
Open Access, Volume 9
Congenital absence of left atrial appendage: Case report and review of the literature
Anna Mengoni1*; Cinzia Zuchi1; Eugenio Trovarelli1; Stefano Sforna1; Giuliana Bardelli1; Federico Crusco2; Erberto Carluccio1; Giuseppe Ambrosio1
1Cardiology and Cardiovascular Pathophysiology, Santa Maria della Misericordia Hospital, Perugia, Italy.
2Complex Structure of Radiology, Santa Maria della Misericordia Hospital, Perugia, Italy.
Anna Mengoni
Cardiology and Cardiovascular Pathophysiology, Santa Maria della Misericordia Hospital, Perugia, Italy.
Email: mengoni@ospedale.perugia.it
Received : Oct 24, 2023,
Accepted : Nov 22, 2023
Published : Nov 30, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Congenital absence of left atrial appendage (LAA) is a rare condition, mostly diagnosed incidentally during imaging examination intended for other purpose. We reported a case of congenital LAA absence diagnosed in a 55-years-old man by trans-esophageal echocardiography (TEE) and confirmed by computed tomography (CT). We also conducted a systematic review of the twenty-eight cases reported in the literature.
Keywords: Absent left atrial appendage; Left atrial appendage agenesis; Atrial fibrillation trans-esophageal echocardiography; Anticoagulant therapy
Abbreviations: LAA: Left Atrial Appendage; LA: Left Atrium; TEE: Trans-Esophageal Echocardiography; CT: Computed Tomography; MESH: Medical Subject Heading; AF: Atrial Fibrillation; 3D: Three-Dimensional; ICD: Implantable Cardioverter Defibrillator.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Mengoni A (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Mengoni A, Zuchi C, Trovarelli E, Sforna S, Bardelli G. Congenital absence of left atrial appendage: Case report and review of the literature. Open J Clin Med Case Rep. 2023; 2161.
Introduction
Left atrial appendage (LAA) is a finger-like muscular extension of the left atrium (LA). It acts as blood reservoir, modulates LA pressure and elicits adaptive responses to stress. Several LAA shapes and variants have been described. We report a rare case of congenital absence of LAA diagnosed by trans-esophageal echocardiography (TEE) and confirmed by computed tomography (CT) in a 55-year-old patient. Additionally, we describe the characteristics of this congenital anomaly by reviewing relevant literature.
Materials and Methods
A systematic literature searches of PubMed and Google Scholar databases for case reports and related articles of absence/agenesis of left atrial appendage (LAA) published until July 2023 was conducted using “left atrium”, “appendage”, “congenital”, “atrial,” and “absent” in addition to the medical subject heading (MESH) terms “atrial appendage” as search terms. Twenty-three cases were identified among articles published. The characteristics of diagnostic modalities, demographic distribution and prognosis of this anomaly were studied.
Case Report
A 55-year-old male patient with history of hypertension, underwent a trans-esophageal echocardiogram for an undated episode of atrial fibrillation (AF). TEE showed normal LA volume without thrombi or echo contrast, but despite the three-dimensional acquisition, we were unable to identify LAA. Congenital absence of LAA was suspected and multi-detector cardiac CT confirmed the abnormality (Figure 1).
Results
In literature, 27 cases of congenital absence of LAA have been reported: the first case was described in 2012 by Collier et al. [1-24] among the 27 reported cases, 15 were men (53,6%) and 10 women (35,7%) (in 3 reports gender was not mentioned) with mean age of 63,3±16,7 years. Characteristics of the cases are reported in Table 1. 89% of the patients had a medical history of atrial fibrillation or atrial flutter.
In about 90% of cases, the abnormality was identified incidentally during imaging examinations performed before AF ablation, cardioversion procedures, LAA closure and implantable cardioverter defibrillator (ICD) implantation.
