
Open Access, Volume 9
Cyclin-dependent kinase 4/6 inhibitors - Ribociclib - Induced ILD/Pneumonitis - The importance of early diagnosis: A case report
Danijela Niciforovic1*; Dragica Pavlovic2; Dragana Papic2; Katarina Milojevic1; Marija Spasojevic3; Sanja Milojevic4; Jasmina Nedovic1; Marina Markovic1,5
1Center for Internal Oncology, University Clinical Center Kragujevac, 34000 Kragujevac, Serbia.
2Department of Genetics, Faculty of Medical Sciences, University of Kragujevac, 69 Svetozar Markovic Street. 34000 Kragujevac, Serbia.
3Department of Pathological Anatomy, University Clinical Center Kragujevac, 34000 Kragujevac, Serbia.
4Department of Radiology, University Clinical Center Kragujevac, 34000 Kragujevac, Serbia.
5Department of Internal Medicine, Faculty of Medical Sciences, University of Kragujevac, 34000 Kragujevac, Serbia.
Danijela Niciforovic
Center for Internal Oncology, University Clinical Center Kragujevac, 34000 Kragujevac, Serbia.
Email: drmed.danijela.niciforovic@gmail.com
Received : Oct 25, 2023,
Accepted : Nov 23, 2023
Published : Nov 30, 2023,
Archived : www.jclinmedcasereports.com
Abstract
CDK4/6 inhibitors have demonstrated significant clinical activity in cancer patients. CDK4/6 inhibitors (palbociclib, ribociclib, and abemaciclib) and endocrine therapy have been approved for the treatment of advanced breast cancer in patients with HR+ and HER2-negative (HER2-) subtypes. The canonical mechanism underlying the activity of CDK4/6 inhibitors is the inhibition of retinoblastoma tumor suppressor protein phosphorylation, which prevents cancer cell proliferation. Common CDK4/6 inhibitors used to treat breast cancer include palbociclib, ribociclib, and abemaciclib, and have been utilized with great success in the treatment of hormone receptor-positive breast cancers and are undertaking testing for numerous other types of tumors. CDK4/6 inhibitors may induce nausea, vomiting, diarrhea, fatigue, alopecia, and myelosuppression symptoms such as leukopenia, neutropenia, and thrombocytopenia mucositis, hepatic toxicities (transaminitis), and cardiotoxicity (QTc prolongation, arrhythmias, novel hypertension, atrial fibrillation, myocardial infarction, pericardial effusion, cardiac failure). Despite a favorable toxicity profile in pivotal studies, increased rates of use in clinical practice may be associated with rare but fatal toxicity, such as pulmonary injury. The FDA has issued a warning regarding a rare but severe pulmonary inflammation that may be caused by the use of CDK4/6 inhibition in advanced breast cancer patients. This article displays a rare case of ribociclib-induced ILD/pneumonitis in a 53-year-old female with metastatic breast cancer
Keywords: Ribociclib; CDK4/6 inhibitors; ILD/Pneumonitis; Breast cancer.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Niciforovic D (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Niciforovic D, Pavlovic D, Papic D, Milojevic K, Spasojevic M, Milojevic S, Nedovic J, et al. Cyclin-dependent kinase 4/6 inhibitors - Ribociclib - Induced ILD/Pneumonitis - The importance of early diagnosis: A case report. Open J Clin Med Case Rep. 2023; 2162.
Introduction
Cyclin-dependent kinase 4/6 (CDK4/6) inhibitors have been a significant advance in the treatment of hormone receptor-positive, HER2-negative metastatic breast cancer, leading to the approval of three different CDK4/6 inhibitors (palbociclib, ribociclib, and abemaciclib) in both first- and second-line indications [1-5,9]. In spite of the studies demonstrating that CDK4/6 inhibitors may induce adverse events [4,6-8,10], there are numerous studies that showed beneficial effect of CDK4/6 inhibitors in breast cancer patients. Recently, it has been demonstrated in phase III clinical trials that these medications prolong overall survival (OS) in this population. According to the results of the MONALEESA-2 clinical study, the combination of ribociclib and letrozole significantly improved the OS of patients who were sensitive to endocrine therapy. The mortality risk was reduced by 24%, and the median survival time was determined to be 63.9 months [12]. The OS advantage was confirmed through statistical analysis in the endocrine-sensitive group of the MONALEESA 3 trial, in which ribociclib and fulvestrant were administered as the initial treatment [13]. In the MONALEESA 7 clinical trial, pre- and perimenopausal patients who received ribociclib in combination with endocrine therapy (aromatase inhibitors or tamoxifen) and goserelin demonstrated a comparable reduction in mortality risk [14]. In the MONARCH 3 clinical trial involving postmenopausal women with endocrine-sensitive diseases, the combination of abemaciclib and AI resulted in an overall response rate of 61% and a mean response duration of 32.7 months [15].
