
Open Access, Volume 9
Bilateral avascular necrosis of femoral heads after pelvic irradiation: A case report and systematic review
Şefika Arzu Ergen1; Ecem Demir1*; Şahin Dikmen1; Aykan Kargın2; İbrahim Adaletli2; İsmet Şahinler1
1IUC-Cerrahpaşa Faculty of Medicine, Department of Radiation Oncology, Turkey.
2IUC-Cerrahpaşa Faculty of Medicine, Department of Radiology, Turkey.
Ecem Demir
IUC-Cerrahpaşa Faculty of Medicine, Department of Radiation Oncology, Turkey.
Email: ergenarzu@yahoo.com
Received : Nov 09, 2023,
Accepted : Dec 06, 2023
Published : Dec 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
The development of radiation induced changes in bone is related to multiple factors such as total dose, per fraction dose, irradiated volume, bone structure and localization, patient age, and chemo-radiotherapy. It is known that chang-es in bone occur after 30-40 Gy. There are very few publications on this subject in the literature, mostly case reports. Therefore, there is no definite consensus about the pathogenesis, diagnosis, and treatment. In this report, a case of avascular necrosis of bilateral femoral heads after pelvic radiotherapy will be presented and the relevant literature will be reviewed.
Keywords: Avascular necrosis; Femoral head; Radiotherapy; Osteoradionecrosis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Demir E (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Ergen SA, Demir E, Dikmen S, Kargın A, Adaletli I, Şahinler I. Bilateral avascular necrosis of femoral heads after pelvic irradiation: A case report and systematic review. Open J Clin Med Case Rep. 2023; 2169.
Background
Avascular necrosis (AVN) or osteonecrosis of the femoral head is a condition that occurs as a result of disruption of physiological vascularization in the bone for various reasons and is most commonly seen in the femoral epiphysis [1]. Traumatic and non-traumatic causes play a role in its etiopathogenesis. In traumatic AVN, ischemia occurs when the vascular structure is damaged following fracture or luxation. The most common causes of non-traumatic AVN are steroid therapy and excessive alcohol use [2]. Other risk factors include Gaucher’s disease, systemic lupus erythematosus, organ transplantation, chronic renal failure, hyperlipidemia, and some hematological diseases. Less frequently, it may develop due to diabetes, radiation, and hyperuricemia [3]. In this report, we present an uncommon case of bilateral AVN in the femoral heads after pelvic irradiation in a 47-year-old female patient and discuss AVN treatment with the relevant literature.
Case Report
A 47-years-old woman with FIGO stage 3 C1 cervical cancer applied to our clinic in August 2019. She was treated with 50,4 Gy pelvic external beam radiotherapy (EBRT) using the volumetric arc therapy (VMAT) technique with chemotherapy (cisplatin, total 5 cycles of 40 mg/m2 /week). It was followed by 30 Gy intracavitary radiotherapy prescribed to HR-CTV (6 Gy per fraction; once a week). A complete response was achieved three months after. During regular follow-up, 12 months after treatment, the patient complained of pain in her hip and groin. The pain was intensified with movement. In her anamnesis, there was no previous history of trauma or fall. She was a non-smoker, non-diabetic, and non-obese (Body Mass Index: 23.8). She didn’t have any comorbidities. On physical examination, there was a bilateral limitation of motion in hip joints, but there was no visible swelling or redness. Also, the FABER test was positive. The magnetic resonance imaging (MRI) showed a crescent sign and a fissure with bone marrow edema on the bilateral femoral heads (Figure 1). In EBRT treatment plan, only 5% of the bilateral femoral head volume received a dose above 42 Gy. However, the maximum point doses of the right and left femoral heads were found to be 51.3 and 49.4 Gy, respectively. Coronal and axial plan dose distributions of the femur heads are shown in (Figure 2). Considering the patient’s radiotherapy history, imaging findings, and physical examination findings, the patient was diagnosed with bilateral AVN of the femoral head. She was referred to an orthopedic clinic and was advised to undergo bilateral hip arthroplasty. She refused the operation and received conservative NSID and physical therapy. The patient was completely relieved with rest and this regimen. Follow-up MRI at 3- months showed regression of the bone marrow edema on bilateral femoral heads, but the persistence of fissure lines was consistent with AVN. After 1- year, the patient was pain-free and had no difficulty in walking.
