. https://doi.org/10.1007/s00421-018-3864-5.
- Emans JB, Caubet JF, Ordonez CL, Lee EY, Ciarlo M. The Treatment of Spine and Chest Wall Deformities With Fused Ribs by Expansion Thoracostomy and Insertion of Vertical Expandable Prosthetic Titanium Rib. Spine (Phila Pa 1976). 2005; 30: S58-68. https://doi.org/10.1097/01.brs.0000175194.31986.2f.
- Dayer R, Ceroni D, Lascombes P. Treatment of congenital thoracic scoliosis with associated rib fusions using VEPTR expansion thoracostomy: a surgical technique. European Spine Journal. 2014; 23: 424–31. https://doi.org/10.1007/s00586-014-3338-3.
- Campbell RM. Operative Strategies for Thoracic Insufficiency Syndrome by Vertical Expandable Prosthetic Titanium Rib Expansion Thoracoplasty. Oper Tech Orthop. 2005; 15: 315–25. https://doi.org/10.1053/j.oto.2005.08.008.
- Krivchenya DU, Dubrovin AG, Krivchenya TD, Khursin VN, Lysak CV. Aplasia of the right lung in a 4-year-old child: Surgical stabilization of the mediastinum by diaphragm translocation leading to complete recovery from respiratory distress syndrome. J Pediatr Surg. 2000; 35: 1499–502. https://doi.org/10.1053/jpsu.2000.16424.
- Nowotny T, Ahrens BC, Bittigau K, Buttenberg S, Hammer H, Kalache KD, et al. Right-sided pulmonary aplasia: Longitudinal lung function studies in two cases and comparison to results from term healthy neonates. Pediatr Pulmonol. 1998; 26: 138-44. https://doi.org/10.1002/(SICI)1099-0496(199808)26:2<138:: AID-PPUL12>3.0.CO;2-2.
- Furia S, Biban P, Benedetti M, Terzi A, Soffiati M, Calabrò F. Postpneumonectomy-Like Syndrome in an Infant With Right Lung Agenesis and Left Main Bronchus Hypoplasia. Ann Thorac Surg. 2009; 87: e43-5. https://doi.org/10.1016/j.athoracsur.2009.02.023.
- Agrawal Y, Patri S, Kalavakunta JK. Right Lung Agenesis with Tracheal Stenosis due to Complete Tracheal Rings and Postpneumonectomy Like Syndrome Treated with Tissue Expander Placement. Case Rep Pulmonol. 2016; 2016: 4397641. https://doi.org/10.1155/2016/4397641.
- Shen KR, Wain JC, Wright CD, Grillo HC, Mathisen DJ. Postpneumonectomy syndrome: Surgical management and long-term results. Journal of Thoracic and Cardiovascular Surgery. 2008; 135. https://doi.org/10.1016/j.jtcvs.2007.11.022.
- Yu Y, Zhu C, Qian X, Gao Y, Zhang Z. Adult patient with pulmonary agenesis: focusing on one-lung ventilation during general anesthesia. J Thorac Dis. 2016; 8: 124-9. https://doi.org/10.3978/j.issn.2072-1439.2016.01.23.
- Wang H. An adult case of isolated unilateral pulmonary agenesis under general anesthesia. Chin Med J (Engl) 2014: 789-90.
- Dutta D, Karlekar A, Saxena R. Agenesis of the lung. Ann Card Anaesth. 2013; 16: 151. https://doi.org/10.4103/0971-9784.109775.
- Babita G, Rashmi M, Deb K. Combined spinal epidural anesthesia for cesarean section in a patient with left lung agenesis. Int J Obstet Anesth. 2001; 10: 125-8. https://doi.org/10.1054/ijoa.2000.0811.