Most common adverse events of CDK4/6 inhibitors: In terms of safety, CDK4/6 inhibitors are generally well-tolerated agents with comparable safety profiles. However, the occurrence and frequency of toxicities vary among them, which may influence the selection of a particular medication [7,16]. Abemaciclib is structurally distinct from other CDK4/6 inhibitors and is more selective for CDK4 than CDK6. It is 14 times more potent against CDK4 than it is against CDK6. CDK4 is more essential for breast tumorigenesis than CDK6, which is linked to hematopoietic stem cell differentiation [17]. Mucositis, nausea, vomiting, diarrhea, fatigue, alopecia, and infections may be caused by CDK4/6 inhibitors, whereas ribociclib and palbociclib mitigate these side effects [6]. Abemaciclib, the most potent of the three CDK4/6 inhibitors, is more likely to cause diarrhea because of its higher potency against CDK4 than CDK6, which may also account for its lower hematological toxicity [18]. Therefore, ribociclib and palbociclib have a toxicity profile characterized by hematological adverse events, with neutropenia and thrombocytopenia being the most frequently reported adverse events [19,20]. The addition of CDK4/6 inhibitors to ET significantly enhanced the risk of infections of all grades, infections of grade 3 or higher, and urinary tract infections [21]. In addition, ribociclib is associated with a higher frequency of QT interval prolongation and elevated liver enzymes [19]. Each of the three CDK4/6 inhibitors — palbociclib, abemaciclib, and ribociclib — is FDA-approved and supported by significant clinical trials: PALOMA-1, MONARCH-1,2,3 [6,16], and MONALEESA-2 [12,20,22]. In the MONALEESA-2 trial, two patients who received ribociclib plus letrozole succumbed to acute respiratory failure [23]. Since the trial’s publication, one case of ribociclib-induced pulmonary toxicity has been reported. On the other CDK 4/6 inhibitors, palbociclib and abemaciclib, the scientific literature contains similar evidence. There are three published case reports of palbociclib-induced pneumonitis, two of which improved after drug discontinuation, and one case report of abemaciclib-associated lung injury [24]. Recently, the Japanese Ministry of Health issued a warning after four patients developed pulmonary toxicity, likely as a result of abemaciclib exposure, with one patient dying [25]. In this article, we present a case of ribociclib-induced ILD/pneumonitis in a 53-year-old female with metastatic breast cancer
Case Presentation
Here, we describe a female patient with metastatic hormone receptor-positive/human epidermal growth factor 2-negative breast cancer who developed pneumonitis during four weeks on ribociclib.
Discussion
Lung injury is a possible side effect of CDK4/6 inhibitors, and there is an increasing need to understand the management of this side effect.
Known Facts
• CDK4/6 inhibitors (palbociclib, ribociclib, and abemaciclib) have been approved for the treatment of metastatic breast cancer in patients with HR+ and HER2-negative (HER2-) subtypes [1-4].
• Ribociclib can cause adverse effects such as mielosupression (leukopenia, neutropenia) and cardiotoxity (QT interval prolongation requiring ECG monitoring) [9]
A new point of view: The FDA warning applies specifically to palbociclib (Ibrance), ribociclib (Kisqali), and abemaciclib (Verzenio), but warnings of the risk of pulmonary inflammation or pneumonia have been approved for addition to the prescribing information for the entire class of CDK4/6 inhibitors [11].
Case description: In March 2023, a 53-year-old postmenopausal female presented to us with metastatic breast cancer. Through self-examination, the patient felt this change in the area of the upper outer quadrant of the right breast. Mammography and ultrasound of the right breast with a core biopsy were performed.
The tumor biology:
• Histomorphologically, the tumor corresponds to a moderately differentiated ductal carcinoma of the breast.
• Immunophenotypically, the tumor corresponds to the Luminal A type (molecular subclassification):
- E-cadherin+
- ER+ (95%+++, score 8), PR+(60%++, score 6), HER2 - (0),
-Ki-67 = 10% (proliferation index is low).
As part of the evaluation, an MSCT examination of the chest, abdomen and pelvis was performed, which showed the absence of visceral metastases, but presence of bone metastases. In the right breast, there was a change measuring 44x30 mm, with a conglomeration of pathologically changing lymph nodes in the right axilla measuring 35x19 mm and several individual, enlarged lymph nodes. Changes in the bone structure can be observed diffusely on the bone structures of the shown parts of the spinal column, sternum, ribs, and iliac bones according to the type of secondary deposit of a mixed type.