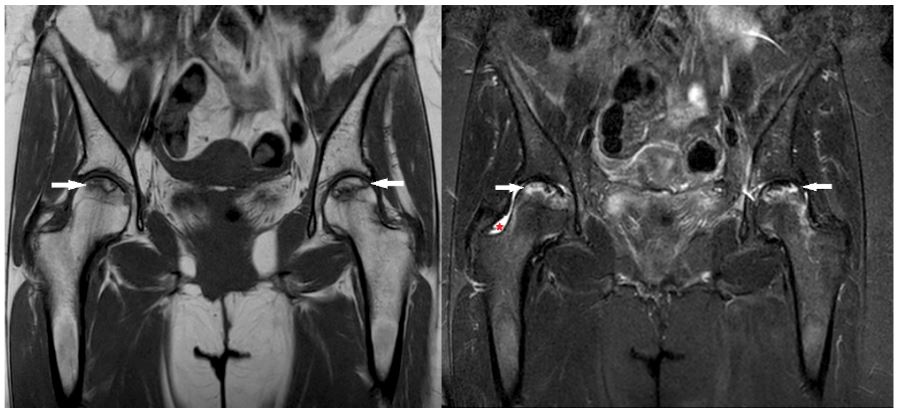
Figure 1: Coronal T1 weighted (left) and coronal STIR (Short tau inversion recovery) image (right). A serpiginous
area of altered signal intensity is seen in the subcortical area of bilateral femoral heads, showing central marrow
signal and ‘double line’ sign (white arrows on left and right). STIR images demonstrates accompanying mild bone
marrow edema surrounding the lesions. Note that mild joint effusion is present as well on the right hip (red arrowhead on right). No related sub-chondral collapse or flattening of femoral head is identified. Findings suggest
‘’stage II’’ avascular necrosis of both hips, according to the Ficat-Arlet classification.
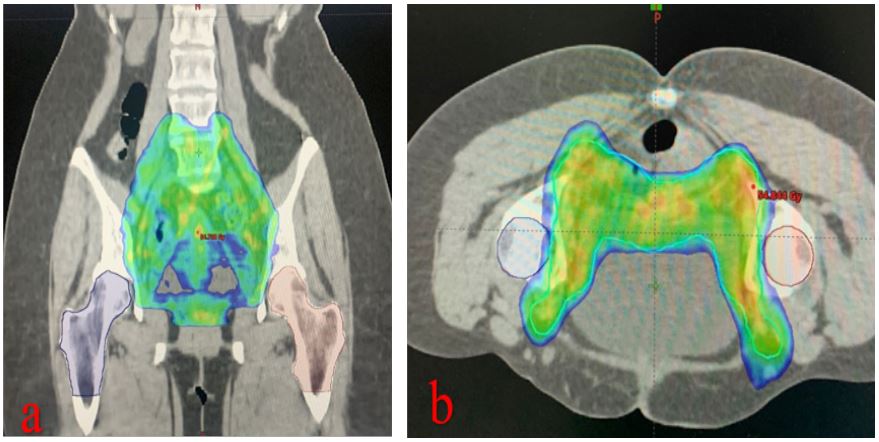
Figure 2: Dose distribution of 50,4 Gy around the femoral head area. (a) coronal plan (b) axial plan.
Table 1: Bilateral femoral head AVN cases after pelvic irradiation reported in the literature.
| Author | Year | N | Age | Gender |
Primer Disease location |
Total Dose | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| Nobier et al. (29) | 1984 | 1 | 53 | F | Cervix | -- | Conservative | Death |
| Csuka et al. (30) | 1987 | 1 | 73 | M | Prostate | -- | -- | -- |
|
Deleeuw and Pottenger (31) |
1988 | 2 | 63 | F | Cervix | 67 Gy |
L: THA R: Conservative |
Mild to moderate pain |
| 50 | M | Anal canal | 50 Gy | Bilateral THA | Conservative | |||
| Phillips et al. (32) | 1989 | 1 | 68 | F | Uterus | 50 Gy | Hip Replacement |
Condition Deteriorated |
| Jenkins et al. (4) | 1995 | 3 | 61 | F | Vulvar | 45 Gy | Bilateral THA | N/A |
| 59 | F | Vulvar | 45 Gy | Bilateral Hemiarthroplasty | N/A | |||
| 66 | F | Anal canal | 49,5 Gy |
L: THA R: Conservative |
N/A | |||
| Dhadda et al. (5) | 2006 | 1 | 41 | F | Cervix | 45 Gy | Bilateral THA | N/A |
|
Quinlan et al. (33) |
2009 | 1 | 67 | M | Urethta | 50 Gy | Bilateral hip arthroplasty | Walks well |
| Xu et al. (14) | 2021 | 1 | 83 | M | Prostate | -- |
L: THA R: Conservative |
L: Uneventful R: Motion limitation |
| Our case | 2023 | 1 | 47 | F | Cervix | 50,4 Gy | Conservative | No pain, walks wel |
M: male; F: female; Gy:gray; L:left; R:right; THA: Total Hip Arthroplas.
