
Open Access, Volume 9
Outcome of high hip centre total hip replacement in a case of development dysplasia of hip: A case report
Sai Kiran Juttiga1; Sanjeev Kumar Singh1; Sudhanshu Shekhar2*; Harshit Pandey1
1Resident 3rd year, Rama Medical College Hospital, India.
2Orthopedics, Rama Medical College Hospital and Research Centre, Mandhana, Kanpur, Uttar Pradesh, India.
Sudhanshu Shekhar
Orthopedics, Rama Medical College Hospital and Research Centre, Mandhana, Kanpur, Uttar Pradesh,
India.
Email: docshekhar84@gmail.com
Received : Nov 03, 2023,
Accepted : Dec 01, 2023
Published : Dec 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Developmental dysplasia of the hip (DDH) is a common underlying condition leading to secondary osteoarthritis (OA) of the hip [1]. Treatment of DDH in an adult includes arthrodesis, excision arthroplasty, acetabulum and/or femoral osteotomy, and total hip replacement. Total hip arthroplasty (THA) is the last and definitive surgical treatment modality for end-stage developmental dysplasia of the hip. High hip center THR is needed in Crow types II, III, and IV. To achieve sufficient socket coverage by the native bone, high placement of cementless acetabular cups is often required.
Case report: A 40-year-old male patient presented to the OPD with complaints of pain in the left hip and difficulty in walking for 1 year. The patient had a history of fever and swelling over the left hip in childhood with no treatment taken for the same. X-ray of the pelvis with both hips showed a deformed femoral head, short neck, narrow femoral canal (Grade 1 Dorr), and arthritic changes in the acetabulum. We managed with total hip replacement using an orthopedic cone stem. Postoperatively, the patient has a good range of motion and has no difficulty in walking and weight-bearing. Functional outcome is excellent as per Harris hip score.
Conclusion: A higher hip center with the V-COR>23.9 mm was found to be a risk factor for dislocation after THA for DDH. Furthermore, advanced age, Crowe classification, and femoral head size were independent risk factors for dislocation. The higher hip center gained more bone coverage but decreased the range of flexion and IR. The high hip center was required to achieve sufficient bone coverage in patients with Crowe II and III hip dysplasia.
Keywords: Development dysplasia of the hip; Secondary osteoarthritis; Narrow femoral canal (Grade 1 Dorr); Total hip replacement; High hip center
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Shekar S (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Juttiga SK, Singh SK, Shekhar S, Pandey H. Outcome of high hip centre total hip replacement in a case of development dysplasia of hip: A case report. Open J Clin Med Case Rep. 2023; 2166.
Background
Development dysplasia of the hip causes a shallow acetabulum and deformed femoral head, which results in the early onset of secondary arthritis of the hip joint [1]. Its surgical treatment in adult include open reduction and acetabulum and/or femoral osteotomy, arthrodesis, excision arthroplasty, and total hip replacement which is the gold standard treatment for Crowe type II, III, IV. Developmental dysplasia of the hip (DDH) is a common underlying condition leading to secondary osteoarthritis (OA) of the hip [1]. Treatment of DDH in an adult includes arthrodesis, excision arthroplasty, acetabulum and/or femoral osteotomy, and total hip replacement. Total hip arthroplasty (THA) is the last and definitive surgical treatment modality for end-stage developmental dysplasia of the hip. In Crowe type II, III, and IV acetabulum roof has deficient bone stock so it is difficult to reconstruct the acetabular cup with a normal anatomical hip centre [2]. Bone grafting at the deficient site can be done to achieve a normal anatomical hip center but it results in reduced contact between acetabulum bone and the acetabulum component, causing loosening of the implant. High placement of the acetabulum component shows sufficient coverage by the native bone. Due to the acetabular morphology in DDH, including bone deficiency in the acetabular roof, it is frequently difficult to reconstruct the acetabular cup at the anatomical center in severe DDH to achieve sufficient bone coverage [2]. Morselized or structural bone grafting is one option for cup placement at the anatomical hip center. However, bone grafting may reduce the bone-implant contact that is essential for biological fixation, particularly with cementless acetabular cups. To avoid insufficient socket coverage by the native bone, high placement of a cementless acetabular cup is often required [3,4].
