
Open Access, Volume 9
Brain Derived Neurotrophin Factor (BDNF) as a clinical marker of endometriosis
Manuel Garcia Manero1*; Nicholas Garcia Goyenechea2
1Hospital García Orcoyen, General hospital in Estella-Lizarra, Spain.
2Faculty of Medicine. University of Navarra, Spain.
Manuel Garcia Manero
Hospital García Orcoyen, General hospital in Estella-Lizarra, Spain.
Email: garciamanero4@gmail.com
Received : Sep 08, 2023,
Accepted : Nov 06, 2023
Published : Nov 10, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Endometriosis is a chronic, multifactorial disease of unknown etiology that affects approximately 10% of all women of childbearing age. It is characterized by dysmenorrhea and chronic pelvic pain, often associated with other symptoms (dyspareunia, dyschezia, rectal bleeding, dysuria, among others) and in 30-40% of cases it is associated with infertility.
The presence of pelvic pain is related to the process of neuroangiogenesis, with the presence of BDNF being a key piece in its development. Several recent studies have shown that BDNF levels are elevated in the serum of patients with endometriosis compared to patients without endometriosis. The objective of this study is to demonstrate if BDNF levels are higher in patients with endometriosis and if there is am correlation with the level of pain.
Material and methods: The study included 59 patients diagnosed with ovarian endometriosis in the Gynecology service of the Garcia Orcoyen Hospital during the period from November 2021 to August 2022. A blood sample was taken before surgery and their BDNF blood levels were determined. The levels of BDNF were analyzed compared to the control group in 10 patients undergoing laparoscopic tubal ligation to establish if the levels were higher in the endometriosis group and if there was a correlation with the intensity of pain.
Results: In this study, of the 59 patients recruited, 10 asymptomatic patients with endometriosis, 21 symptomatic patients who were not receiving hormonal treatment but only anti-inflammatory treatment, and 19 symptomatic patients receiving hormonal treatment were included. The rest of the patients (n=9) were excluded due to a diagnosis of endometriosis. As a control group, 10 patients undergoing tubal ligation as a contraceptive method were recruited.
The median BDNF value is 11.3 pg./ml among asymptomatic patients and 24.2 pg./ml among patients with symptoms. Statistical evidence is found (p < 0.05) which indicate that the median values are different depending on whether the patients show symptoms or not, being higher among patients who present symptoms.
BDNF has a median value of 35.0pg/ml among symptomatic patients treated with NSAIDs and 15.8pg/ml among symptomatic patients treated with ACOS (p<0.5).
Conclusion: Serum BDNF levels in women with endometriosis are significantly higher than in those patients without endometriosis. This level is directly correlated with the severity pelvic pain that the patient presents. Hormonal treatments produce a decrease in BDNF levels, which gives this marker the possibility of being used as a means of monitoring the response to treatment.
Keywords: BDNF; Endometriosis; Pelvic pain.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Emmanouil M (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Emmanouil E, Martinez-gonzalez B, Evangelidou M, Angelakis E. A case of hand-foot-and-mouth disease in a systemic lupus erythematosus patient presenting as late complication onychomadesis. Open J Clin Med Case Rep. 2023; 2151.
Introduction
Endometriosis is a chronic, multifactorial disease of unknown etiology that affects approximately 10% of all women of childbearing age. Its prevalence, although difficult to estimate precisely, may exceed that of diabetes mellitus or breast cancer. It is estimated that in Spain there are one million women affected by endometriosis.
Endometriosis is characterized by dysmenorrhea and chronic pelvic pain, often [1] associated with other symptoms (dyspareunia, dyschezia, rectal bleeding, dysuria, among others) and in 30-40% of cases it is associated with infertility. The difficulty of diagnosis lies in the variety of symptoms that often overlap, and which can be associated with other diseases, or have other etiologies (e.g. pelvic inflammatory disease, inflammatory bowel disease, diverticulosis, irritable bowel syndrome, cystitis). Interstitial, irritable bladder, somatization, depression, etc.) [2]. Added to this is the lack of patient consultation or referral from other professionals due to several factors, mainly: The lack of knowledge of the professionals or the patients themselves, which implies a false normalization of dysmenorrhea, and shame, fear or lack of of access to health services. This can make it take several years for endometriosis to be diagnosed, and explains the under-diagnosis of the disease. This delay is common and it is estimated that between 7 and 8 years can pass from the onset of symptoms to diagnosis [3,4].
