
Open Access, Volume 9
Complete response to preoperative multimodal therapy of a persistent extraskeletal myxoid chondrosarcoma of the trunk: A case report
Michela Angelucci1*; Alessandra Panichelli1; Luca Improta1; Beniamino Brunetti2 ; Alessandro Strumia3; Carlo Greco4; Rossana Alloni1; Bruno Vincenzi5; Carla Rabitti6; Irene Aprile7; Sergio Valeri1
1Department of Surgery for Soft Tissue Sarcoma, Fondazione Policlinico Campus Bio-Medico, Rome, Italy.
2Plastic and Reconstructive Surgery, Fondazione Policlinico Campus Bio-Medico, Rome, Italy.
3Operative Unit of Anaesthesia and Intensive Care, Department of Medicine, Fondazione Policlinico Campus Bio-Medico, Rome, Italy.
4Division of Radiotherapy, Fondazione Policlinico Campus Bio-Medico, Rome, Italy.
5Department of Medical Oncology, Fondazione Policlinico Campus Bio-Medico, Rome, Italy.
6Department of Pathology, Fondazione Policlinico Campus Bio-Medico, Rome, Italy.
7IRCCS Fondazione Don Carlo Gnocchi-Onlus, Florence, Italy.
Michela Angelucci
Department of Surgery for Soft Tissue Sarcoma, Fondazione Policlinico Campus Bio-Medico Rome, Italy.
Tel: 003906225411331;
Email: michela.angelucci@unicampus.it
Received : Oct 20, 2023,
Accepted : Nov 17, 2023
Published : Nov 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Extraskeletal myxoid chondrosarcoma (EMC) is a rare malignant neoplasm affecting mesenchymal tissue. EMC patients need tailored treatments.
Methods: Clinical decision should be taken within a multidisciplinary tumor board, although, at present, limited specific literature evidence guides management. In this report, we present the case of a patient affected by persistent EMC of the thoracic wall treated with a multimodal combination of preoperative radiotherapy, chemotherapy, and hyperthermia.
Results: Pathological examination of the surgical specimen after the excision showed an unexpected complete response, suggesting a positive interaction of the preoperative treatment administered.
Conclusion: More extensive studies are needed to evaluate the potential additional effect of hyperthermia on preoperative therapies and better define its role among complementary treatments in high-risk STS.
Keywords: Case; Tumor; EMC; Sarcoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Angelucci M (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Angelucci M, Panichelli A, Improta L, Brunetti B, Strumia A, Greco C, Alloni R, et al. Complete response to preoperative multimodal therapy of a persistent extraskeletal myxoid chondrosarcoma of the trunk: A case report. Open J Clin Med Case Rep. 2023; 2159.
Introduction
Extraskeletal myxoid chondrosarcoma (EMC) is a rare malignant neoplasm affecting mesenchymal tissue. It comprises less than 3% of all adult soft tissue tumors [1]. Whereas EMC was initially classified as a low-grade sarcoma with indolent clinical course, long-term follow-up studies have emphasized its resilient nature with a significant potential for metastatic progression [2]. Typically, it affects patients between 50 and 60 years old, with a male to female ratio of 2:1 [3], and it usually arises from the soft tissues of the lower extremities (80%) and the superficial trunk (20%) [4]. Soft tissue sarcoma (STS) are rare tumors, with a variety of histological subtypes characterized by peculiar clinical features and specific therapeutic options [5]. To ensure the best chances of recovery, EMC patients need tailored treatments defined by a dedicated multidisciplinary tumor board (MTB) [6]. Nevertheless, specific literature on EMC is limited, and most evidence does not come from histology-specific studies. According to present guidelines, the only curative option for primary localized EMC is wide local resection [7]. Multiple options for preoperative treatment are available to improve local and systemic control. Radiation therapy (RT) is typically added to surgery as part of the standard treatment of high-grade lesions [8]. Historically, RT was delivered post-operatively in high grade lesions, although it is now commonly administered in the preoperative setting in order to induce tumor shrinkage and reduce long-term complications. Indeed, preoperative RT is strongly recommended in large lesions or when the mass is close to critical structures, such as nerves and vessels, and a wide surgical margin is therefore challenging