Doehring TC et all support a high hip center without superolateral cup placement, including heights of up to 37 mm from the normal anatomical hip centre [5]. Johnston RC et al. study shows that ac etaular reconstruction with anatomical hip centre reduces joint reaction force [6]. A higher hip center improved the bone coverage but decreased the range of flexion and internal rotation in THA due to bony or implant impingement. Here we are evaluating the outcome of the high hip center based on dislocation and range of motion. Factors determining dislocation are femoral head size, anteversion angle, age, V-COR, and Crowe stage.
Case Report
The patient Shiv Poojan, 40 year male, labourer by occupation has come to OPD with c/o- Limp since childhood. It is insidious in onset and gradually progresses. Limp is painless, associated with difficulty in squatting and cross-leg sitting, and not associated with any trauma, fever, night sweats, weight loss, or morning stiffness. There is no history of asthma, diabetes, hypertension, alcohol intake, or smoking. Local examination s/o flexion, adduction and internal rotation attitude and patient walks with bipedal unassisted Trendelenburg gait. Left ASIS is higher as compared to right, exaggerated lumber lordosis. There is an FFD of 20 degrees as confirmed by the Thomas test. On the squaring pelvis, there is a 20-degree ADD and 10-degree IR deformity. The movements at the hip were restricted in all planes, with no axis deviation. Left side 4 cm apparent shortening and 2 cm true shortening. 2 cm supratrochanteric shortening as confirmed by Bryant’s triangle, Nelaton line.
X-ray pelvis with hip ap view s/o-shallow acetabulum, pseudo acetabulum, subchondral sclerosis, deformed femoral head, reduced joint space, over-riding of GT, narrow femoral canal (Dorr type I) (Figure 1). Preoperative templating is done, it helps in knowing appropriate size of femoral and acetabulum component. The acetabulum and femoral bone stock are assessed by hip X-rays.
After clinical examination and thorough investigation patient is diagnosed as DDH left hip and is planned for THR left hip. After PAC clearance, the patient is shifted to OT, and total hip replacement is done by lateral approach (Figure 3a). TFL split, deep i/m plane made between gluteus medius and minimus. T-shaped incision given over capsule, femoral head dislocated. Femoral neck cut is done 1 finger proximal to LT and at a 45-degree angle. Bony osteophytes were excised (Figure 3b), and the acetabulum was reamed adjacent to the medial wall of the pelvis to maximize the bone coverage, appropriate size, angulation, and anteversion angle obtained. Acetabulum component 56 mm was inserted and fixed by a 6.5 CC screw of size 30 and 34 mm put in the posterosuperior quadrant. Femoral canal preparation was done using small rasps and broaches and appropriate size was obtained. The femoral component, uncemented, 135 degrees, size 9 mm and head of 36 mm inserted (Figure 4a-d). After implant placement, the movements at the hip joint in all planes were assessed and limb length was compared for no discrepancy. The wound was closed in layers and the patient was given an abduction bar to prevent dislocation.
Postoperative: The patient is put on antibiotics, analgesics, antiplatelet. Patient is ambulated with the help of a walker from POD 1. Quadricep and hip abductor strengthening exercises started from POD 1. Post op x-ray done on POD 1 (Figure 2). ROM exercises started from POD 5. Suture removed on POD 14. At present 3 months of follow-up, the patient is comfortable with no pain and difficulty in walking. The patient has a good hip range of motion (Figure 6). The functional outcome is good as per Harris’s hip score.
This is a case report study done at RAMA MEDICAL COLLEGE HOSPITAL after securing due approval from the institutional ethical committee. Informed written consent was taken from the patient in his language and the post-op complication was explained to the patient.