- 47% of women with endometriosis have symptoms before turning 20, and progress brings with it serious consequences for the woman’s physical, sexual and emotional health [5,6]. Currently, efforts are focused on improving the diagnosis of this disease, to identify it in early stages and thus reduce unnecessary or inopportune surgeries, as well as its sequelae and complications. For this reason, more conservative management is increasingly
Advocated, prioritizing early medical treatment over surgical treatment. The existence of serum biomarkers could mean an advance in the diagnosis and a better evolution of the disease. In addition, these markers could be tools to monitor the response to various treatments.
Ovarian endometriosis is the most common form of the disease, representing more than 2/3 of the anatomical distribution. Ovarian involvement is mainly associated with pelvic pain and subfertility or infertility. Traditionally, the management of endometriosis cysts has been surgical, but multiple studies have shown the risks associated with this surgery: The involvement of the ovarian function due to trauma or destruction of healthy ovarian tissue, and the risk of recurrence due to incomplete excision of endometriotic tissue [7]. Furthermore, 25% of women who undergo surgery for ovarian endometriosis (cystectomy) experience recurrence of the disease, and it is known that reintervention produces much greater damage than the first surgery. Given this fact, if we can manage pelvic pain with medical treatment monitored by biomarkers, we would avoid the risks of surgery. The question we have always asked ourselves is why does endometriosis cause pelvic pain [8,9]. In the initial studies of angiogenesis it was shown that the formation of new blood vessels in the endometriotic process is linked to an increase in nociceptive fibers [10]. From this point of view, excision of endometriotic cysts should be associated with a significant improvement in pain.
However, pain in endometriosis is not always due to the local inflammatory effect and peripheral innervation but is also associated with a central mechanism [11-13]. Recent studies suggest the involvement of neurotrophins such as BDNF, NGF, nuerotrophin 3 and neurotransmitters 4 and 5 in endometriotic pathology [14-16].
After analyzing several types of neurotransmitters that could assess the degree of intensity of the painful symptoms of endometriosis, we decided to study serum levels of BDNF for 3 reasons:
1) Direct relationship with ovarian physiology. Follicular maturation.
2) Role in the development of neurons at the cerebral and peripheral level.
3) Serum marker of patients with ovarian endometriosis.
Aim
Primary objective: Determine if BDNF determination is a marker of endometriosis.
Secondary objective: analyze whether there is a correlation between the serum level of BDNF and the intensity of pain.
Figure
Materials and Methods
This study was carried out at the Garcia Orcoyen Hospital in Estella from November 2021 to August 2022. All participants gave informed consent and were willing to participate in this study, which had been approved by the hospital ethics committee. The study samples were obtained from patients who met the inclusion-exclusion criteria, recruiting 59 cases. Subjects with endometrial cysts detected endometrial cysts, pain, infertility and endometriosis through laparoscopic surgery were included in the endometriosis group. Laparoscopic tubal ligation was the criterion for selecting members of the control group Diagnosis and surgical procedures were performed by a reproductive endocrinology consultant obstetrician-gynecologist.
Furthermore, the degree of endometriosis was classified into 4 grades according to the American Reproductive Medicine (ASRM). The level of pain was determined using a Visual Analogue Scale (VAS), from scale 0 (absence of pain) to 10 (worst pain).
Measurement of serum BDNF: Blood samples were obtained before laparoscopic surgery Patients were asked to fast for at least eight hours, and then 5 ml of venous blood was drawn. The blood samples were subjected to serum preparation, and then the serum samples were immediately stored at -20 degrees Celsius until they were analyzed. Serum BDNF levels in patients and controls were measured by EnzymeLinked Immunosorbent Assay (ELISA) with Human BDNF Quantakine®. BDNF was measured according to the manufacturer’s instructions. All results were expressed in pg/ml [17]. The statistical analysis was carried out using the computer application: Rstudio (RStudio 2021.09.2+382 «Ghost Orchid» Release (fc9e217980ee9320126e33cdf334d4f4e105dc4f, 2022-01-04) for macOS
The statistical techniques and tests used have been:
(1) The quantitative variables have been described using the usual centrality and variability tools: mean and standard deviation, median and interquartile range. As well as the minimum and maximum values.