In 1 case the LAA absence was identified during a cardiac tomography performed for angor and dyspnea [19], in another case during TEE performed to evaluate intracardiac thrombi in a stroke patient [17] and in the last case during autopsy [11]. Only 5 patients had other congenital cardiac anomalies [4,11,18,21,22] but the embryological mechanism of this anomaly remains unknown. Only 3 patients had history of stroke and 2 compatibles with embolic process [7,17,24].
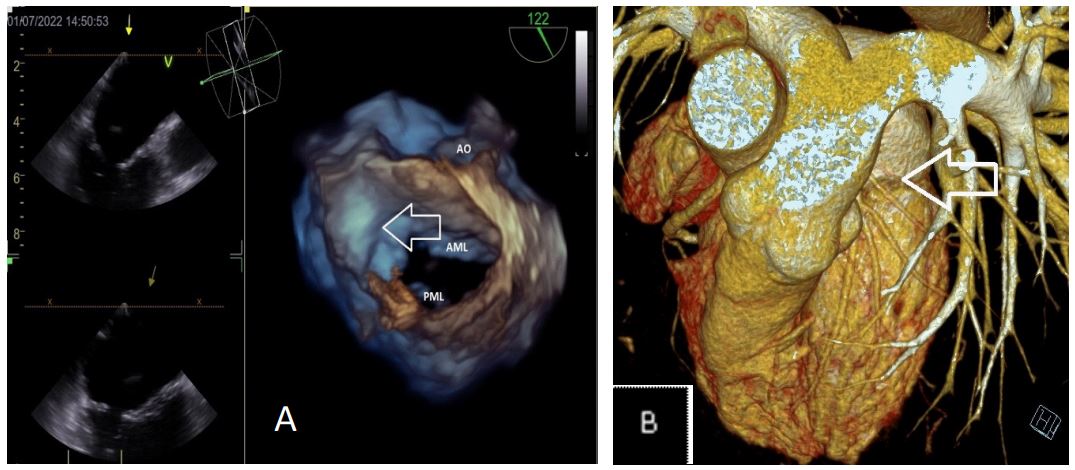
Figure 1: Congenital absence of LAA was suspected and multi-detector cardiac CT confirmed the abnormality.
A: 2D and 3D trans-esophageal echocardiogram: the arrow show absent of left atrial appendage.
B: Heart computer tomography. The arrow evidences no left atrial appendage.
Table 1: Characteristics of the cases are reported.
| Article/Date | Gender (m/f) | Age (Years) |
Past Medical History |
Associated Congental Pathology |
Diagnosed by |
Diagnostic Study/ Studies Performed |
Anticoagulant (NAO/TAO) |
|---|---|---|---|---|---|---|---|
|
Collier [12] (2012) |
F | 73 | AF | / |
Incidental finding during preprocedural TEE for AF cardioversion |
TEE | Unknown |
| Zhang [16] (2013) |
M | 60 | HTN, DM, CAD, AF | / |
Incidental finding during preprocedural TEE for AF ablation |
TEE + 3D Reconstruction; Cardiac CT angiography; Left atrial angiography |
Unknown |
|
De ponti [4] (2014) |
Unknown | 52 |
Idiopathic paroxysmal AF |
Persistent left SVC draining into the distal coronary sinus |
Incidental finding during preprocedural TEE for AF ablation |
TEE; Cardiac CT angiography |
Unknown |
| Rosso [9] (2015) | M | 62 | Paroxysmal AF | / |
Incidental finding during preprocedural TEE for AF ablation |
TEE; Cardiac CT angiography; Left atrial angiography |
Unknown |
|
di Gioia [6] (2015) |
M | 78 |
HTN, HLP, AF, History of intracranial bleeding with warfarin |
/ |
Incidental finding during pre-procedural evaluation of LAA closure |
TEE; Cardiac CT angiography |
No (Single antiplatelet therapy) |
| Ghori [8] (2015) | M | 50 | AF | / |
Incidental finding during pre-procedural TEE for AF cardioversion |
TEE; Cardiac CT angiography; Cardiac MRI |
Yes |
|
Saleh [15] (2015- 1) |
F | 54 | CAD-STEMI, CHF, AF |
/ |
Incidental finding during preprocedural TEE for AF ablation |
TEE; Cardiac CT angiography |
Yes |
|
Saleh [15] (2015- 2) |
M | 79 |
HTN, AF, non-ischemic cardiomiopathy |
/ |
Incidental finding during pre-procedural TEE for biventricular ICD insertion |
TEE | Unknown |
|
Katsumata [22] (2016) |
F | 76 | HTN, paroxysmal AF |
Persistent left SVC |
Incidental finding during pre-procedural CT for AF ablation |
TEE; Cardiac CT angiography; Left atrial angiography |
Unknown |
|
Song [24] (2016- 1) |
M | 68 | HTN, DM, CAD, AF | / |
Incidental finding during pre-procedural CT for AF ablation |
Cardiac CT angiography; Left atrial angiogram |
Yes (Warfarin for 12 months after ablation) |
|
Song [24] (2016- 2) |
F | 58 |
HTN, lacunar stroke, AF |
/ |
Incidental finding during pre-procedural CT for AF ablation |
Cardiac CT angiography; Left atrial angiogram |