Figure 1: Pre-op x-ray of the pelvis with both hip AP view.
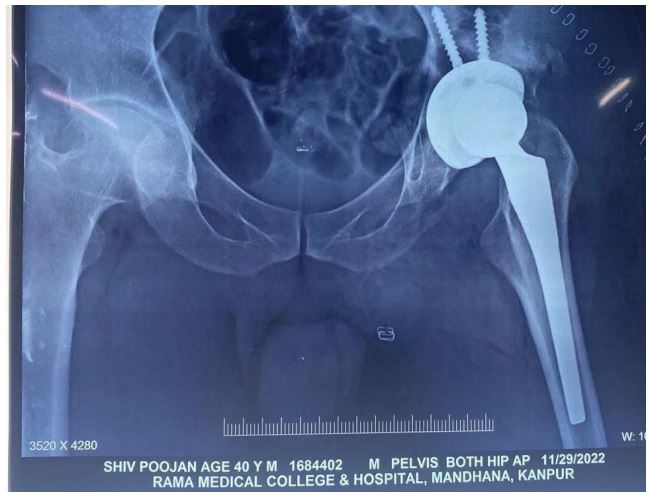
Figure 2: Post-op x-ray of the pelvis with both hip AP view.

Figure 3: Shows a superficial incision.

Figure 4a: Shows the femoral canal broaching.

Figure 4b: Shows femoral component insertion.

Figure 4c: Shows the acetabulum component.

Figure 4d: Shows osteophyte.