to be obtained. On the other hand, post-operative RT can be delivered following a wide surgery in high-risk EMC [7,9]. Chemotherapy in high-risk EMC patients showed benefits both in disease-free survival (DFS) and overall survival (OS). Chemotherapy may be administered as preoperative treatment in naive patients with a double purpose: to reduce the tumor size before surgery and to reduce the risk for metastatic progression [7]. However, patients with significant comorbidities cannot be considered for neoadjuvant chemotherapy. In recent years, hyperthermia (HT) has been advocated as a potential novel treatment in combination with RT or chemotherapy, due to its radio and chemo-sensitizer activity. Moreover, HT directly damages tumor cells by its intrinsic cytotoxic effect, provided by induction of apoptosis and instability of the cell membrane, dysfunction of intracellular proteins, and impairment of DNA repair while increasing tissue oxygenation [10]. In this report, we present the case of a patient affected by persistent EMC of the thoracic wall, treated with a multimodal combination of preoperative RT, chemotherapy, and HT. Pathological examination of the specimen after a wide surgical excision showed a complete response.
Case Report
Informed consent has been obtained for the case report by the patient. This study was performed in line with the principles of the Declaration of Helsinki. A 50-year-old man came to our center in November 2020 with a history of persistent bulking mass of the left armpit. His co-morbidities included: class III obesity (BMI of 43,6), chronic obstructive pulmonary disease and obstructive sleep apnea syndrome, with a history of atrial fibrillation and arterial hypertension, currently under pharmacological control.
The patient reported self-palpatory findings of a mass in the axillary region, about 6 months earlier.
In a non-referral hospital, he underwent Magnetic Resonance Imaging (MRI). Then, a percutaneous biopsy was performed, highlighting a chondromyxoid fibroma at the pathological examination. The patient underwent debulking surgery. The postoperative course was uneventful. The pathological examination reported EMC. No post-operative treatments were provided.
When he came to our attention - 2 months after the first surgery - the patient showed a 7 cm nodule in the left armpit and a positive chest MRI, indicating an extra-costal solid mass of 10.93x7.89 cm.
The pathological review, performed by an expert pathologist at our referral center, confirmed the diagnosis of a G3 EMC according to WHO 2020 and FNCLCC (Fédération Nationale des Centres de Lutte Contra le Cancer) [11] both in the surgical specimen and in the first biopsy.
After the MTB discussion, taking into account the stratified perioperative and long-term risk [12], as well as the patient’s underlying pathologies, it was decided that a multimodal approach would be the proper course of action. Moreover, the persistence of the tumor in a challenging location – with a high risk of surgical site seeding during the previous procedure – worried the team of a high risk of further recurrence, even after wide re-excision, reinforcing the need for multimodal therapies. Preoperative chemoradiotherapy plus hyperthermia was administered with a weekly dose of 250 mg/mq of Gemcitabine plus a total dose of 56 Gy (fractionated in 200 cGy/day) plus 6 cycles of hyperthermia.
1 month after the preoperative treatment, the Computer Tomography scan (CT), showed a partial radiological response according to RECIST criteria with a mass measuring 9.00x6.8 cm [13].
MRI imaging of the mass before and after the preoperative treatments, and following the surgery, is shown in Figure 1.
In April 2021, 4 weeks after the end of preoperative treatment, a wide surgical excision was performed, which included partial resection of the left pectoralis major and minor muscles, of the left latissimus dorsi muscle and of the scapula, and a complete resection of serratus anterior muscle and infraspinatus muscle. The surgery also comprised en-bloc excision of the previous surgery scar. A concurrent reconstruction of the surgical defect was performed with a right fascia lata tensor fascio-cutaneous free flap. The scar of the first surgery, the preoperative drawing and the surgical field after the re-excision are shown in Figure 2.