The patient complained of difficulty walking and pain in the lower region of the spine, which propagated to the right leg, with tingling and weakness in the same. MRI of the spine showed diffuse metastatic bony lesions with pathological fractures of the Th XI, XII, and LI vertebral bodies without signs of process propagation into the spinal canal.
Initial values of tumor markers were: CEA 174.4 ug/L (the limit values <5 ug/L), CA 15-3>1002.0 (the limit values <23.5 U/ml).
The consilium suggests that the patient report to a spinal surgeon for consideration of stabilization of the thoracolumbar spine. The spine surgery team was involved. Percutaneous vertebroplasty Th XI, XII, and LI were performed by a spinal orthopedist. Subjectively, the patient felt better after spinal stabilization.
The patient started therapy with the CDK4/6 inhibitor Ribociclib-Kisqali (600 mg daily for 21 days and 1 week off) and Arimidex (1 mg per day every month).
Four weeks from the start of treatment, the patient was hospitalized at the Department of Oncology due to shortness of breath, dyspnea, and weakness. The differential diagnosis at that time included pulmonary embolism, chest infection, cardiac toxicity, and pulmonary edema. Clinically, the patient was not overloaded, and a chest examination was not indicative of pulmonary edema. Cardiac enzymes (including CK-MB and troponin), an electrocardiogram, and an echocardiogram were carried out, and all were unremarkable for cardiac cause. The clinical impression was in favor of pulmonary disease
The auscultatory findings on the lungs were bilaterally weakened breath sounds at the bases, with inspiratory crackles present. Blood gas analyzes were: pH 7.46↑, pCO2 4.70, pO2 8.70↓, cNa +128↓, cK +3.4, cCa ++ 1.03↓, glucose 6.5↑, Lac. cHct 34↓, cHCO3 24.9↑, SO2 c 94↓. The ionogram was within the acceptable limits of the reference values. Initial laboratory analyzes showed the following values in table below:
Table 1: Initial, control and the latest laboratory analyzes.
| Initial obtained values | Control values (6 weeks later) | The latest values | The limit values | |
|---|---|---|---|---|
| Leukocytes | 6.60 109/L | 10.38 109/L | 3.96 109/L | 3.70 – 10.00 109/L |
| Absolute neutrophils # | 4.40 109/L | 8.9 109/L | 2.88 109/L | 2.10 -6.50 109/L |
| Erythrocytes | 4.50 1012/L | 3 1012/L | 3.57 1012/L | 3.86 -5.08 1012/L |
| Hemoglobin | 116 g/L | 85 g/L | 106 g/L | 110 -157 g/L |
| Platelets | 248 109/L | 247 109/L | 225109/L | 135-450 109/L |
| Total proteins | 53↓g/L | 63↓ g/L | - | 64-83 g/L |
| Albumins | 32↓ g/L | 33↓ g/L | - | 35-52 g/L |
| Globulins | 27 g/L | 30 g/L | - | 21-31 g/L |
| Total bilirubin | 15.9 umol/L | 15.1 umol/L | 14.5 | 5.0-21.0 umol/L |
| direct bilirubin | 8.7↑ umol/L | 3.7 umol/L | 5.5 | 0.0-6.5 umol/L |
| AST | 174↑ U/L | 33 U/L | 19 | 0-40 U/L |
| ALT | 74↑ U/L, | 22 U/L | 17 | 0-40 U/L |
| GGT | 156↑ U/L | - | - | 7-50 U/L |
| Alkaline phosphatase | 231↑ U/L | 139 U/L | 120 | 34-104 U/L |
| Urea | 5.4 mmol/L | 5.6 mmol/L | 4.2 | 3.0-8.0 mmol/L |
| Creatinine | 85 umol/L | 82 umol/L | 52 | 49-106 umol/L |
| INR | 1.05 | 1.21 | - | 0.90-1.10 |
| aPTT | 37.3↑ sec | 33.3 sec | - | 25.0-35.0 sec |
| Fibrinogen | 4.72 g/L | 6.7↑ g/L | - | 2.0-5.0 g/L |
| D dimer | 3.45↑ ug/ml FEU | 2.52↑ | - | <0.50 ug/ml FEU |
| C reactive protein | 125↑ mg/L, | 149 ↑ | 4 | 0.00-5.00 mg/L |
| Procalcitonin | 0.100 ng/ml | 0.22 ng/ml | - | 0.500-2.000 ng/ml |
| PCR test for Sars- Covid -2 | negative | negative | negative | Negative |
| LDH | 623 U/L↑ | 639 U/L↑ | - | 220-450 U/L |
JADERS: Japanese Adverse Event Reporting System; LDH: Lactate Dehydrogenase; LMWH: Low Molecular Weight Heparin; MRI: Magnetic resonance; MSCT: Multislice computed tomography (scanner); OS: Overall Survival; PCR: Polymerase Chain Reaction; PFS: Progression-free survival; PPI: Proton Pump Inhibitors; RF: Rheumatoid Factor; W-Taxol: Weekly Taxol.