Figure 5: Showing post-op suture.
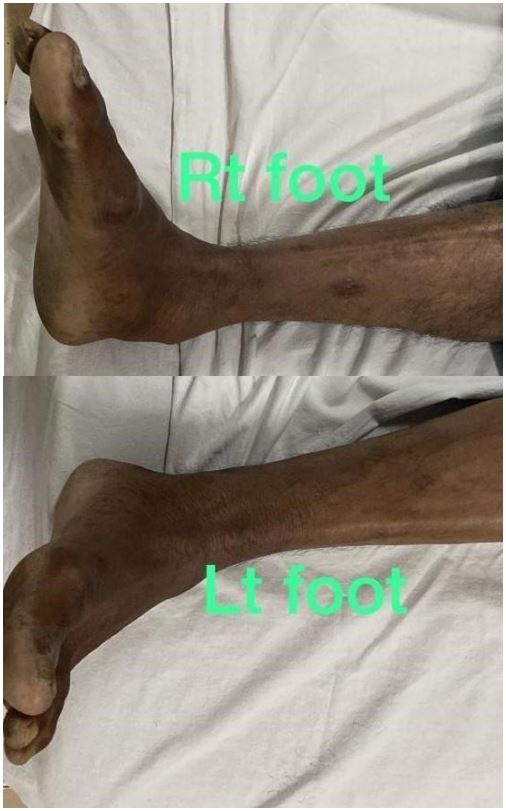
Figure 6: Post-op x-ray of the pelvis with both hip AP view.
Discussion
Hip dislocation is common in DDH [3]. Large femoral head size decreases dislocation. Wang et al. reported dislocation in 24 (2.93%) of 820 hips in patients with DDH [8]. A larger head size decreased the dislocation rate: 1.3% (7/535) with <28 mm and 0.5% (2/375) with ≥28 mm. In our case, the femoral head size is 36 mm. Hip dislocation also depends on the combined anteversion angle [7]. Akiyama et al. reported that the femoral anteversion in DDH ranged from − 13.2° to 58.2° with a significantly wider distribution of values than that in normal hips [9]. In our case, the combined anteversion angle is 50 degrees. Hip dislocation also depends on V-COR. With each increase of 5 mm in V-COR risk of dislocation increases by 3.1 times. Kaneuji et al. showed that the mean V-COR was 26.8±4.8mm (range, 20-35.9 mm), and there were no acetabular failures at a mean of 15 years [10]. Murayama et al. demonstrated that clinical and radiographic outcomes were excellent with placements of <35 mm from the interteardrop line [11]. In our case, VCOR is 26.4 mm. Hip dislocation also depends on the age of the patient [2]. Serious changes due to aging include changes in pelvic inclination and progressive decline in bone quality and muscle volume [12]. These phenomena related to aging could increase the risk of dislocation after THA. Regarding Hip dislocation also depends on Crowe classification [12]. Cameron et al. revealed that a high Crowe grade is correlated to a high chance of complications, such as nerve palsy, infection, and dislocation. Crowe classification can predict the complexity of surgery, with an increase in the Crowe grade making complications more common [13]. In our case, it’s Crowe type II. The higher hip center gained more bone coverage but decreased the range of flexion and IR. The high hip center was required to achieve sufficient bone coverage in patients with Crowe II and III hip dysplasia [14]. In our case range of flexion is 20 to 110 degrees and IR is 10 to 30 degrees.
Conclusion
Risk factors for dislocation after high hip center THA for DDH are high hip center >23.9, advanced age, high grade as per Crowe classification, and femoral head size. The higher hip center gained more bone coverage but decreased the range of flexion and IR.
Declarations
Ethics approval and consent to participate: This is a case report study done at RAMA MEDICAL COLLEGE HOSPITAL after securing due approval from the institutional ethical committee. Informed written consent was taken from the patient in his own language and the post op complication was explained to the patient.
Consent for publication: Consent for publication of clinical details and images of the patient taken.
Availablity of data and material: Not applicable.
Competing interest: No financial and non-financial competing interest.
Funding: No funding was obtained for this study.
Author contribution: HP helped in relevant literature search. SKS wrote intial draft. SKS and SS contributed in drafting of the manuscript. All authors have read and approved the final manuscript.
Acknowledgement: The authors offer thanks to the patient who participated in this case report study.
References
- Reijman M, Hazes JM, Pols HA, Koes BW, Bierma-Zeinstra SM Acetabular dysplasia predicts incident osteoarthritis of thehip: the Rotterdam study. Arthritis Rheum. 2005; 52(3): 787-793.
- Ganz R, Leunig M Morphological variations of residual hip dysplasia in the adult. Hip Int. 2007; 17(2): 22-28.
- Russotti GM, Harris WH Proximal placement of the acetabular component in total hip arthroplasty. A long-term follow-up study. J Bone Joint Surg Am. 1991; 73(4): 587-592.
- Komiyama K, Nakashima Y, HirataM, Hara D, Kohno Y, Iwamoto Y Does a high hip center decrease the range of motion in total hip arthroplasty? A computer simulation study. J Arthroplast. 2016; 31(10): 2342-2347.
- Doehring TC, Rubash HE, Shelley FJ, Schwendeman LJ, Donaldson TK, Navalgund YA Effect of superior and superolateral relocations of the hip center on hip joint forces – an experimental and analytical analysis. J Arthroplasty. 1996; 11(6): 693703
- Johnston RC, Brand RA, Crowninshield RD Reconstruction of the hip. A mathematical approach to determine optimum geometric relationships. J Bone Joint Surg Am. 1979; 61(5): 639-652.
- Nakashima Y, Hirata M, Akiyama M, Itokawa T, Yamamoto T, Motomura G, Ohishi M, Hamai S, Iwamoto Y Combined anteversion technique reduced the dislocation in cementless total hip arthroplasty. Int Orthop. 2014; 38(1): 27-32.
- Wang L, Trousdale RT, Ai S, An K-N, Dai K, Morrey BF Dislocation after total hip arthroplasty among patients with developmental dysplasia of the hip. J Arthroplast. 2012; 27(5): 764-769.
- Akiyama M,Nakashima Y, Fujii M, Sato T, Yamamoto T, Mawatari T, Motomura G, Matsuda S, Iwamoto Y Femoral anteversion is correlated with acetabular version and coverage in Asian women with anterior and global deficient subgroups of hip dysplasia: a CT study. Skelet Radiol. 2012; 41(11): 1411-1418.
- Kaneuji A, Sugimori T, Ichiseki T, Yamada K, Fukui K,Matsumoto T Minimum ten-year results of a porous acetabular component for Crowe I to III hip dysplasia using an elevated hip center. J Arthroplast. 2009; 24(2): 187-194.
- Murayama T, Ohnishi H, Okabe S, Tsurukami H, Mori T, Nakura N, Uchida S, Sakai A, Nakamura T 15-year comparison of cementless total hip arthroplasty with anatomical or high cup placement or Crowe I to III hip dysplasia. Orthopedics. 2012; 35(3): 313-318.
- Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y, Schneider SM, Topinkova E, Vandewoude M, Zamboni M Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010; 39(4): 412-423.
- Cameron HU, Botsford DJ, Park YS Influence of the Crowe rating on the outcome of total hip arthroplasty in congenital hip dysplasia. J Arthroplast. 1996; 11(5): 582-587.
- Komiyama K, Nakashima Y, Hirata M, Hara D, Kohno Y, Iwamoto Y. Does high hip center decreased range of motion in total hip arthroplasty? A computer simulation study. The Journal of Arthroplasty. 2016; 31(10): 2342-7.