(2) In the case of categorical variables, the frequency and proportion presented by each of the categories within the variable have been shown.
(3) Normality tests have been carried out using a Kolmogorov-Smirnov test.
(4) In the case of variables that do not meet the conditions of normality, the non-parametric Mann- Whitney median contrast test has been applied when two groups are compared and the Kruskal- Wallis test has been applied when more than two groups are compared.
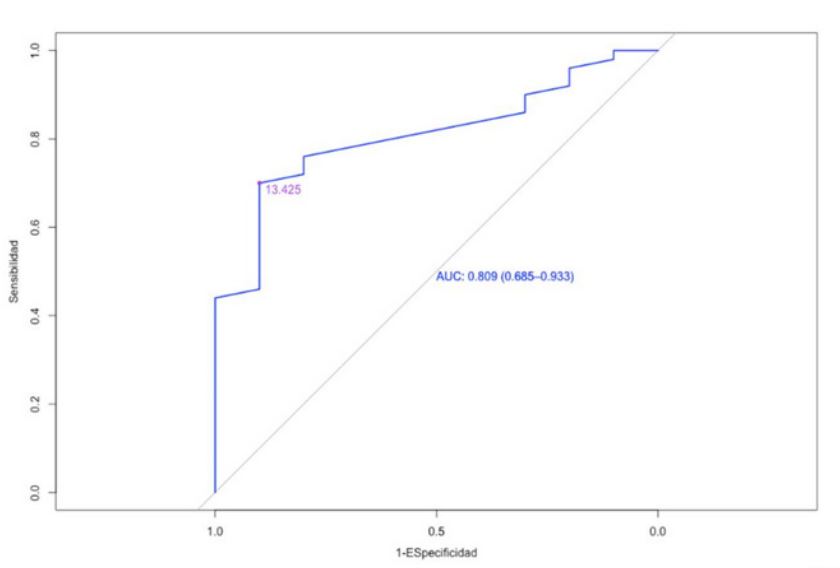
(5) To determine the cut-off point, a ROC graph has been used.
Results
In this study, of the 59 patients recruited, 10 asymptomatic patients with endometriosis, 21 symptomatic patients who were not receiving hormonal treatment but only anti-inflammatory treatment, and 19 symptomatic patients receiving hormonal treatment were included. The rest of the patients (n=9) were excluded due to a diagnosis of endometriosis. As a control group, 10 patients undergoing tubal ligation as a contraceptive method were recruited.
Descriptive analysis
35.0% of patients present symptoms and are treated with NSAIDs, while another 31.7% present symptoms and are treated with hormones. The control group makes up 16.7% of the patients included in the study. Similarly, we found another 16.7% of asymptomatic patients.
The average size of the cysts is 29.4 mm and that of BDNF is 20.5 pg/dl 16.7% of the patients are in stage I, 5.0% are in stage II, 43.3% are in stage III and the remaining 33.3% are patients who are in stage IV of endometriosis.
Regarding VAS, it can be seen that 65.0% of patients have a VAS of 0-3, 16.7% have a VAS of 4-7 and the remaining 18.3% have a VAS of 8-10. (13.4)
| Variable |
Total sample (n=60) |
|---|---|
| Symptoms | |
| Asymptomatic | 10 (16.67%) |
| Symptomatic NSAID treatment | 21 (35.00%) |
| Symptomatic Hormonal treatment | 19 (31.67%) |
| Control | 10 (16.67%) |
| size | |
| Mean (SD) | 29.4 (13.4) |
| Median (IQR) | 27.0 (20.2) |
| Range | 10.0 - 60.0 |
| BDNF | |
| Mean (SD) | 20.5 (11.4) |
| Median (IQR) | 16.4 (16.3) |
| Range | 5.7 - 47.3 |
| stadium | |
| I | 10 (16.7%) |
| II | 3 (5.00%) |
| III | 26 (43.33%) |
| IV | 20 (33.33%) |
| VAS | |
| 0-3 | 39 (65.00%) |
| 7-Apr | 10 (16.67%) |
| 10-Aug | 11 (18.33%) |
Inferential analysis
Next, the inferential analysis of the data described previously will be carried out with the aim of responding to the proposed objectives.