The surgical specimen measured 30x20x16 cm. Pathological examination showed a nodule of 13x8 cm, at least 6,5 cm distant from all margins, consisting of areas of adipose tissue, hypo-cellulated areas, fibrotic areas, with spindle cells in a myxoid stroma and osseous tissue, in absence of viable tumor cells. Therefore, the mass showed a complete response to preoperative treatment. The histopathological aspect of the excised lesion is shown in Figure 3.
After MTB discussion, no further treatments were provided.
The early postoperative course was uneventful and the patient was discharged on postoperative day 19. One month after the surgery, the patient suffered from wound dehiscence (classification Clavien Dindo IIIa [14]) and was treated with 8 weeks negative pressure wound therapy, with a complete resolution. Over the following months, a progressive development of an edema on the left upper arm was treated with compressive bandages, with a complete resolution within 3 months from the beginning of the treatment.
During the postoperative phase, the patient underwent a 6-weeks long tailored physical rehabilitation program, reaching 50% recovery of the preoperative baseline functionality within 3 months from surgery. One year after surgery the patient returned to his normal life without any relevant restriction. 3-, 6- and 9-months follow-up MRI and CT scans did not highlightd any local relapse or systemic progression.
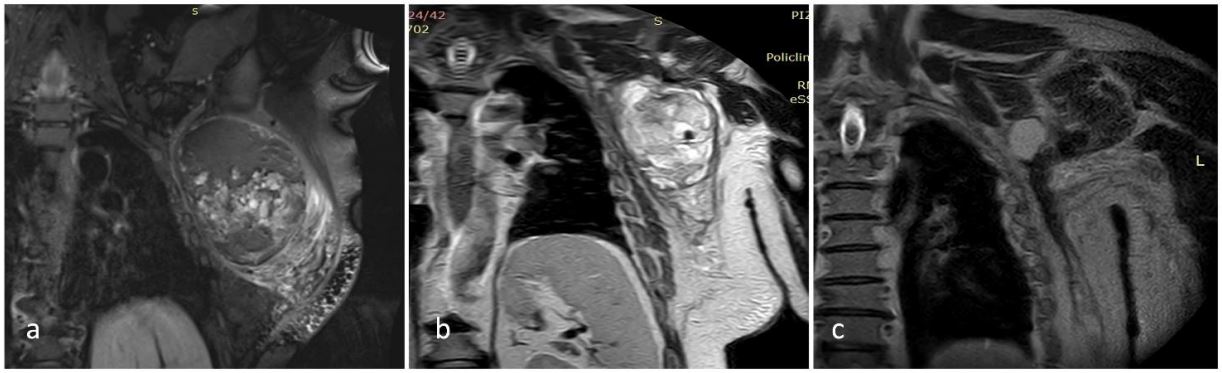
Figure 1: Pretreatment (a) Post-treatment (b), and Postoperative (c) MRI images: a) September 2021; b) November 2021;
c) March 2022.
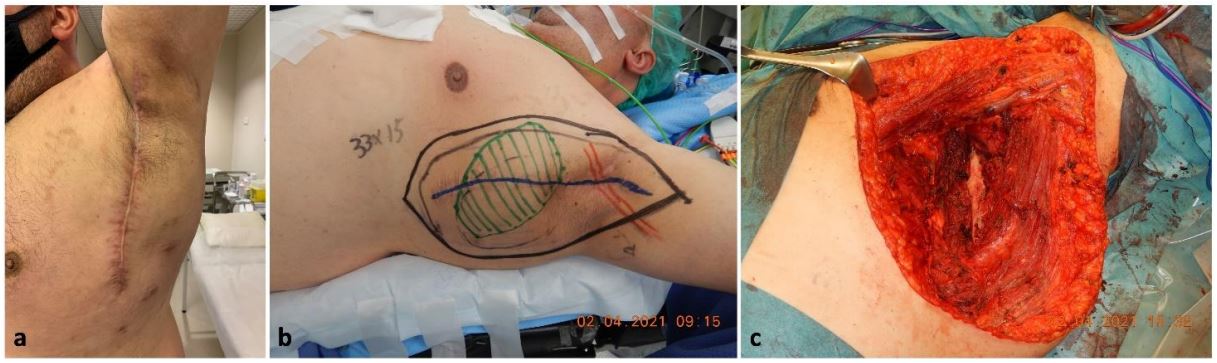
Figure 2: (a) Scar of the first surgery; (b) Preoperative drawing; (c) Surgical bed after tumor excision.