Table 2: Current staging systems used in the classification of osteonecrosis of the femoral head.
| ARCO classification criteria | Steinberg classification criteria | Ficat and arlet classification criteria | |
|---|---|---|---|
| Stage 0 | -- | Non-diagnostic imaging | -- |
| Stage I |
X-ray normal MRI: low signal intensity around necrosis |
X-ray normal, some changes
on MRI IA, IB, IC* |
Normal radiographic finds |
| Stage II |
Radiographs or CT scans show
focal osteoporosis or cystic changes in the femoral head but no evidence of subchondral fracture, necrotic fracture, or flattening of the femoral head |
sclerotic and cystic changes
in the femoral head IIA, IIB, IIC* |
Normal femoral head, Cysts
or osteosclerotic changes in some areas |
| Stage III |
Subchondral fracture image
on X-ray or CT |
Subchondral collapse
(crescent sign) without flattening IIIA, IIIB, IIIC* |
Subchondral collapse or
flattening of the femoral head |
| Stage IV |
Narrowing of the hip joint,
osteoarthritis, and acetabular changes on X-rays |
Flattening of femoral
head IVA, IVB, IVC* |
Degenerative changes are
seen in the acetabulum with narrowing of the joint space |
| Stage V | -- |
Joint space narrowing
and/or acetabular changes VA, VB,VC* |
-- |
| Stage VI | -- | Severe degenerative changes | -- |
• I-II-III-IV-VA: Mild (<%15 of femoral head
affected)*
• I-II-III-IV-VB-Moderate (%13 to %30 of femoral head
affected)*
• I-II-III-IV-VC: Severe (>%30 of femoral head
affected)*
Discussion
Radiation-induced AVN of the femoral head is uncommon but seriously a late toxicity that affects the patient’s quality of life. Depending on the radiotherapy technology and standards used, the incidence of pelvic AVN might range from 2.1 to 34% [4,5]. Bilateral femoral AVN cases reported after pelvic irradiation in the literature are even fewer. When we rewieved the literature for bilateral femoral head AVN in the last 40 years, we found 11 patient in 8 case reports published. We finally obtained a total of 12 patients’ information with our case (Table 1). Since it is so rarely seen, there is no definite consensus about its diagnosis and treatment.
When we investigate the pathophysiology, the mechanism of AVN formation is still not fully understood today. It is generally accepted that bones are relatively slow-proliferating tissues and relatively more resistant to ionizing radiation. However, higher radiotherapy doses have been shown to significantly increase the incidence of AVN [6]. This is owing to bone tissue’s high calcium concentration, which absorbs 40% greater radiation than surrounding tissue, making bones a typical location of radiation damage [7]. Although the risk of developing radiation-induced AVN is known to be low at doses below 50 Gy, there is no such thing as a safe or tolerable dose. Wang et al. suggested that V50 Gy <2% as tolerable dose constrain for prevention of AVN [8]. Several factors influence the likelihood of radiation-induced changes in bone, including fractionation, total treatment dose, dose intensity, and irradiated volume. Tolerance doses (TD5/5- TD50/5) that would not cause more than a 5% and 50% rate of serious complication rate within 5 years of irradiation have been reported between 20 to 30 Gy and 65 to 70 Gy for single and fractionated doses, respectively. The structure of the bone, its location, and the patient’s age are all important factors [9-10]. According to Bragga et al. [11] the threshold dosage for inducing osseous necrosis is 50 Gy. The femoral head had lower radiation tolerance than the long bones. According to current normal structural tolerance criteria, if the complete femoral head is exposed to 52 Gy, there is a 5% chance of AVN, which climbs to 50% with a dosage of 65 Gy [12]. With today’s advanced RT procedures and infrastructure, it is possible to reduce post-irradiation osseous damage to the hip joint by giving high doses to a compact volume and using protective shields that seal the head. When inguinal lymph nodes need to be irradiated, the femoral head is inevitably exposed to radiation doses that above the threshold, resulting in osteonecrosis [13]. Even though the frequency of post-irradiation AVN of the hip has significantly decreased in recent years, our patient still developed bilateral AVN requiring total hip arthroplasty. The effects of chemotherapy have been accepted as a possible cause of bone cell susceptibility to radiation damage; yet, the long-term effects of combination chemotherapy remain poorly known [14].