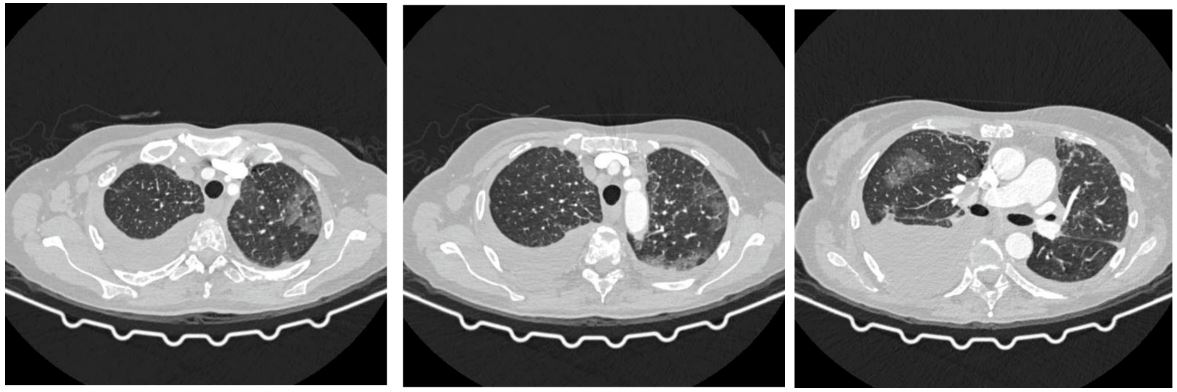
Figure 1: Chest scanner with GGO-type zones as part of ILD/pneumonitis.
On the X-ray of the heart and lungs, bilateral pleural effusions were present, more pronounced on the right. An urgent CT scan with contrast pulmonary angiography was performed, showing no signs of pulmonary thromboembolism (Figure 1).
A CT scan with contrast was performed, showing bilaterally present pleural effusions, more pronounced on the right. Diffuse in the visible part of the lung parenchyma, interlobular septa with GGO-type zones are highlighted on both sides in the upper lobes and the lower left lobe (Figure1). The clinical findings were worse than the radiographic. GGO- ground-glass opacity.
A pleural puncture was performed by a thoracic surgeon, during which approximately 1500 ml of serous content was obtained, which was sent for pathohistological analysis. The pathohistological findings of the pleural punctuate showed a structureless eosinophilic content, a mass of neutrophil granulocytes and erythrocytes, as well as rare mesothelial cells without noticeable malignant cells. Blood and sputum cultures remained sterile, and a comprehensive infectious disease workup was negative. Polymerase chain reactions for atypical pneumonia and respiratory viruses were all negative as well. Therefore, ribociclib was discontinued along with starting methylprednisolone (1.5 mg/kg/day), with noticeable clinical improvement within 1 week. The patient was treated with other symptomatic and supportive therapies, including oxygen therapy (O2 l/min), dual antibiotic therapy with probiotic, LMWH (Low Molecular Weight Heparin), PPI (Proton Pump Inhibitors), diuretic therapy, pain reliever, antiemetic therapy, and internal medicine therapy. Six weeks later, the patient displayed recovery, clinically. Therefore, the steroids were slowly tapered down. Ribociclib was permanently discontinued, Arimidex too. The patient continued treatment with systemic chemotherapy according to the W-Taxol (3+1) protocol. A control CT chest scan, showed that the previously described zones in the lung parenchyma according to the type of GGO are in progression (Figure 2). Other findings are stationary compared to the previous chest scanner.