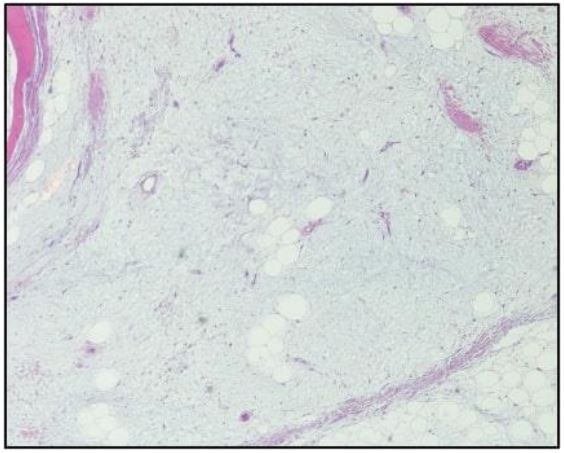
Figure 3: Histopathological aspect of the excised mass. A complete response to preoperative treatment was evidenced.
Discussion
Among STS histotypes, EMC is commonly characterized by an indolent course but, if not properly treated, the risk of uncontrolled local and systemic progression is consistent over time [3,5,6,10,11,15]. Patients who underwent unplanned excision have 34% risk of local recurrence versus 6% risk in patients who underwent planned wide excisions. An upfront appropriate surgery has been shown to increase local recurrence-free survival up to 89.7%, in patients with primary localized disease [16].
To our knowledge, this is the first reported case of a persistent EMC after inappropriate surgery in a non-referral center, which showed a complete pathological response to preoperative multimodal treatment.
From 20% to 60% of patients receive a diagnosis of STS only after an initial unplanned excision [17]. This exposes patients to a higher risk of residual disease, and, consequently, of local recurrence (LR) and, on the other hand, prevents access to preoperative complementary treatments, impairing long terms outcomes [15].
Radical surgery is mandatory after unintentional incomplete excision. It is still debated if the indication for margin enlargement is to be extended to patients who underwent a macroscopically-complete primary excision. Re-excision should always be considered for tumors located in critical sites, where a local recurrence may directly determine the prognosis [17].
Despite the fact that patients undergoing unplanned excisions in a non-referral center had a doubled risk of LR, no correlation with a higher risk of distant metastasis (DM) or with a reduction in the OS was demonstrated [17].
The MTB discussion is the cornerstone of the decision-making process for sarcoma patients. Multimodal therapy is critical for adequate local-regional and distant disease control in high-risk extremity and trunk STS patients [18].
In the reported case, after the MTB discussion, preoperative combination of chemotherapy, radiotherapy and hyperthermia were administered. Afterwards, the patient was re-nominated for radical surgery. This approach was chosen because re-excisions often require a larger surgery which is sometimes mutilating, sacrificing major motor function to warrant wide margins.
A multimodal approach to high-risk persistent STS of superficial trunk is consistent with the latest guidelines [7]. Moreover, EMC patients who received surgery alone showed significantly higher local recurrence rates than patients treated with a combination of surgery and neoadjuvant therapy [19].
The latest evidence highlights the need to tailor treatments to the clinical and biological qualities of the patients. In this specific case, it was pointed out how a further local recurrence would have been difficult to manage due to the tumor site and the patient’s comorbidities.
Most of preoperative chemotherapy regimens in STS consist of an association of ifosfamide and anthracycline (IA), to maximize both the cytotoxic and cytoreductive effect. Nevertheless, in resectable, localized STS, there is no consensus among experts on the routinary use of perioperative IA-based chemotherapy. Although widely adopted worldwide, perioperative IA-based chemotherapy is not a standard treatment [7,20]. Other drugs regimens and preoperative strategy could be proposed to tailor the best combination, which may include chemotherapy alone, concurrent chemo-radiation, or more commonly, chemotherapy and subsequent radiation [21].