The gold standard in the diagnosis of AVN is the histologic demonstration of atrophy and cell damage in bone tissue. However, histologic examination is not essential and is not routinely performed in the clinic. The diagnosis is mostly based on several evaluations such as previous radiotherapy history, presence of clinical symptoms, physical examination and radiologic imaging findings [14]. The clinical presentation is usually progressive pain, stiffness, and crepitus. On physical examination, patients typically complain of limited range of motion and pain in the hip joint, particularly with difficulty in internal rotation [15]. Diseases affecting the hip joint and giving similar clinical symptoms, and bone metastases, especially in cancer patients, should be considered in the differential diagnosis. Since AVN and bone metastases show similar characteristics in conventional imaging, they are usually not sufficient for diagnosis. Computed tomography and magnetic resonance imaging examinations are generally preferred. The imaging findings vary according to the stage and size of the lesion. In the early period, an increase in density is observed in the affected area, cystic changes occur due to the resorption of dead bone tissue, and various degrees of collapse occurs in the bone [16]. Currently, there are several staging systems based on radiological findings (Table 2). The most well-known among these are the Association Research Circulation Osseous (ARCO) staging system, the Ficat and Arlet staging system, and the Steinberg staging system. The ARCO staging system is widely used in clinical practice because it is more systematic, comprehensive, practical, and more sensitive in diagnosis, predicting treatment efficacy and prognosis than other staging systems [17]. Recovery is possible if treatment is provided in early-stage disease (without collapse of the femoral head). However, if this process is not treated, it causes irreversible joint damage and losses affecting hip function [14]. Femoral head AVN treatment can be categorized into [2] different groups surgical and non-surgical methods. Nonsurgical treatments consist of pharmacological agents, and biophysical treatments; Surgical treatment includes joint sparing and joint replacement surgeries [14,18].
Medical management of radiation-induced AVN includes pentoxifylline, alpha-tocopherol, and bisphosphonates [19,20]. Pentoxifylline increases red blood cell elasticity and blood flow by dilating the vessels in damaged tissue. It is also believed that it reduces the cytokine cascade that promotes the progression of AVN with its anti-tumor necrosis factor activity [20]. Alpha-tocopherol increases the release of nitric oxide from endothelial cells, superoxide in neutrophils and macrophages, and can inhibit platelet aggregation [21]. At the same time, α-tocopherol is a weak antioxidant, it eliminates reactive oxygen species that play a role in the pathophysiology of AVN by inducing peroxidation in the cell membrane [23]. Studies have shown the efficacy of the combination of pentoxifylline and tocopherol in the treatment of body radiation injury compared to placebo and drug monotherapy [20,23]. Clodronate stimulates osteoblast’s function while inhibiting osteoclast activity, reducing the inflammatory expression and proliferation of fibroblasts. Ultimately reduces the incidence of collapse in osteonecrotic hips [24]. Biophysical therapies are hyperbaric oxygen (HBO) therapy, pulsed electromagnetic therapy, and extracorporeal shock wave therapy (ESWT). ESWT has been established to induce angiogenesis, restore oxygenation in tissues and reduce edema. It may be an alternative to invasive methods for early-stage AVN cases. It was also associated with both pain and functional improvement and observed a reduction in necrosis and bone marrow edema at follow-up [25,26]. HBO increases the extracellular oxygen concentration. It has been suggested that it reverses cellular ischemia and reduces the inflammatory response in symptomatic early-stage AVN. It is also expected to reduce edema by creating a high concentration of dissolved oxygen [27]. Conservative treatments are mostly used in early-stage patients. However, the efficacy of these treatments is limited and there are no clear recommendations for their use, and the level of evidence is low. The most common procedure in the early stage of the surgical treatment of AVN is core decompression; in advanced disease, total hip arthroplasty (THA) is performed [14,15,28]. In recent years, as new treatment strategies, stem cell therapy, which can help the bone formation and remodeling, has been tried. Also, cells believed to promote bone growth have been developed and new implants such as porous titanium rods are being used [2].