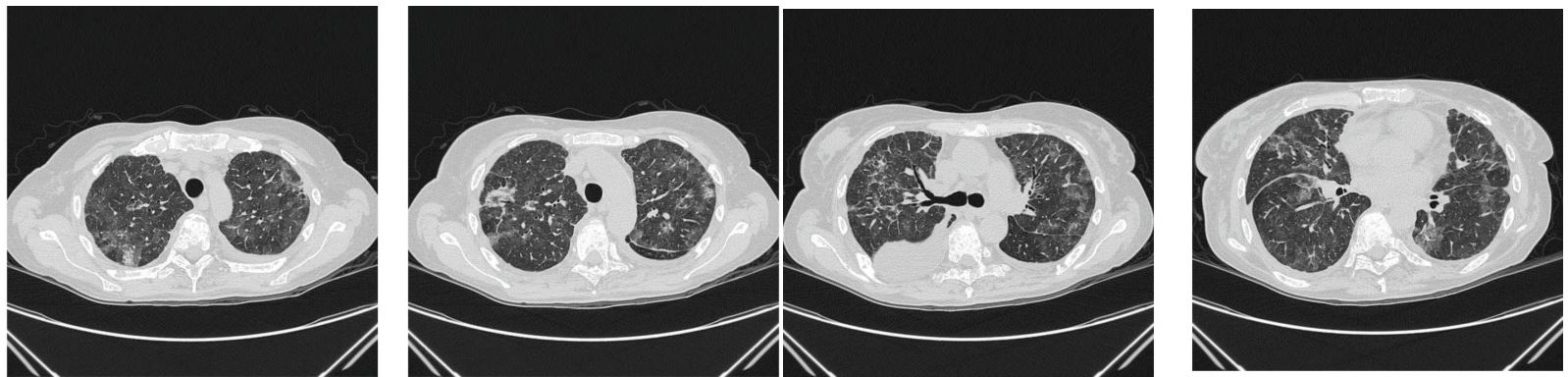
Figure 2: Chest scanner with GGO-type zones with progression as part of ILD/pneumonitis.
The patient was clinically better, but the control radiographic finding was in progression. Therefore, a pulmonologist was involved. Blood gas analyzes were: pH 7.47↑, pCO2 4.1↓, pO2 7.3↓, cNa +135↓, cK +3.2↓, cCa + 1.14↓, glucose 5.2, Lac 3.5, cHct 35, cHCO3 22.6, SO2 c 90%. Laboratory analyzes showed the control values in the Table 1. The ionogram was within the acceptable limits of the reference values. The urine test was normal. Immunological analyzes were within the limits of reference values: IgG 8.44 g/L, C3 1.59 g/L, C4 0.55 g/L, RF 11 IU/ml, AMA 1.1 IU/ml, ds DNA 10.2 IU/ml, cANCA 1.2 IU/ml, pANCA 0.9 IU/ml, ANA DETECT 0.3 (index). Tumor marker values were: CEA 474.1 (the limit values <5 ug/L) and CA 15-3 19899 (the limit values <23.5 U/ml). The pulmonologist prescribed corticosteroid therapy according to the following scheme: 40 mg of prednisone once daily for 3 weeks, then 30 mg of prednisone once daily for a month, then 20 mg of prednisone once daily for 3 months. Other recommended therapy by the pulmonologist included: PPI, LMWH, dual antibiotic therapy with a probiotic, formoterol/beclomethasone spray 100/6 mcg 3 times for two inhalations, fenoterol/ ipratropium bromide spray 3 times for two inhalations, oxygen therapy 1.5-2 l per minute, 18 hours during the night and day. After 3 months of therapy by a pulmonologist, the patient underwent a control scan of the chest and abdomen, which described a complete regression of zones according to the type of GGO as part of ILD/pneumonitis (Figure 3). The latest laboratory results are displayed in the third column of the Table 1. Tumor marker values then were: CEA 101.5 (the limit values <5 ug/L) and CA 15-3 3786 (the limit values <23.5 U/ml).
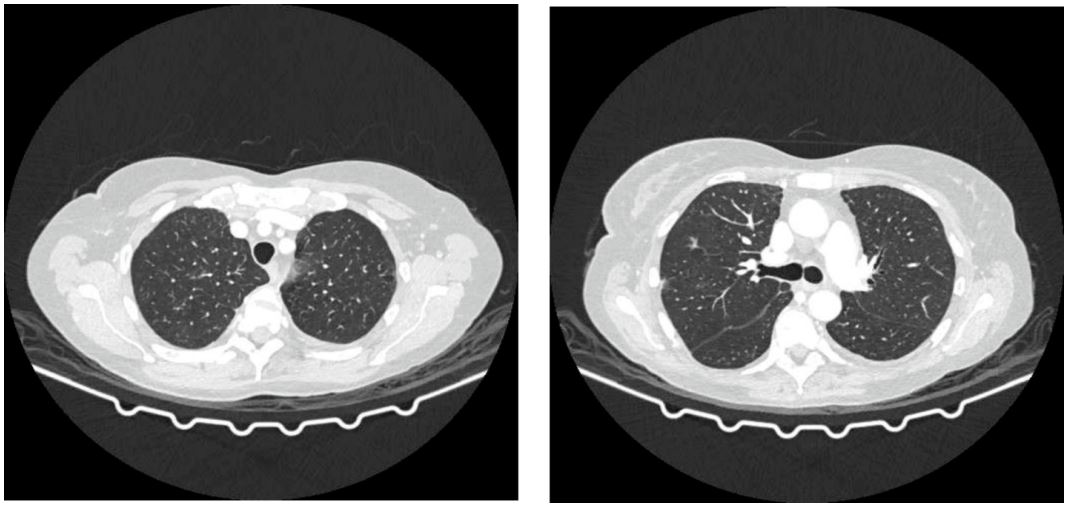
Figure 3: CT scan with complete regression of zones according to the type of GGO as part of ILD/pneumonitis.
