
Open Access, Volume 9
Melanosis coli in a Nigerian female: A case report
Lukman O Abdulkareem1*; Oluwasesan A Abdul2; Rukayat A Abdulkareem3; Ojonogwa A Ameh1
1Department of Internal Medicine, University of Abuja Teaching Hospital, Abuja, Nigeria.
2Department of Histopathology, University of Abuja Teaching Hospital, Abuja, Nigeria.
3Department of Family Medicine, University of Abuja Teaching Hospital, Abuja, Nigeria.
Lukman O Abdulkareem
Department of Internal Medicine, University of Abuja Teaching Hospital, Abuja, Nigeria.
Email: lukkareem@yahoo.com
Received : Oct 17, 2023,
Accepted : Nov 15, 2023
Published : Nov 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Melanosis coli is a rare condition characterized by dark discoloration of the colonic mucosa. It is associated with long term use of anthraquinone-containing laxatives. It may be mistaken for other colonic diseases including ischaemic colitis. We present a middle-aged female with history of chronic constipation and longterm use of laxatives. Colonoscopy identified dark brown – black discoloration of the colonic mucosa which was suggestive of melanosis coli and confirmed by histology. The significance lies in the rarity of melanosis coli and the importance of avoiding a misdiagnosis. Dietary measures should be instituted in individuals with chronic constipation in order to avoid prolonged laxative use and possible development of melanosis coli.
Abbreviations: MC: Melanosis coli.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Abdulkareem LO (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Abdulkareem LO, Abdul OA, Abdulkareem RA, Ameh OA. Melanosis coli in a Nigerian female: A case report. Open J Clin Med Case Rep. 2023; 2157.
Introduction
Melanosis coli (MC) is a condition characterized by a brown to black discoloration of the colon [1]. It is associated with long term use of anthraquinone-containing laxatives in people with chronic constipation [1]. MC itself has no symptoms and it is frequently diagnosed incidentally during lower gastrointestinal endoscopy or during abdominal surgery. The importance of accurately diagnosing MC is the fact that it may pose a diagnostic dilemma and be confused for ischaemic colitis or other colonic diseases [2,3]. Though few cases have been reported in our country, most colonoscopy studies show the rarity of MC among Nigerians. [3,4]. This is the first case of MC seen at colonoscopy in our hospital in the past fifteen years of endoscopy practice.
Case Presentation
We present a 40 year old Nigerian female who presented with more than ten years’ history of chronic constipation. There was history of occasional anal pains and blood-stained stools over the past one year. She had associated recurrent abdominal discomfort which was usually relieved after passing hard stools. She had used various laxatives including herbs-based laxatives. She usually got some relief following the use of laxatives. Her physical examination findings were normal. Her basic blood investigations and abdomino-pelvic ultrasound scan were also normal. She was referred for colonoscopy on account of the chronic constipation and hematochezia with a working diagnosis of suspected Irritable Bowel Syndrome-Constipation (IBS-C) to rule out colorectal neoplasm. Colonoscopy showed brown-blackish discoloration of the mucosa of the caecum, ascending colon and part of the transverse colon (Figure 1). Mucosa of the descending colon, sigmoid and rectum appeared grossly normal. She also had internal hemorrhoids in the ano-rectal region on retroflexion of the colonoscope. Multiple biopsy specimen were taken from the different parts of the colon and sent for histology. Histology showed melanotic pigments within lamina propria macrophages and dense lymphoid follicles which confirmed the diagnosis of MC (Figure 2).
She was counseled on dietary measures with high fibre diet and liberal fluid intake as well as lifestyle modifications including exercise. She was subsequently followed up in the Gastroenterology out-patient clinic.
