
Open Access, Volume 9
Right ventricle hypertrophy in fetuses diagnosed with Noonan syndrome: Can ductus venosus agenesis represent a contributing cause?
Gioia Mastromoro1*; Paolo Versacci2; Valentina D’Ambrosio3; Fiorenza Colloridi1; Alessandro De Luca4; Antonella Giancotti3; Antonio Pizzuti1,5; Flavia Ventriglia2
1Department of Experimental Medicine, Sapienza University of Rome, Policlinico Umberto I Hospital, Rome, Italy.
2Department of Pediatrics, Sapienza University of Rome, Policlinico Umberto I Hospital, Rome, Italy.
3Department of Gynecological, Obstetrical and Urological Sciences, Sapienza University of Rome, Policlinico Umberto I Hospital, Rome, Italy.
4Molecular Genetics Unit, Casa Sollievo della Sofferenza Hospital, IRCCS, San Giovanni Rotondo, Italy.
5Clinical Genomics Unit, Casa Sollievo della Sofferenza Hospital, IRCCS, San Giovanni Rotondo, Italy.
Gioia Mastromoro
Department of Experimental Medicine, Sapienza University of Rome, Policlinico Umberto I Hospital,
Rome, Italy.
Email: mastromorogioia@gmail.com
Received : Nov 07, 2023,
Accepted : Dec 01, 2023
Published : Dec 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Noonan syndrome (NS) is the most common genetic syndrome in fetuses with increased nuchal translucency (NT) and normal karyotype. NS patients present typical patterns of cardiac defects, such as pulmonary stenosis, polyvalvular dysplasia and hypertrophic cardiomyopathy. This study aims to evaluate onset and trend of cardiac disease in fetuses with molecular diagnosis of NS and to search for other cardiovascular sonographic markers of NS. We performed a fetal echocardiographic follow-up of pregnancies with increased NT in the first trimester. All the fetuses with normal Karyotype and Comparative Genomic Hybridizationarray underwent a targeted next-generation sequencing panel for RASopathies. Increased NT was the only finding up to the second trimester in half of the fetuses, while in the others ductus venosus agenesis was also observed. In all of them, during the late second trimester, a severe cardiopathy arouse.
In conclusion, when abnormal NT is detected in the first trimester, even if the second trimester fetal echocardiogram is normal, further ultrasound follow-up is mandatory, due to late onset of cardiac findings in NS. Ductus venosus agenesis, as well as increased NT, should be considered a marker for RASopathies and it might require investigations for late-onset cardiopathy and for NS.
Keywords: Prenatal diagnosis; Ductus venusus agenesis; Noonan syndrome; Cardiomyopathy; Increased nuchal translucency.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Mastromoro G (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Mastromoro G, Versacci P, D’Ambrosio V, Colloridi F, Alessandro DL, Giancotti A, Pizzuti A, et al. Right ventricle hypertrophy in fetuses diagnosed with Noonan syndrome: Can ductus venosus agenesis represent a contributing cause?. Open J Clin Med Case Rep. 2023; 2165.
Introduction
Noonan syndrome (NS) is the most common genetic syndrome found in fetuses with increased nuchal translucency (iNT) and normal Karyotype, with a frequency up to 10% [1,2]. Typical NS cardiac defects include pulmonary valvular/supra-valvular stenosis, polyvalvular dysplasia and hypertrophic cardiomyopathy (hCMP).
The rapid evolution of molecular genetics and imaging has resulted in a substantial increase in knowledge about development of congenital heart diseases, especially in genetic syndromes. Nowadays, more attention is given to prenatal ultrasound evaluations because of the importance of early diagnosis, which can influence the outcome. However, the mechanisms for development of cardiomyopathy in NS patients are still not elucidated, and an improvement of knowledge of the involved pathway could increase the possibility of target therapies. Here, we describe the late-onset appearance of severe cardiopathy in four pregnancies presenting with iNT in the first trimester, normal echocardiography during the early second trimester and a molecular diagnosis of NS.
This is the first study that aims to highlight and describe both onset and worsening of heart disease in NS fetuses, in order to reach an early diagnosis that can facilitate the postnatal therapeutic planning, and to evaluate additional sonographic markers for RASopathies.