The patient was presented to the consilium, which now makes the decision that the patient should continue with Arimidex and report in 3 months with the control findings of the chest and abdomen scanner. Other findings are stationary compared to the previous chest scanner.
Discussion
CDK4/6 inhibitors are increasingly being used, although rare adverse effects (AEs) including respiratory disorders have been reported. There have been a handful of severe and fatal cases of interstitial lung disease (ILD) and pneumonia caused by CDK4/6 inhibitors, which the FDA has warned about on drug labels [1]. Although cases of severe pulmonary inflammation, including fatalities, were observed in clinical trials with all CDK4/6 inhibitors, each agent demonstrated significant improvements in PFS [11]. From asymptomatic radiological changes to respiratory failure, anticancer medications have been associated with pulmonary toxicity [26]. Interstitial lung disease and/or pneumonitis may manifest as hypoxia, cough, dyspnea, or interstitial infiltrates on radiologic examinations in patients for whom all other causes have been ruled out [11]. In February 2015, the first CDK4/6 inhibitor, palbociclib, was approved for the treatment of breast cancer. [11]. According to the prescribing information for the drug, after the approval of palbociclib, the incidence of interstitial lung disease and non-infectious pneumonitis was observed [27].
In the MONARCH 3 trial, which compared the combination of abemaciclib and an aromatase inhibitor to an aromatase inhibitor alone in untreated postmenopausal women with HR-positive, HER2-negative locoregionally recurrent or metastatic breast cancer, one patient treated with the combination died from pneumonitis. In the MONARCH 2 trial, which compared the CDK4/6 inhibitor + fulvestrant to fulvestrant alone in women with HR-positive, HER2-negative advanced or metastatic breast cancer who have disease progression following endocrine therapy, two patients died from pneumonitis. The MONARCH 2 trial’s results supported the approval of abemaciclib [11]. According to the prescribing information, cases of interstitial lung disease/pneumonitis were also reported after approval [12]. Ribociclib in combination with an aromatase inhibitor was also approved in 2017 as initial endocrine-based therapy for postmenopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer [11]. There is less evidence showing the link between CDK-4/6 inhibitors and pulmonary toxicity. The articles on pablociclib- and abemaciclib-induced lung injury illustrate the potentially fatal drug-associated lung injury that may be associated with them. After four weeks of ribociclib use, our patient developed pneumonitis, which is uncommonly reported in the medical literature. The multi-slice chest scan revealed ILD/pneumonitis with GGO-type zones that were highlighted on both sides in the upper lobes and the lower left lobe, as well as bilateral pleural effusion (Figure 1). The clinical findings were worse than the radiographic (Figure 1). Therefore, ribociclib was discontinued along with starting methylprednisolone (1.5 mg/kg/day), with noticeable clinical improvement within 1 week. Six week later a control CT chest scan displayed progression of the previously described zones in the lung parenchyma according to the type of GGO (Figure 2). The patient was clinically better, but the control radiographic finding was in progression. Therefore, the pulmonologist prescribed corticosteroid therapy according to the following scheme: 40 mg of prednisone once daily for 3 weeks, then 30 mg of prednisone once daily for a month, then 20 mg of prednisone once daily for 3 months. After 3 months of therapy by a pulmonologist, the patient underwent a control scan of the chest and abdomen, which described a complete regression of zones according to the type of GGO as part of ILD/pneumonitis (Figure 3). In addition, previous real-world study based on the FAERS database showed that a median latency of 63 days (range 21-136) for CDK4/6 inhibitor-associated ILD [1]. This finding was in line with the results from an adverse event-time analysis of abemaciclib and palbociclib using data from Japanese Adverse Drug Event Report (JADER) database, suggesting that both abemaciclib and palbociclib were associated with the onset of ILD after 1-2 months from the start of treatment [29]. A retrospective study of drug-induced ILD demonstrated that, there was a certain similar trend in the timing of the occurrence of ILD induced by most anticancer drugs, most of which occurred within 3 months [30]. There are no known risk factors for the development of lung inflammation associated with CDK4/6 inhibitor use [11]. For patients with severe interstitial lung disease and/or pneumonitis who develope new or worsening pulmonary symptoms, the FDA recommends interrupting treatment and permanently discontinuing CDK4/6 inhibition and initiating corticosteroids [26]. It is essential for clinicians to remember that fatal interstitial pneumonitis can occur in ribociclib-treated patients (even after only four weeks into treatment), as early diagnosis can be crucial [9]. Besides early diagnosis of ILD/pneumonitis proper and continuos usage of corticosteroids is also crucial.