Yes (Rivaroxaban) |
|
Kureshi [21] (2017) |
F | 62 | Obesity, HTN, AF |
Single left sided and 2 right-sided pulmunary veins |
Incidental finding during pre-procedural CT for AF ablation |
Cardiac CT agiography; TEE; 3D CT reconstruction of the LA in electroanatomic mapping system |
Unknown |
| Dar [10] (2017) | M | 67 | HTN, DM, AF | / |
Incidental finding in
pre- procedural CT for MAZE procedure for AF |
Cardiac CT angiography | Unknown |
| Enomoto [5] (2018) |
M | 70 | HTN, AF | / |
Incidental finding during pre-procedural TEE/CT for AF ablation |
TEE; Cardiac CT angiography; Left atrial angiography; 3D voltage mapping of LA |
Yes but stopped anti- coagulation 6 months after AF ablation as there was no AF recurrence and absent LAA |
| Lee [17] (2018) | M | 58 | Type 2 DM | / |
Work up for source of emboli |
TTE; TEE; Cardiac CT angiography |
Unknown |
| Nandar [23] (2018) |
F | 77 | HTN, HLP, AF | / |
Incidental finding during pre-procedural TEE/CT for AF ablation |
TEE; Cardiac CT angiography |
Yes (Warfarin) |
| Singam [1] (2018) |
F | 79 |
COPD, HTN, HLP, DM, CHF, persistent AF, intolerance for oral anticoagulation |
/ |
Incidental finding during pre-procedural evaluation of LAA closure |
TTE; TEE + 3D; Left
atrial angiography; Cardiac CT angiogrqaphy |
Yes |
| Pashun [19] (2019) |
M | 42 |
No past medical history, no AF |
/ |
Incidental finding during
CT angiography for angor and dyspnea |
Cardiac CT angiography | Unknown |
|
Pourafkari [3] (2020) |
M | 80 |
COPD, HTN, Atrial flutter |
/ |
Incidental finding during pre-ablation evaluation |
TEE; Cardiac CT angiography with 3D reconstruction |
Yes (Rivaroxaban) |
|
Vaideeswar [11] (2020) |
M | 0,25 |
History of respiratory distress |
Ostium secundum atrial septal defect; Ventricular septal defect, Trasposition of the great vessels; Mitral atresia; Single ventricle of right ventricular morphology with a double outlet |
Incidental finding during autopsy after death for adenoviral interstitial pneumonitis with superadded confluent bronchopneumonia |
TEE; Complete autopsy | No |
| Mayire [7] (2021) | F | 68 |
HTN, DM, History of ischemic stroke; paroxysmal AF (ablation refractoriness) |
/ |
Incidental finding during pre-procedural evaluation of LAA closure |
TEE + 3D Reconstruction; Cardiac CT angiography |
Yes (Warfarin) |
| Li [2] (2022) | M | 57 |
HTN, DM, paroxysmal AF (electric CV refractoriness) |
/ |
Incidental finding during pre-ablation evaluation |
TEE; Cardiac CT angiography |
No |
| Meeks [20] (2022) |
F | 70 | Paroxysmal AF | / |
Incidental finding during pre-ablation evaluation |
Cardiac CT agiography; TEE + contrast-enhanced imaging acquisition (i.v. Perflutren Lipid Microspheres - Definity) |
Yes |
| Vartak [14] (2023) |
F | 92 |
Atrial flutter, asthma, other comorbidities unknown |
/ |
Incidental finding during pre-procedural TEE for atrial flutter cardioversion |
TEE; Cardiac CT angiography |
Unknown |
|
Arguelles [18] (2023 -1) |
Unknown | 57 |
Paroxysmal AF, apical hypertrophic cardiomyopathy; ICD implantation after VT |