Discussion
Melanosis coli is a benign condition characterized by brown or black discoloration on the colonic mucosa [1]. It is caused by long-term use or abuse of anthraquinone-containing laxatives in individuals with chronic constipation. It has been reported in various age groups including children [5]. It is however, commoner among middle aged females [6], just like in our case who is middle-aged female. There have been few reported cases from our country [3]. Most colonoscopy reports have shown the rarity of this disorder in our country as they did not report finding MC among their patients [7-9]. However, a study in Lagos, southwest Nigeria reported prevalence of 0.3% among patients who underwent colonoscopy [4]. A similarly low prevalence of 1.2% was reported among colonoscopy in China [6].

Figure 1: Colonoscopy images showing hyperpigmentation of the colonic mucosa of the caecum, ascending and
transverse colon.
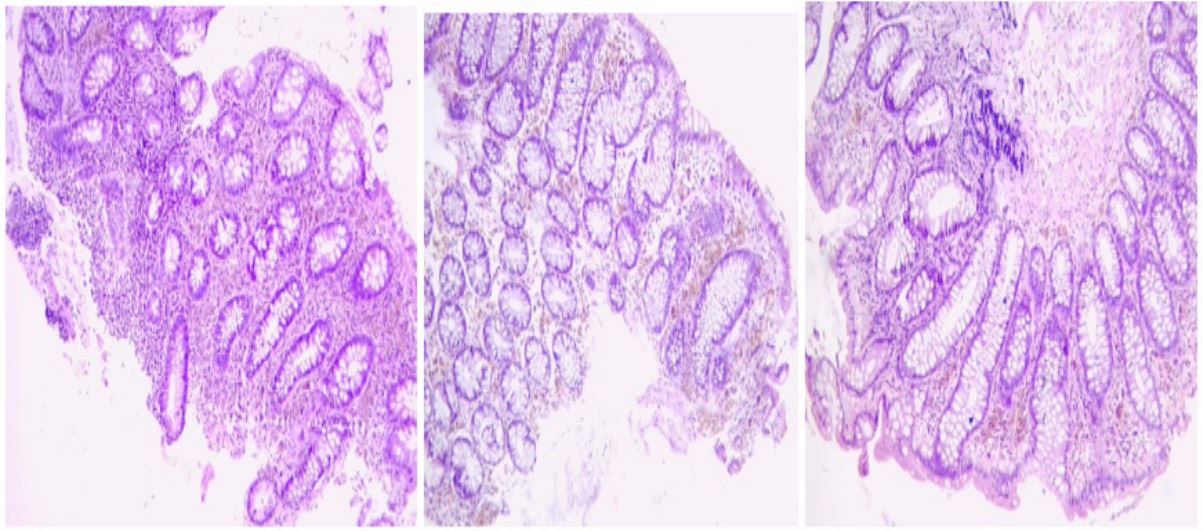
Figure 2: Histology microphotographs of our patient showing colonic type mucosa with melanotic pigments within lamina propria macrophages and dense lymphoid follicles.
Anthraquinone-based laxatives cause epithelial cell dysfunction often leading to impaired secretion, absorption and motility and causing cell death [1,10]. Macrophages phagocytose the dead cells with lipofuscin deposition in the lamina propria of the colon. Lipofusin rather than melanin (as the name “melanosis coli” may imply) causes the dark discoloration of the colonic mucosa [11]. Reports have shown that MC is commoner on the right side of the colon than the left with an antegrade progression from the caecum towards the rectum [1]. This is similar to the colonoscopy finding in our patient. However, there have been reports of pan-colonic involvement [11] .
MC is not known to cause any symptoms. It is usually an incidental finding during colonoscopy or surgery. Individuals at risk include those with chronic constipation, irritable bowel syndrome-constipation and elderly patients. About 95%of cases are associated with long term use of anthraquinone-based laxatives [11]. MC requires no specific treatment as it usually resolves after about six months of stopping anthraquinone-based laxatives. High-fibre diet, liberal fluid intake as well as exercise regimen should be instituted to relieve chronic constipation in patients with MC in order to avoid use of laxatives. Our patient was counselled on this as well.