Acknowledgments: Not applicable.
Statement of ethics: The patient’s written consent was obtained for the writing and publication of her case, including the publication of images.
Competing interests: The authors declare that there is no conflict of interest.
Funding sources: No funding was received for this study.
Author contributions:
Danijela Niciforovic: Conceptualization; visualization; Writing – original draft; Writing – review & editing.
Dragica Pavlovic: Conceptualization; visualization; Writing – original draft; Writing – review & editing.
Dragana Papic: Conceptualization; visualization; Writing – original draft; Writing – review & editing.
Katarina Milojevic; visualization; Writing – original draft;
Marija Spasojevic: visualization; Writing – original draft;
Sanja Milojevic visualization; Writing – original draft;
Jasmina Nedovic: vsualization; Writing – original draft;
Marina Markovic: Conceptualization; supervision; Writing – review & editing
Abbreviations: AEs: Adverse Effects; ALT: Alanin transaminaza; Anti-dsDNA: Anti-double stranded DNA antibodies; AMA: Anti-Mitochondrial Antibodies; ANA: Antinuclear Antibodies; AST: Aspartate aminotransferase; CEA: Carcinoembryonic Antigen; CA 15-3: Carcinoma Antigen 15-3; CDK4/6 inhibitors: Cyclin-dependent kinase 4/6 inhibitors; C3: Complement Component 3; CK-MB: Creatine Kinase from cardiac muscle; FAERS: FDA Adverse Event Reporting System; FDA: Food and Drug Administration; GGT: Gamma glutamyl transferase; GGO: Ground-Glass Opacity; HR: Hormone Receptor positive; HER 2: Human Epidermal Growth Factor 2 Receptors; ILD/pneumonitis: Intersstitial Lung Disease/pneumonitis
References
- Zhang Y, Ma Z, Sun X, Feng X, An Z. Interstitial lung disease in patients treated with Cyclin-Dependent Kinase 4/6 inhibitors: A systematic review and meta-analysis of randomized controlled trials. Breast. 2022; 62: 162-169.
- KISQALI (ribociclib). Highlights of Prescribing Information, Novartis Pharmaceuticals Corporation, East Hanover, NJ, July 2018. https://www.pharma.us.novartis.com/sites/www.pharma.us.novartis.com/files/kisqali.pdf. Accessed October 9, 2018.
- IBRANCE (palbociclib). Highlights of Prescribing Information, Pfizer, New York, NY. 2018. Available at http://labeling.pfizer.com/ShowLabeling.aspx?id=2191. Accessed October 9, 2018.
- VERZENIO (abemaciclib). Highlights of Prescribing Information, Eli Lilly and Company, Indianapolis, IN. 2018. Available at https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208855s000lbl.pdf. Accessed October 9, 2018.
- Lanza O, Ferrera A, Reale S, Solfanelli G, Petrungaro M, Tini Melato G, Volpe M, et al. New Insights on the Toxicity on Heart and Vessels of Breast Cancer Therapies. Med Sci (Basel). 2022; 10: 27.
- Gelbert LM, Cai S, Lin X, Sanchez-Martinez C, Del Prado M, Lallena MJ, et al. Preclinical characterization of the CDK4/6 inhibitor LY2835219: in-vivo cell cycle-dependent/independent anti-tumor activities alone/in combination with gemcitabine. Invest New Drugs. 2014; 32: 825-37.
- Pavlovic D, Niciforovic D, Papic D, Milojevic K, Markovic M. CDK4/6 inhibitors: basics, pros, and major cons in breast cancer treatment with specific regard to cardiotoxicity - a narrative review. Ther Adv Med Oncol. 2023; 15: 17588359231205848.
- Samip R. Master.Cardiac complications of CDK4/6 inhibitors for breast cancer. Journal of Clinical Oncology. 2020; 38: 13038-13038.
- Algwaiz G, Badran AA, Elshenawy MA, Al-Tweigeri T. Ribociclib-Induced Pneumonitis: A Case Report. Breast Care (Basel). 2021; 16: 307-311.