Case Presentation
During the last 4 years, 3500 women were referred to the Department of Gynecology and Obstetrics for I trimester ultrasound evaluation, performed using a Samsung Echography WS80 Elite. NT scan was measured between 11 and 3 days and 13 weeks and 6 days of pregnancy or when crown-rump length is between 45 mm and 84 mm. Seven hundreds of the fetuses showed iNT. All the fetuses, who showed normal karyotype and CGH-array, underwent a targeted next-generation sequencing (NGS) panel for RASopathies. We performed a fetal echocardiographic follow-up of these pregnancies, selecting the four cases of the eleven NS fetuses that have come to birth, in order to describe the trend of the cardiopathy during last trimester, too. All the echocardiograms were performed using 3d convex 4,8 MHz of a Samsung Echocardiography Accuvix A30 and then retrospectively reviewed. Here, we report the late-onset appearance of cardiopathy in 4 fetuses with iNT and molecular diagnosis of NS (Table 1) (Figure 1). Ductus venosus agenesis (DVA) was observed in two fetuses, as in 27% of NS pregnancies [1].
Table 1: Late-onset appearance of cardiopathy in 4 fetuses with iNT and molecular diagnosis of NS.
| II trim Fetal Ecocardiography | III Trim Fetal Ecocardiography | Delivery | Postnatal Echocardiography |
|---|---|---|---|
|
Mild interventricular
septum hypertrophy |
Interventricular septum and RV hypertrophy | CS | Obstructive hCMP, PV stenosis, ASD |
| Reduced aortic annulus | Polyvalvular dysplasia, LVOTO | CS | CoA, hCMP, polyvalvular dysplasia |
| Normal | Polyvalvular dysplasia | eutocic |
Polyvalvular dysplasia,
hCMP, PV stenosis, supravalvular aortic stenosis |
| Normal | Hypertrophic obstructive CMP | eutocic | Polyvalvular dysplasia, hCMP, PV stenosis |
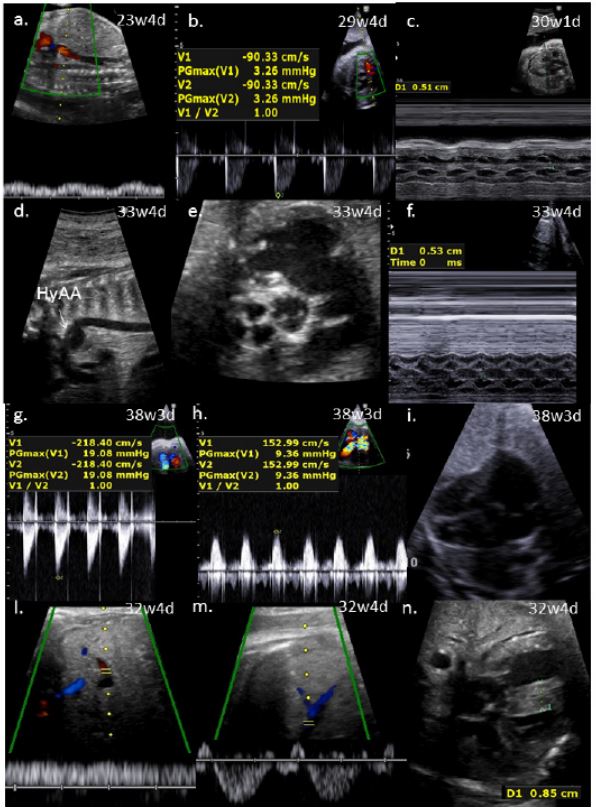
Figure 1: Prenatal ultrasound findings in the 4 fetuses with NS.
Case 1 a: Ductus venosus was not detectable. b. Doppler velocity in the main pulmonary artery was at the top of the normal range. c. Interventricular septum was thickened.
Case 2 d: Hypoplasia of aortic arch (HyAA). e. Semilunar valves were thickened and pulmonary valve (PA) seemed to be bicuspid. f. Interventricular septum was thickened.
Case 3: g.h. Doppler velocity was increased in both pulmonary artery and aorta because of the obstruction of the outlets. i. Redundant foramen ovale flap.
Case 4 l.m. Umbilical and sovrahepatic veins. Ductus venosus was not detectable. n. Interventricular septum was thickened.
Case 1 a: Ductus venosus was not detectable. b. Doppler velocity in the main pulmonary artery was at the top of the normal range. c. Interventricular septum was thickened.
Case 2 d: Hypoplasia of aortic arch (HyAA). e. Semilunar valves were thickened and pulmonary valve (PA) seemed to be bicuspid. f. Interventricular septum was thickened.
Case 3: g.h. Doppler velocity was increased in both pulmonary artery and aorta because of the obstruction of the outlets. i. Redundant foramen ovale flap.
Case 4 l.m. Umbilical and sovrahepatic veins. Ductus venosus was not detectable. n. Interventricular septum was thickened.