Anomalous right coronary artery originating from the left coronary cusp through a slit- like ostium with an interarterial course |
Incidental finding during preprocedural TEE for AF cardioversion |
TEE + 3D Reconstruction; Cardiac CT angiography |
Yes (Rivaroxaban) |
|
Arguelles [18] (2023 -2) |
Unknown | 71 |
Paroxysmal AF, HLP, severe meta- rheumatic mitral regurgitation awaiting for surgical MVR |
/ |
Incidental finding during pre-procedural evaluation of LAA closure |
TEE; surgical visualization | Unknown |
| Saghir [13] (2023) |
M | 58 |
Paroxysmal AF, CAD, DM, CHF, a n t i c o a g u l a t i o n intollerance |
/ |
Incidental finding during pre-procedural evaluation of LAA closure |
TEE; Cardiac CT angiography |
Unknown |
| Current (2022) | M | 55 | HTN, AF | / |
Incidental finding during pre-procedural TEE for AF cardioversion |
TEE + 3D Reconstruction; Cardiac CT angiography |
Yes |
(AF: Atrial Fibrillation; CAD: Coronary Artery Disease; CHF: Congestive Heart Failure; COPD: Chronic Obstructive Pulmonary Disease; CT: Computed Tomography; CV: Cardioversion; DM: Diabetes Mellitus; F: Female; HLP: Hyperlipidemia; HTN: Hypertension; ICD: Implantable Cardioverter-Defibrillator; LA: Left Atrium; LAA: Left Atrial Appendage; M: Male; MPR: Multi-Planar Reconstruction; MRI: Magnetic Resonance Imaging; MVR: Mitral Valve Replacement/Repair; STEMI: ST Elevation Miocardial Infarction; SVC: Superior Vena Cava; TEE: Transesophageal Echocardiography; TTE: Transtoracic Echocardiography).
Discussion
Left atrial appendage (LAA) is a finger-like muscular extension of the left atrium (LA) located close to the left ventricular free wall [25] and close to the left circumflex artery [26]. Several shapes and sizes of the LAA were described [27] and multiple imaging modalities can be used to define the its anatomy or to detect any in situ thrombosis, but the most widely used technique is TEE, especially with 3D reconstruction system [21]. As we showed, LAA agenesis is a rare condition but its real prevalence and incidence remains unknown because it is always an occasional finding. It seems more frequent in male patients and it can be associated with congenital heart defects that we should always look for. The role of this abnormality in thrombotic risk assessment has not been studied, but it is known that in patients with non-valvular AF, about 10% of intracardiac thrombi form at sites other than the LAA [28], so in these patients, the thrombotic risk remains no negligible. The congenital absence of LAA could be also considered similar to LAA percutaneous occlusion or surgical exclusion which are less effective than anticoagulants (IIb class of recommendation in ESC guideline Atrial Fibrillation 2020) [29]. Therefore, in our opinion, anticoagulant therapy should be considered, based on the traditional risk factor approach, using the clinical risk score for stroke CHA2DS2- VASc.
Conclusion
Congenital absence of LAA is an extremely rare condition, and despite reported cases are increasing, its embryological origin and its pathophysiological role in thromboembolic risk, is still not well defined.