- FDA warns about rare but severe lung inflammation with Ibrance, Kisqali, and Verzenio for breast cancer. FDA website. 2019. https://bit.ly/2lUvT1q. Accessed September 16, 2019.
- Astor L. FDA Warns of Lung Inflammation From CDK4/6 Inhibitor Use in Breast Cancers. Targeted Oncology. 2019. https://www.targetedonc.com/view/fda-warns-of-lung-inflammation-from-cdk46-inhibitor-use-in-breast-cancers
- Goetz MP, Hamilton EP, Campone M, Hurvitz SA, Cortes J, Johnston SR, et al. Acquired genomic alterations in circulating tumor DNA from patients receiving abemaciclib alone or in combination with endocrine therapy. J. Clin. Oncol. 2020; 38: 3519.
- Cristofanilli M, Turner NC, Bondarenko I, Ro J, Im SA, Masuda N, et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016; 17: 425-439.
- Dickler MN, Tolaney SM, Rugo HS, Cortés J, Diéras V, Patt D, et al. MONARCH 1, A Phase II Study of Abemaciclib, a CDK4 and CDK6 Inhibitor, as a Single Agent, in Patients with Refractory HR + /HER2 - Metastatic Breast Cancer. Clin Cancer Res. 2017; 23: 5218-5224.
- Johnston S, Martin M, Di Leo A, Im SA, Awada A, Forrester T, et al. MONARCH 3 final PFS: a randomized study of abemaciclib as initial therapy for advanced breast cancer. NPJ Breast Cancer. 2019; 5:5.
- Raschi E, Fusaroli M, Ardizzoni A, Poluzzi E, De Ponti F. Cyclin-dependent kinase 4/6 inhibitors and interstitial lung disease in the FDA adverse event reporting system: a pharmacovigilance assessment. Breast Cancer Res Treat. 2021; 186: 219-227.
- Malumbres M, Barbacid M. Cell cycle, CDKs and cancer: a changing paradigm. Nat Rev Cancer. 2009; 9: 153-66
- Braal CL, Jongbloed EM, Wilting SM, Mathijssen RHJ, Koolen SLW, Jager A. Inhibiting CDK4/6 in Breast Cancer with Palbociclib, Ribociclib, and Abemaciclib: Similarities and Differences. Drugs. 2021; 81(3): 317-331.
- Hortobagyi GN, Stemmer SM, Burris HA, Yap YS, Sonke GS, Paluch-Shimon S, et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann Oncol. 2018; 29: 1541-1547.
- Turner NC, Slamon DJ, Ro J, Bondarenko I, Im SA, Masuda N, et al. Overall Survival with Palbociclib and Fulvestrant in Advanced Breast Cancer. N Engl J Med. 2018; 379: 1926-1936. Bas O, Erul E, Guven DC, Aksoy S. Infectious complications of cyclindependent kinases 4 and 6 inhibitors in patients with hormone-receptor-positive metastatic breast cancer: a systematic review and meta-analysis. Support Care Cancer. 2022; 30: 9071-9078.
- Bas O, Erul E, Guven DC, Aksoy S. Infectious complications of cyclin-dependent kinases 4 and 6 inhibitors in patients with hormone-receptor-positive metastatic breast cancer: a systematic review and meta-analysis. Support Care Cancer. 2022; 30: 9071-9078.
- Coffman JA. Cell cycle development. Dev Cell. 2004; 6: 321-7.
- Hortobagyi GN, Stemmer SM, Burris HA, Yap YS, Sonke GS, Paluch-Shimon S, et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann Oncol. 2018; 29: 1541.
- Ahsan I MF, Jafri S. Palbociclib Related Pnemotoxicity: A Rare Side. 2017;195 A5546 EAJRCCM.
- Breast cancer drug Verzenio could have serious side effects on lungs Js, health ministry warns. The Japan Times. XUAA. 2019.
- Omarini C., Thanopoulou E., Johnston S. R. D. Pneumonitis and pulmonary fibrosis associated with breast cancer treatments. Breast Cancer Research and Treatment. 2014; 146: 245-258.
- Ibrance (palbociclib) [prescribing information]. Pfizer; April 2019. https://bit.ly/2kMcKPd.
- Verzenio (abemaciclib) [prescribing information]. Indianapolis, IN: Eli Lilly and Company. 2019. https://bit.ly/2JIpYU6.
- Nawa H, Niimura T, Yagi K, Goda M, Zamami Y, Ishizawa K. Evaluation of potential complication of interstitial lung disease with abemaciclib and palbociclib treatments. Cancer Rep (Hoboken). 2022; 5: 1402.
- Matsuno O. Drug-induced interstitial lung disease: mechanisms and best diagnostic approaches. Respir Res. 2012; 13: 39.
