
Open Access, Volume 9
Spontaneous thrombosis of unruptured berry aneurysm presenting as facial palsy
Mohamed Rebayudeen*; Kulothungan; Gowtham Thomas
Department of Internal Medicine, Karpaga Vinayaga Institute of Medial Sciences and Research Centre, Tamil Nadu, India.
Mohamed Rebayudeen
Department of Internal Medicine, Karpaga Vinayaga Institute of Medial Sciences and Research Centre,
Tamil Nadu, India.
Email: rebayudeen@gmail.com
Received : Nov 06, 2023,
Accepted : Dec 04, 2023
Published : Dec 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Spontaneous thrombosis of saccular unruptured intracranial aneurysm (UIAs) is a known occurrence in giant aneurysms. However, spontaneous complete or partial thrombosis of non-giant aneurysms is a rare event in the natural history of UIAs that can be discovered incidentally on advanced neuroradiologic studies. They occasionally present with ischemic stroke, which is rare entity. Parent artery occlusion due to local extension of the luminal thrombus, aneurysms ejecting emboli to distal arteries, or increased mass effect have been described as possible pathogenic mechanisms. Guidelines for the management of these patients were limited. We present a documented case of this unusual entity a case of non-giant intracranial aneurysm with spontaneous thrombosis presenting as Upper motor neuron type of facial palsy due to acute ischemic stroke.
Keywords: Thrombosis; Aneurysm; Stroke; Upper motor neuron; Facial palsy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Rebayudeen M (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Rebayudeen M, Kulothungan, Thomas G. Spontaneous thrombosis of unruptured berry aneurysm presenting as facial palsy. Open J Clin Med Case Rep. 2023; 2168.
Introduction
Unruptured intracranial aneurysms (UIA) may be found incidentally since the diffusion of MRI and CT scan have increased their incidental diagnosis. Rarely saccular aneurysms may present with spontaneous partial or complete thrombosis and this can be symptomatic or asymptomatic. Spontaneous thrombosis is frequent in ruptured aneurysms, unruptured large and giant aneurysms. Spontaneous thrombosis of non–giant unruptured intracranial aneurysm (UIA) is otherwise rare. Among patients with UIA, the reported prevalence of ischemic stroke or transient ischemic attack is low (3-6.3%). We present a case of non-giant intracranial aneurysm with spontaneous thrombosis presenting as Upper motor neuron type of facial palsy due to acute ischemic stroke
Case Report
23 years old female came with complaints of deviation of angle of mouth towards right side for past 6 days associated with headache for 4 days for that she went to nearby hospital, treated it as Bell’s palsy. However, the deviation of angle of mouth and headache persisted so she came to our hospital. Patient had deviation of angle of mouth to right side more during eating and smiling associated mild drooling of saliva on left side present. Headache is also sudden onset and throbbing type for 4 days. There was no hyperacusis, speech and vision abnormalities. There was no history of vomiting, headache, seizures, dizziness, fever, recent vaccination, trauma to ear and ear discharge. No bowel & bladder incontinence. Patient conscious and oriented, afebrile. Her neurologic examination showed that rightward deviation of angle of mouth, left facial muscle weakness and loss of left nasolabial fold with preservation of left side forehead creases and ability to close her eyes on both side. Sensory and secretomotor motor functions intact on both side. All other cranial nerves were normal. No evidence of motor weakness, sensory impairment and cerebellar Signs.
MRI brain done along with MR Angiography-Showed a T2/FLAIR hyperintensity with diffusion restriction in DWI noted right frontal and right gangliocapsular region (Figure 1 marked in red arrow) along with partially thrombosed aneurysm of size 1.8 cm x 1.7 cm arising from M2 segment of Right middle cerebral artery (Figures 2 and 3). Then patient undergone 4 Vessel Doppler of neck and echocardiography, as it showed no evidence of thrombi. Then Serum homocysteine, serum ANA. APLA profile done. USG abdomen screening done for ADPKD. All investigations are within normal limits. So final diagnosis Spontaneous Thrombosis of Unruptured intracranial aneurysm causing acute infarct presenting as isolated Left UMN facial palsy. Neurosurgery opinion obtained as it was spontaneously thrombosed non giant intracranial aneurysm with acute infarction advised to start antiplatelet therapy and watch for any evidence of rupture. After 6-month follow-up, MRI taken aneurysm completely thrombosed and advised to continue antiplatelet therapy.