Among chemotherapeutic agents, Gemcitabine has shown radio-sensitizing activity in a wide span of tumors. Preclinical data from cell lines and xenograft models also suggests that Gemcitabine could be an affective radiosensitizer also for STS, although literature evidence on a large cohort of STS patients is still lacking [18,22]. Considerable evidence suggests a potential role of Gemcitabine in STS patients. Tseng et al. highlighted its efficacy in a phase 1 trial in the preoperative setting, with better results on smallersize tumors. However, no correlation with tumor histology was found. Moreover, patients who completed preoperative gemcitabine and external-beam radiation therapy (EBRT) were more likely to undergo a complete tumor resection with microscopically negative margins [18]. That being said, it is important to mention that safety and efficacy of neoadjuvant gemcitabine plus RT in patients with STS is still unknown and larger trials are still lacking.
This report remarks the possible role of HT in STS patients, when literature data is still limited. Preclinical studies have confirmed its efficacy in inducing cytotoxic effects over several histologies, including STS [23]. Routine use of HT is currently limited to a small number of phase III clinical trials and poor availability of dedicated facilities [7,23,24]. Recent evidence highlighted how the use of regional HT plus neoadjuvant chemotherapy resulted in increased survival, as well as local progression-free survival among patients with localized high-risk soft tissue sarcoma [24]. Latest guidelines propose HT as a potential complementary treatment in STS [7] and concomitant preoperative HT and RT appear to be potentially useful in patients with locally advanced STS, who are not suitable for neoadjuvant systemic treatment due to poor performance status, chemo-resistant isotypes, or disease progression during chemotherapy [10].
The pleotropic effects on malignant cells and tumor stroma in contrasting tumor growth and progression have been recently summarized as hallmarks of hyperthermia. An updated analysis of a completed EORTC-ESHO intergroup randomized phase 3 trial for the most common types of high-risk STS demonstrates a significantly improved long-term overall survival in patients receiving preoperative radio – hyperthermia in combination with neo-adjuvant chemotherapy added to standard surgery and postoperative radiation [25]. Despite this evidence, a complete pathological response to preoperative multimodal therapy has never been reported in literature. The pathological response described in this report underlines the potential of multimodal therapy in enhancing the chances for local control in locally advanced or high-risk STS. Moreover, even with the limitation of a single case report, this study may suggest that a multimodal therapy consisting of concurrent chemoradiation plus hyperthermia could play a role even in patients unfit for surgery.
Conclusion
The combination of gemcitabine and RT could be effective in some isotypes. In the context of an unresectable disease (due to local extension or the patient’s comorbidities) an effective multimodal treatment could be the best chance for long–lasting palliation. The additional effect of hyperthermia should be evaluated in a prospective, multicentric study to accurately define its role among complementary treatments in high-risk STS.
References
- Masrouha K, Multani I, Bhatt O, Ghert M. Extraskeletal Myxoid Chondrosarcoma: Long-Term Survival in the Setting of Metastatic Disease. Case Rep Orthop. 2020; 2020: 2684746.
- Kawaguchi S, Wada T, Nagoya S, et al. Extraskeletal myxoid chondrosarcoma: a Multi-Institutional Study of 42 Cases in Japan. Cancer. 2003; 97: 1285-92.
- Drilon AD, Popat S, Bhuchar G, et al. Extraskeletal myxoid chondrosarcoma: a retrospective review from 2 referral centers emphasizing long-term outcomes with surgery and chemotherapy. Cancer. 2008; 113: 3364-71.
- Fidele NB, Tianfu W, Liu B, Sun Y, Yifang Z. Extraskeletal Myxoid Chondrosarcoma of the Parotid Gland. Ann Maxillofac Surg. 2019; 9: 439-43.
- Ray-Coquard I, Thiesse P, Ranchère-Vince D, et al. Conformity to clinical practice guidelines, multidisciplinary management and outcome of treatment for soft tissue sarcomas. Ann Oncol. 2004; 15: 307-15.