Discussion
Obstruction of lymphatic drainage is frequent in NS [3], which could be prenatally detected as iNT, cystic hygroma, hydrops or pleural effusions [4]. In the current series of NS fetuses iNT was the only feature and the survey of the cardiac morphology was normal up to the second trimester, only to witness the appearance of severe cardiopathies in the second part of the pregnancy and their postnatal worsening. Actually, in two of the four cases DVA added to the clinical picture
Ductus venosus connects the intra-abdominal umbilical vein to inferior vena cava at its inlet to the heart. The portocaval pressure gradient causes well-oxygenated blood in the ductus to accelerate towards the left lateral wall of inferior vena cava. When the umbilical vein reaches the liver, the ductus venosus branched off into a venous network, decreasing the blood pressure, before it continues itself in inferior vena cava. Fetuses with DVA and aberrant insertion of the umbilical vein, bypassing the liver network, present additional risks of developing congestive heart failure [5,6]. The mechanism responsible for triggering heart failure might be the increased cardiac preload and progressive cardiac decompensation [3]. In the NS fetuses with DVA we analyzed, the umbilical vein threw itself in the iliac vein, so we hypothesize that the increased intracaval and intracardiac pressure gradient could stimulate the right heart chambers to the hypertrophy [7]. In these cases, pulmonary stenosis could be worsened to limit flows in pulmonary artery. Moreover, fetuses with DVA could have a vulnerability in hypoxemic states and it can be also the primary cause of fetal hypoxia as the obstruction of the placental venous flow return can result in placental edema and impaired gas exchange. This edema reduces materno-fetal transfer of proteins and it may contribute to a decrease in fetal plasma protein levels, that can cause hydrops [8], frequent in NS fetuses.
The cardiopathies observed during third trimester in the present series were not detectable in the early pregnancy and it leads us to think that the absence of NS cardiac features at 20 weeks should not preclude genetic testing when markers are present. Therefore, if iNT is detected in a fetus at 12 GA, a further fetal echocardiogram should be offered in the third trimester, even if the second trimester fetal echocardiogram is normal. Three out of the 4 fetuses developed hCMP and the fetuses presenting with DVA showed a higher grade of right ventricular hypertrophy. This observation prompted us to consider DVA a contributing cause of biventricular hypertrophy
DVA should be considered a marker for RASopathies and for biventricular hypertrophy, requiring investigations for late-onset cardiopathy and NS, even if it could be suitable to validate a larger number of observations. Fetuses with prenatal diagnosis of NS need a close sonographic follow-up to control the cardiac status and to detect hCMP or polyvalvular dysplasia that could gradually arise. The absence of typical cardiac features of NS at 20 weeks should not preclude genetic testing when other markers are present. DVA should be noted, as it can represent a contributing cause of biventricular hypertrophy.
References
- Vigneswaran T V, Homfray T, Allan LD, et al. Persistently elevated nuchal translucency and the fetal heart. J Matern Neonatal Med. 2017; 4: 1-5.
- Mastromoro G, Guadagnolo D, Khaleghi Hashemian N, Bernardini L, Giancotti A, Piacentini G, et al. A Pain in the Neck: Lessons Learnt from Genetic Testing in Fetuses Detected with Nuchal Fluid Collections, Increased Nuchal Translucency versus Cystic Hygroma-Systematic Review of the Literature, Meta-Analysis and Case Series. Diagnostics (Basel). 2022; 13(1): 48.
- Joyce S, Gordon K, Brice G, Ostergaard P, Nagaraja R, Short J, et al. The lymphatic phenotype in Noonan and Cardiofaciocutaneous syndrome. Eur J Hum Genet. 2016; 24(5): 690-6.
- Myers A, Bernstein JA, Brennan ML, Curry C, Esplin ED, Fisher J, et al. Perinatal features of the RASopathies: Noonan syndrome, Cardiofaciocutaneous syndrome and Costello syndrome. Am J Med Genet Part A. 2014; 164(11): 2814-21.
- Berg C, Kamil D, Geipel A, et al. Absence of ductus venosus – importance of umbilical venous drainage site. Ultrasound Obs Gynecol. 2006; 28: 275-81.
- Contratti G, Banzi C, Ghi T, et al. Absence of the ductus venosus: report of 10 new cases and review of the literature. Ultrasound Obstet Gynecol. 2001; 18(6): 605-9.
- Mastromoro G, Pizzuti A, Ventriglia F. Role of ductus venosus agenesis in right ventricle development. J Matern Fetal Neonatal Med. 2020:1-4.
- Sivén M, Ley D, Hägerstrand I, Svenningsen N. Agenesis of the ductus venosus and its correlation to hydrops fetalis and the fetal hepatic circulation: case reports and review of the literature. Pediatr Pathol Lab Med. 1995; 15(1): 39-50.