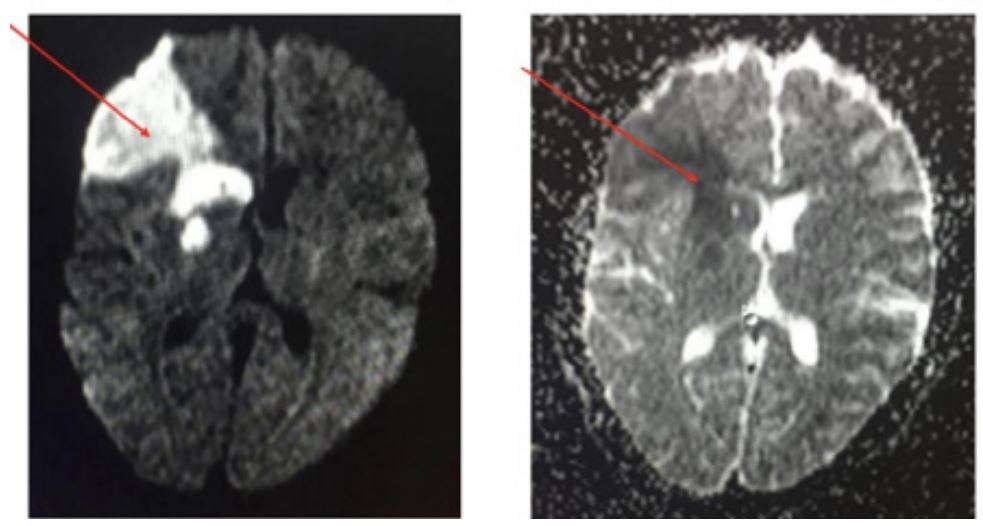
Figure 1: MRI brain done along with MR Angiography-Showed a T2/FLAIR hyperintensity with diffusion restriction in DWI noted right frontal and right gangliocapsular region (marked in red arrow).
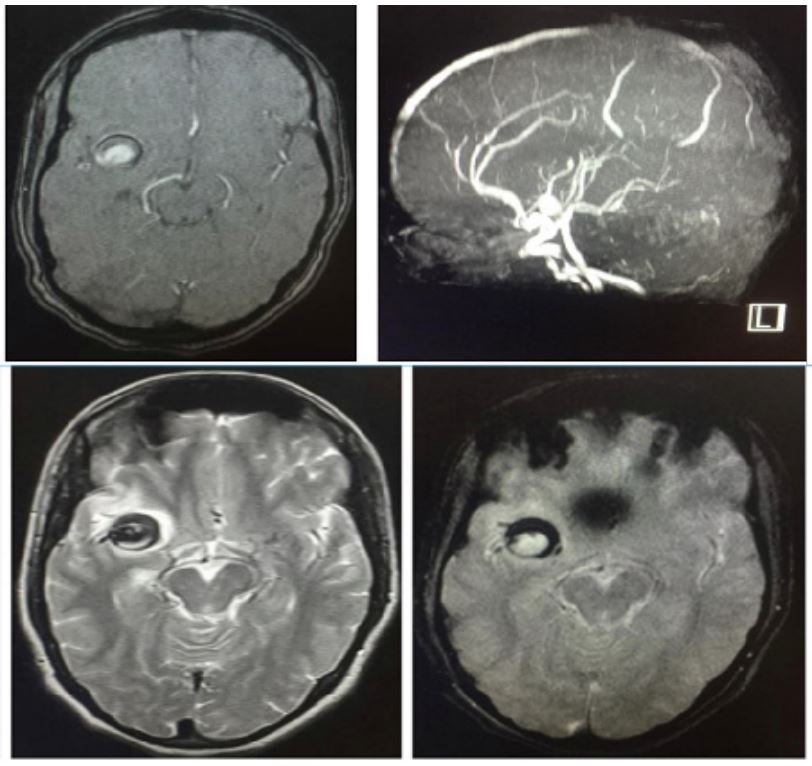
Figure 2 & 3: MRI Along with partially thrombosed aneurysm of size 1.8 cm x 1.7 cm arising from M2 segment of
right middle cerebral artery.
Discussion
Complete thrombosis of a cerebral aneurysm after rupture is a well-known event that can be related to hypotension, vasospasm and local damage to the arterial wall [1]. Spontaneous intra-aneurysmal thrombosis is also a well-documented phenomenon in large and giant aneurysms as up to 10-30% show partial thrombosis [2].