- Blay JY, Soibinet P, Penel N, et al. Improved survival using specialized multidisciplinary board in sarcoma patients. Ann Oncol. 2017; 28: 2852-9.
- Gronchi A, Miah AB, Dei Tos AP, et al. Soft tissue and visceral sarcomas: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up(☆). Ann Oncol. 2021; 32: 1348-65.
- von Mehren M, Randall RL, Benjamin RS, et al. Soft Tissue Sarcoma, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2018; 16: 536-63.
- Ogura K, Fujiwara T, Beppu Y, et al. Extraskeletal myxoid chondrosarcoma: a review of 23 patients treated at a single referral center with long-term follow-up. Arch Orthop Trauma Surg. 2012; 132: 1379-86.
- Spałek MJ, Kozak K, Czarnecka AM, Bartnik E, Borkowska A, Rutkowski P. Neoadjuvant Treatment Options in Soft Tissue Sarcomas. Cancers (Basel). 2020; 12.
- Sbaraglia M, Bellan E, Dei Tos AP. The 2020 WHO Classification of Soft Tissue Tumours: news and perspectives. Pathologica. 2021; 113: 70-84.
- Angelucci M, Strumia A, Gronchi A, et al. Traditional risk scores do not properly predict perioperative morbidity and mortality for retroperitoneal sarcoma resection. J Surg Oncol. 2022.
- Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009; 45: 228-47.
- Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009; 250: 187-96.
- Decanter G, Stoeckle E, Honore C, et al. Watch and Wait Approach for Re-excision After Unplanned Yet Macroscopically Complete Excision of Extremity and Superficial Truncal Soft Tissue Sarcoma is Safe and Does Not Affect Metastatic Risk or Amputation Rate. Ann Surg Oncol. 2019; 26: 3526-34.
- Potter BK, Adams SC, Pitcher JD, Jr., Temple HT. Local recurrence of disease after unplanned excisions of high-grade soft tissue sarcomas. Clin Orthop Relat Res. 2008; 466: 3093-100.
- Danieli M, Barretta F, Fiore M, et al. Unplanned Excision of Extremity and Trunk Wall Soft Tissue Sarcoma: To Re-resect or Not to Re-resect? Ann Surg Oncol. 2021; 28: 4706-17.
- Tseng WW, Zhou S, To CA, et al. Phase 1 adaptive dose-finding study of neoadjuvant gemcitabine combined with radiation therapy for patients with high-risk extremity and trunk soft tissue sarcoma. Cancer. 2015; 121: 3659-67.
- Bishop AJ, Bird JE, Conley AP, et al. Extraskeletal Myxoid Chondrosarcomas: Combined Modality Therapy With Both Radiation and Surgery Improves Local Control. Am J Clin Oncol. 2019; 42: 744-8.
- Casali PG, Abecassis N, Aro HT, et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018; 29: iv51-iv67.
- Nathenson MJ, Sausville E. Looking for answers: the current status of neoadjuvant treatment in localized soft tissue sarcomas. Cancer Chemother Pharmacol. 2016; 78: 895-919.
- Pauwels B, Korst AE, Lardon F, Vermorken JB. Combined modality therapy of gemcitabine and radiation. Oncologist. 2005; 10: 34-51.
- Jha S, Sharma PK, Malviya R. Hyperthermia: Role and Risk Factor for Cancer Treatment. Achievements in the Life Sciences. 2016; 10: 161-7.
- Issels RD, Lindner LH, Verweij J, et al. Effect of Neoadjuvant Chemotherapy Plus Regional Hyperthermia on Long-term Outcomes Among Patients With Localized High-Risk Soft Tissue Sarcoma: The EORTC 62961-ESHO 95 Randomized Clinical Trial. JAMA Oncol. 2018; 4: 483-92.
- Issels R, Lindner LH. Regional hyperthermia for high-risk soft tissue sarcoma treatment: present status and next questions. Curr Opin Oncol. 2016; 28: 447-52.