Though MC is considered a benign condition, there are reports of increased adenoma detection rates in patients with MC [12]. This may be due to easier detection of polyps, which may lack pigment, proffered by the dark mucosa background of MC [12]. There is also a report of colon cancer in a patient with MC which was thought to be co-existence rather than a causal relationship [13]. Our patient had no colonic polyp but had internal hemorrhoids which was the likely cause of her rectal bleeds. Perhaps, the hemorrhoids were due to the chronic constipation she presented with and not a result of the MC. There has been reports of colectomy done at laparotomy due to misdiagnosis of MC as ischaemic colitis [2]. It is thus important to correctly identify MC and differentiate it from ischaemic colitis to avoid unwarranted surgery.
In conclusion, MC is a benign condition that is usually diagnosed incidentally during colonoscopy or surgery. It is usually caused by use of anthraquinone-based laxatives in patients with chronic constipation. The importance is in the avoidance of laxatives, mostly without prescription, in order to prevent development of MC. Proper identification by clinicians and confirmation by histology are important to avoid misdiagnosis.
References
- Yang N, Ruan M, Jin S. Melanosis coli: A comprehensive review. Gastroenterol Hepatol. 2020; 43(5): 266-272.
- Chaudhary BN, Sharma H, Nadeem M, Niayesh MH. Ischemic colitis or melanosis coli: a case report. World J Emerg Surg. 2007; 2(25): doi.org/10.1186/1749-7922-2-25.
- Ezike KN, Okwudire-Ejeh IA, Salu IK, Nnabuchi CV, Aghahowa ME, Ani FO, et al.. Biopsy-proven melanosis coli initially diagnosed as candidiasis on colonoscopy: A report of two cases from north central Nigeria. Cureus. 2023; 15(1): 34393. doi:10.7759/cureus.34393.
- Onyekwere CA, Odiagah JN, Ogunleye OO, Chibututu C, Lesi OA. Colonoscopy practice in Lagos, Nigeria: a report of an audit. Diagn Ther Endosc. 2013; 2013: 798651. doi: 10.1155/2013/798651.
- Jeong OS, Seung KL. Melanosis Coli Associated with Aloe Consumption in a Child. Korean J Pediatr Gastroenterol Nutr. 2010; 13: 81- 85.
- Liu ZH, Foo DCC, Law WL, Chan FSY, Fan JKM, Peng JS. Melanosis coli: Harmless pigmentation? A case-control retrospective study of 657 cases. PLoS ONE. 2017; 12(10): 0186668.
- Manko M, Bello AK, Mohammed MF, Jabir AM, Isah, IA, Daniyan M, et al. Colonoscopy in Zaria: Indications and Findings. Nig Jour of Clin Pract. 2022; 25(9): 1580-1583.
- Akere A, Oke TO, Otegbayo JA. Colonoscopy at a tertiary healthcare facility in Southwest Nigeria: Spectrum of indications and colonic abnormalities. Ann Afr Med. 2016; 15(3): 109-13.
- Musa Y, Abdulkadir YM, Manko M, Umar YS, Mohammed AN, Yusuf I, et al. A 10-year review of colonoscopy at Aminu Kano Teaching Hospital, Kano Nigeria. Niger J Clin Pract. 2021; 24(7): 1072-1076.
- Suharno H, Bayupurnama P, Ratnasari N. Melanosis coli. The Indonesian Journal of Gastroenterology, Hepatology, and Digestive Endoscopy. 2016; 17(2): 131-3.
- Moeller J, Solomon R, Kiffin C, Ditchek JJ, Davare DL. Melanosis Coli: A Case of Mistaken Identity-A Case Report. Perm J. 2019; 23: 18-063. doi: 10.7812/TPP/18-063.
- Blackett JW, Rosenberg R, Mahadev S, Green PHR, Lebwohl B. Adenoma detection is increased in the setting of melanosis coli. J Clin Gastroenterol. 2018; 52: 313-318.
- Zhao W, Chen J, Xing H, Yu J, Liu Q. Case report: Melanosis coli combined with colon cancer, causality or coincidence?. Front. Surg. 2022; 9: 973883. doi: 10.3389/fsurg.2022.973883.