Acknowledgments: None.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Singam NSv, Gopinathannair R, Stidam, J. M, Solankhi, N. K, Bessen, M, & Stoddard, M. F. A curious case of an absent left atrial appendage. Echocardiography (Mount Kisco, N.Y.). 2018; 35(11): 1882-1884. https://doi.org/10.1111/echo.1415.
- Li L, Qiuting F, Chunyuan Y, et al. Absence of Left Atrial Appendage in an Atrial Fibrillation Patient: Congenital or Acquired?. Authorea. 2022. https://doi.org/10.22541/au.164864861.19103708/v1.
- Pourafkari L, Sadeghpour A, Baghbani-Oskouei A, Savadi-Oskouei S, Pouraliakbar H, Fazelifar AF, et al. Absent left atrial appendage: case report and review of the literature. Cardiovascular Pathology. 2020; 45: 107178. https://doi.org/10.1016/j.carpath.2019.107178.
- De Ponti R, Lumia D, Zoli L, Marazzi R, Doni LA, Fugazzola C, et al. Agenesia of the left atrial appendage. Journal of Cardiovascular Medicine. 2016; 17: 116-117. https://doi.org/10.2459/JCM.0000000000000173.
- Enomoto Y, Hashimoto G, Sahara N, Hashimoto H, Niikura H, Nakamura K, et al. Congenital Absence of Left Atri-al Appendage Diagnosed by Multimodality Imaging. International Heart Journal. 2018; 59(2): 439-442. https://doi.org/10.1536/ihj.17-094.
- Di Gioia, G, Mega S, Visconti S, Campanale CM, Creta A, Ragni L, et al. Congenital Absence of Left Atrial Append-age in a Patient with Intracranial Hemorrhage. The American Journal of Case Reports. 2015; 16: 514-516. https://doi.org/10.12659/AJCR.894331.
- Mayire A, Jia LL, Yasen N, Zhou G, Du X. Congenital absence of left atrial appendage in a patient with ischemic stroke and atrial fibrillation. Clinical Case Reports. 2023; 11(2). https://doi.org/10.1002/ccr3.5847.
- Ghori MA, Alessandro S. Congenital absence of left atrial appendage: A case report and literature review. Journal of the Saudi Heart Association. 2015; 27(2): 132-134. https://doi.org/10.1016/j.jsha.2014.11.004.
- Rosso R, Vexler D, Viskin S, Aviram G. Congenital absence of left atrial appendage. Journal of Cardiovascular Elec-trophysiology. 2014; 25(7): 795. https://doi.org/10.1111/jce.12383.
- Dar T, Yarlagadda B, Swarup V, Lakkireddy D. Congenital Absence of Left Atrial Appendage. Journal of Atrial Fi-brillation. 2017; 10(3): 1730. https://doi.org/10.4022/jafib.1730.
- Vaideeswar P, Karande S. Congenital absence of the left atrial appendage. Journal of Postgraduate Medicine. 2020; 66(2): 108. https://doi.org/10.4103/jpgm.JPGM_671_19.
- Collier P, Cavalcante JL, Phelan D, Thavendiranathan P, Dahiya A, Grant A, et al. Congenital Absence of the Left Atrial Appendage. Circulation: Cardiovascular Imaging. 2012; 5(4): 549-550. https://doi.org/10.1161/CIRCIMAGING.112.975516.
- Saghir ZA, Ballard BD, Ianitelli MM, Mohan J. Congenital Absence of the Left Atrial Appendage and the Role of Anticoagulation. Journal of the American College of Cardiology. 2023; 81(8): 3636. https://doi.org/10.1016/S0735-1097(23)04080-9.
- Vartak N, Wutawunashe Cv, Toole J, Dwivedi A. Congenital absence of the left atrial appendage diagosed on mul-tidetector computed tomography. Journal of the American College of Cardiology. 2023; 81(8): 3356. https://doi.org/10.1016/S0735-1097(23)03800-7.