Conclusion
In conclusion, a case of bilateral femoral head AVN developed after RT for cervical cancer is presented. The etiology in this patient may have been the higher doses to which the femoral heads were exposed during radiotherapy. Although the effect of concomitant chemotherapy is unknown, the possibility of contribution should be considered. Currently, the RT dose threshold that poses no risk for AVN is unknown. It is also necessary to consider bone tissue among organs at risk (OAR) located in the irradiated field. Attention to dose distribution and the use of collimators during treatment planning allows the total dose delivered to the OAR to be reduced. The possibility that radiation-induced AVN is a stochastic effect should not be excluded who have received pelvic radiotherapy and it should be considered in every patient with a painful hip. Early detection of AVN is very important to start treatment before the collapse and to get successful results. It will also increase the quality of life by enabling surgical intervention in appropriate patients. Careful and prompt management and appropriate treatment can protect patients from longterm morbidities. Although AVN appears to be a relatively unusual adverse effect of radiotherapy, clinicians should be aware of it since it can cause substantial functional impairment in individuals who have been cancer-free for a long time.
Conflicts of Interest: There is no conflict of interest.
Informed consent: Written consent for publication was obtained from the patient.
Authors’ contributions: Şefika Arzu Ergen: Writing, editing, literature review. Ecem Demir: Editing, literature review. Şahin Dikmen: Writing, editing. Aykan Kargın: Radiological evaluation. İbrahim Adaletli: Radiological evaluation, research. İsmet Şahinler: Editing, discussion.
Acknowledgements: There is no acknowledgements.
References
- Kerachian MA, Harvey EJ, Cournoyer D, Chow TY, Séguin C. Avascular necrosis of the femoral head: vascular hypotheses. Endothelium. 2006; 13(4): 237-44.
- Petek D, Hannouche D, Suva D. Osteonecrosis of the femoral head: pathophysiology and current concepts of treat-ment. EFORT Open Rev. 2019; 4(3): 85-97.
- Guggenbuhl P, Robin F, Cadiou S, Albert JD. Etiology of avascular osteonecrosis of the femoral head. Morphologie. 2021; 105(349): 80-4.
- Jenkins P, Montefiore DS, Arnott S. Hip complications following chemoradiotherapy. Clinical Oncology. 1995; 7(2): 123-6.
- Dhadda A, Chan S. Bilateral avascular necrosis of the hips after chemoradiotherapy for cervical cancer. Clinical Oncology. 2006; 18(7): 576-7.
- Nicolay NH, Lopez Perez R, Debus J, Huber PE. Mesenchymal stem cells – A new hope for radiotherapy-induced tissue damage? Cancer Lett. 2015; 366(2): 133-40.
- Curi MM, Cardoso CL, de Lima HG, Kowalski LP, Martins MD. Histopathologic and Histomorphometric Analysis of Irradiation Injury in Bone and the Surrounding Soft Tissues of the Jaws. J Oral Maxillofac Surg. 2016; 74(1): 190-9.
- Bao Z, Wang D, Chen S, Chen M, Jiang D, Yang C, et al. Optimal dose limitation strategy for bone marrow sparing in intensitymodulated radiotherapy of cervical cancer. Radiat Oncol. 2019; 14(1): 118.
- Massin P, Duparc J. Total hip replacement in irradiated hips. A retrospective study of 71 cases. J Bone Joint Surg Br. 1995; 77(6): 847-52.
- Michalecki L, Gabryś D, Kulik R, Wydmański J, Trela K. Radiotherapy induced hip joint avascular necrosis-Two cases report. Rep Pract Oncol Radiother. 2011; 16(5): 198-201.
- Bragg DG, Shidnia H, Chu FC, Higinbotham NL. The clinical and radiographic aspects of radiation osteitis. Radiol-ogy. 1970; 97(1): 103-11.
- Emami B, Lyman J, Brown A, Coia L, Goitein M, Munzenrider JE, et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys. 1991; 21(1): 109-22.
- Nagi O, Chaudhary D, Kumar P, Rana N, Ojha MM, Mehrotra R. Radiation induced avn of hip joint following pelvic irradiation for endometrial carcinoma. EXECUTIVE EDITOR. 2018; 9(5): 274.