The prevalence of complete spontaneous thrombosis was higher in bigger aneurysms. Aneurysm’s size is a risk factor for spontaneous thrombosis. The occurrence of this phenomenon in non-giant saccular aneurysms has been rarely reported [3].
Both TIAs and ischemic strokes can be observed distal to unruptured aneurysms, presumably because of Parent artery occlusion due to local extension of the luminal thrombus, distal embolization, and increased mass effect have been implicated as possible pathogenic mechanisms [4]. Cerebral infarcts can be the first manifestation of spontaneous thrombosis of large or giant “UIAs. Most of the ischemic events were associated with aneurysms located in the middle cerebral artery or internal carotid artery due to higher flow rate and more shear forces may be contributing to embolization from the aneurysmal sac.
We found a prevalence Ischemic symptoms associated with intracranial aneurysms is 3.3% from multicenter review. The International Study of Unruptured Intracranial Aneurysms reported that 11% of patients with unruptured aneurysms presented with ischemic cerebrovascular disease [5]. When we reviewed the literature unruptured intracranial aneurysm with spontaneous thrombosis can present with various manifestations due cerebral infarction seen mostly in giant aneurysm, however our patient with spontaneous thrombosis of non-giant intracranial aneurysm presenting with isolated upper motor neuron type of facial palsy is extremely rare and very few cases reported till date.
There are clear guidelines for the management of thrombosed ruptured intracranial aneurysm. Whereas management of spontaneous thrombosis in non-ruptured intracranial aneurysm is limited. Based on size of the aneurysm whether surgical intervention or medical therapy might be selected.
Our patient had a partial thrombosis of non-giant UIA patient wants non-surgical intervention and requested medical management and willingness to adhere strict follow up. Antiplatelet treatments could be safely used in small UIAs use of aspirin or clopidogrel may reduce the risk of associated thromboembolic complications and also decrease aneurysmal growth rate and wall inflammation [6,7], aspirin seems to be a reasonable alternative for patients who are not good candidates for surgical resection of aneurysms [8]. While it should be avoided in thrombosed aneurysms larger than 20 mm. Spontaneous intra-aneurysmal thrombosis is associated with a higher risk of rupture in bigger aneurysms and therefore an early intervention is indicated. Complete intra-aneurysms thrombosis cannot be considered as a curative event, Aneurysm clipping may be beneficial because it decreases subarachnoid hemorrhage. However, given the risk of intraoperative thromboembolic events is higher. Elective coiling of UIA is another therapeutic alternative.
Conclusion
Ischemic stroke is a rare but serious complication of UIA. In this patients with confirmed spontaneous aneurysm thrombosis presented with isolated UMN facial palsy. During follow-up, no ischemic recurrences or subarachnoid hemorrhage were observed. For small aneurysms (≤15-20 mm) and aneurysms that are not amenable to surgery, aspirin may be used to reduce the risk of recurrent ischemic attacks.
Conflicts of Interest: No conflicts of interest.
References
- T. B. S. R. Brownlee RD. Spontaneous thrombosis of an unruptured anterior communicating artery aneurysm. Stroke, p. Stroke. 1995; 26: 1945-1949.
- J. P. B. K. Y.D. Cho. Endovascular treatment of largely thrombosed saccular aneurys ms : follow-up results in ten patients. Neuroradiology. 2010; 751-758.
- R. G. U. F. Cohen JE. Thrombosis and recanalization of symptomatic non-giant saccular aneurysm. Neurol Res. 2003; 25: 857-9.
- M. N. a. B. MW. Unruptured cerebral aneurysms presenting with ischemic events. Can J Neurol Sci. 2008; 35: 588-592.
- International Study of Unruptured Intracranial Aneurysms Investigators: Unruptured intracranial aneurysms: Risk of rupture and risks of surgical intervention. N Engl J Med. 1998; 339: 1725-1733.
- M. Y. Y. A. Qureshi AI. Ischemic events associated with unruptured intracranial aneurysms: multicenter clinical study and review of the literature. Neurosurgery. 2000; 46: 282-289.
- C. J. Antunes JL. Cerebral emboli from intracranial aneurysms. Surg Neurol. 1976; 6: 7-10.
- Nagashima M. Unruptured aneurysms associated with ischaemic cerebrovascular diseases. Surgical indication. Acta Neurochir (Wien). 124: 71-78.