- Saleh M, Balakrishnan R, Castillo Kontak L, Benenstein R, Chinitz LA, Donnino R, et al. Congenital absence of the left atrial appendage visualized by 3D echocardiography in two adult patients. Echocardiography (Mount Kisco, N.Y.). 2015; 32(7): 1206-1210. https://doi.org/10.1111/echo.12882.
- Zhang ZJ, Dong JZ, Ma CS. Congenital absence of the left atrial appendage: A rare anatomical variation with clini-cal significance. Acta Cardiologica. 2013; 68(3): 325. 327. https://doi.org/10.1080/ac.68.3.2983429.
- Lee D, Kim D. Congenital Absence of the Left Atrial Appendage: An Unexpected and Incidental Anomaly in a Pa-tient with Multiple Cerebellar Infarctions. Chonnam Medical Journal. 2018; 54(2): 133. https://doi.org/10.4068/cmj.2018.54.2.133.
- Arguelles E, Mihalatos D, Leung A, Colangelo RG, Jayam V, Fujikura K. Congenital Absence of the Left Atrial Ap-pendage: Role of Multimodality Imaging. Case. 2023; 7(6): 220-225. https://doi.org/10.1016/j.case.2023.01.003.
- Pashun RA, Gannon MP, Tomassetti C, Rahmani N, Saba SG. Congenital absence of the left atrial appendage. Journal of Cardiovascular Computed Tomography. 2020; 14(6): 115-117. https://doi.org/10.1016/j.jcct.2019.07.009.
- Meeks W, Wilson R, Isbell D. Congenitally absent left atrial appendage: cardiac CTA and TEE correlation. BMJ Case Reports. 2022; 15(6): 250348. https://doi.org/10.1136/bcr-2022-250348.
- Kureshi F, Bateman TM, Wimmer AP. The “absent” left atrial appendage. HeartRhythm Case Reports, 2017; 3(10): 494-495. https://doi.org/10.1016/j.hrcr.2017.07.007.
- Katsumata Y, Kashimura S, Nishiyama T, Kimura T, Takatsuki S. The absence of a left atrial appendage in a pa-tient with paroxysmal atrial fibrillation with a persistent left superior vena cava. European Heart Journal – Cardiovas-cular Imaging, jew227. 2016. https://doi.org/10.1093/ehjci/jew227.
- Nandar PP, Kichloo A, Aung TT, Kravitz KD. Therapeutic Dilemma of Natural Watchman: Congenital Absence of the Left Atrial Appendage. Case Reports in Cardiology. 2018. 7573425. https://doi.org/10.1155/2018/7573425.
- Song IG, Kim SH, Oh YS, Rho TH. Underdevelopment of Left Atrial Appendage. Korean Circulation Journal. 2017; 47(1): 141. https://doi.org/10.4070/kcj.2016.0181.
- Beigel R, Wunderlich NC, Ho SY, Arsanjani R, Siegel RJ. The Left Atrial Appendage: Anatomy, Function, and Non-invasive Evaluation. JACC: Cardiovascular Imaging. 2014; 7(12): 1251-1265. https://doi.org/10.1016/j.jcmg.2014.08.009.
- Hensey M. A Review of the Anatomical and Histological Attributes of the Left Atrial Appendage with Descriptive Pathological Examination of Morphology and Histology. Journal of Atrial Fibrillation. 2018; 10(6). https://doi.org/10.4022/jafib.1650.
- Veinot JP, Harrity PJ, Gentile F, Khandheria BK, Bailey KR, et al. Anatomy of the Normal Left Atrial Appendage. Circulation. 1997; 96(9): 3112-3115. https://doi.org/10.1161/01.CIR.96.9.3112.
- Blackshear JL, Odell JA. Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. The Annals of Thoracic Surgery. 1996; 61(2): 755-759. https://doi.org/10.1016/0003-4975(95)00887-X.
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. ESC Scientific Document Group (2021). ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the Eu-ropean Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. European heart journal. 2020; 42(5): 373-498. https://doi.org/10.1093/eurheartj/ehaa612.