- Xu S-h, Tang J-s, Shen X-y, Niu Z-x, Xiao J-l. Osteoradionecrosis of the hip, a troublesome complication of radia-tion therapy: case series and systematic review. Frontiers in Medicine. 2022; 9.
- Konarski W, Poboży T, Śliwczyński A, Kotela I, Krakowiak J, Hordowicz M, et al. Avascular Necrosis of Femoral Head-Overview and Current State of the Art. Int J Environ Res Public Health. 2022; 19(12).
- Cohen-Rosenblum A, Cui Q. Osteonecrosis of the Femoral Head. Orthop Clin North Am. 2019; 50(2): 139-49.
- Zhao D, Zhang F, Wang B, Liu B, Li L, Kim SY, et al. Guidelines for clinical diagnosis and treatment of osteonecro-sis of the femoral head in adults (2019 version). J Orthop Translat. 2020; 21: 100-10.
- Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World J Orthop. 2015; 6(8): 590-601.
- Rivero JA, Shamji O, Kolokythas A. Osteoradionecrosis: a review of pathophysiology, prevention and pharmaco-logic management using pentoxifylline, α-tocopherol, and clodronate. Oral Surg Oral Med Oral Pathol Oral Radiol. 2017; 124(5): 464-71.
- Delanian S, Depondt J, Lefaix JL. Major healing of refractory mandible osteoradionecrosis after treatment combin-ing pentoxifylline and tocopherol: a phase II trial. Head Neck. 2005; 27(2): 114-23.
- Azzi A, Ricciarelli R, Zingg JM. Non-antioxidant molecular functions of alpha-tocopherol (vitamin E). FEBS Lett. 2002; 519(1-3): 8-10.
- Lyons A, Ghazali N. Osteoradionecrosis of the jaws: current understanding of its pathophysiology and treatment. Br J Oral Maxillofac Surg. 2008; 46(8): 653-60.
- Delanian S, Chatel C, Porcher R, Depondt J, Lefaix JL. Complete restoration of refractory mandibular osteoradi-onecrosis by prolonged treatment with a pentoxifylline-tocopherol-clodronate combination (PENTOCLO): a phase II trial. Int J Radiat Oncol Biol Phys. 2011; 80(3): 832-9.
- Fromigué O, Body JJ. Bisphosphonates influence the proliferation and the maturation of normal human osteo-blasts. J Endocrinol Invest. 2002; 25(6): 539-46.
- Alves EM, Angrisani AT, Santiago MB. The use of extracorporeal shock waves in the treatment of osteonecrosis of the femoral head: a systematic review. Clin Rheumatol. 2009; 28(11): 1247-51.
- Heller KD, Niethard FU. [Using extracorporeal shockwave therapy in orthopedics--a meta-analysis]. Z Orthop Ihre Grenzgeb. 1998;136(5):390-401.
- Pasquier D, Hoelscher T, Schmutz J, Dische S, Mathieu D, Baumann M, et al. Hyperbaric oxygen therapy in the treatment of radio-induced lesions in normal tissues: a literature review. Radiother Oncol. 2004;72(1):1-13.
- Malizos KN, Karantanas AH, Varitimidis SE, Dailiana ZH, Bargiotas K, Maris T. Osteonecrosis of the femoral head: etiology, imaging and treatment. Eur J Radiol. 2007; 63(1): 16-28.
- Nobler MP. Sarcoma and multi-systemic radionecroses following pelvic irradiation for epidermoid carcinoma of the cervix. Int J Radiat Oncol Biol Phys. 1984; 10(4): 580.
- Csuka M, Brewer BJ, Lynch KL, McCarty DJ. Osteonecrosis, fractures, and protrusio acetabuli secondary to x-irradiation therapy for prostatic carcinoma. J Rheumatol. 1987; 14(1): 165-70.
- Deleeuw HW, Pottenger LA. Osteonecrosis of the acetabulum following radiation therapy. A report of two cases. J Bone Joint Surg Am. 1988; 70(2): 293-9.
- Phillips T, Rao D. Destructive arthropathy of the hip following pelvic irradiation: report of four cases. Canadian Journal of surgery Journal Canadien de Chirurgie. 1989; 32(5): 353-7.
- Quinlan JF, North J, Clarke DA, Gwynne-Jones DP. Radiation-induced osteonecrosis of the hips following genital-preserving surgery and chemoradiotherapy. N Z Med J. 2009; 122(1297): 84-6.