Firstly, an analysis of the normality of the BDNF variable has been carried out to determine whether parametric or non-parametric tests are applied throughout the analysis. The result of this test has shown that the variable does not meet the conditions of normality (p<0.05).
BDNF depending on whether patients have endometriosis or not the median BDNF value is 11.3 pg/dl among patients without endometriosis and 18.0 pg/dl among patients with endometriosis. Statistically significant differences are found (p<0.05) that indicate that the median BDNF values are different depending on whether the patients have endometriosis or not, being higher among patients with endometriosis.
| Variable | Total sample (n=60 |
|||
|---|---|---|---|---|
| Asymptomatic AC |
Tto symptoms aine |
Tto symptoms acos |
Control | |
| (N=10) | (N=21) | (N=19) | (N=10) | |
| size1 | ||||
| Mean (SD) | 30.7 (14.9) | 27.1 (14.3) | 30.5 (11.4) | 0 |
| Medium (IQR) | 27.0 (24.0) | 22.0 (11.0) | 30.0 (15.0) | |
| BDNF | ||||
| Mean (SD) | 11.6 (3.4) | 34.2 (6.7) | 14.8 (4.1) | 11.3 (3.8) |
| Medium (IQR) | 11.3 (3.6) | 35.0 (10.0) | 15.8 (3.8) | 11.3 (3.6) |
| stadium | ||||
| I | 1 (10.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) |
| II | 2 (20.00%) | 1 (4.76%) | 0 (0.00%) | 0 (0.00%) |
| III | 7 (70.00%) | 6 (28.57%) | 13 (68.42%) | 0 (0.00%) |
| IV | 0 (0.00%) | 14 (66.67%) | 6 (31.58%) | 0 (0.00%) |
| VAS | ||||
| 0-3 | 10 (100.00%) | 1 (4.76%) | 18 (94.74%) | 10 (100.00%) |
| 4-7 | 0 (0.00%) | 9 (42.86%) | 1 (5.26%) | 0 (0.00%) |
| 8-10 | 0 (0.00%) | 11 (52.38%) | 0 (0.00%) | 0 (0.00%) |
BDNF depending on whether patients have symptomatic or asymptomatic endometriosis. The median BDNF value is 11.3 pg/dl among asymptomatic patients and 24.2 pg/dl among patients with symptoms. There is statistical evidence (p<0.05) that indicates that the median values are different depending on whether the patients manifest symptoms or not, being higher among patients who present symptoms.
| No | VAS | P_value | |
|---|---|---|---|
| (N=10) | (N=50) | ||
| BDNF | |||
| Mean (SD) | 11.3 (3.8) | 22.3 (11.5) | |
| Median (IQR) | 11.3 (3.6) | 18.0 (20.3) | 0.002** |
BDNF depending on the treatment that symptomatic patients receive BDNF has a median value of 35.0 pg/dl among symptomatic patients treated with NSAIDs and 15.8 pg/dl among symptomatic patients treated with ACOS. In this way, important statistical differences (p<0.05) are found between the median values of the two groups, with the values being lower among patients treated with ACOS.
| Asymptomatic | Symptomatic | P_value | |
|---|---|---|---|
| (N=10) | (N=40) | ||
| BDNF | |||
| Mean (SD) | 11.6 pg/dl (3.4) | 25.0 pg/dl (11.3) | |
| Median (IQR) | 11.3 pg/dl (3.6) | 24.2 pg/dl (19.1) | <0.001** |
BDNF depending on the stages and level of pain The median BDNF value is 11.3 pg/dl among patients in stage 0, 13.0 pg/dl among patients in stage I, 8.9 pg/dl for patients in stage II, 16.0 pg/dl among patients who are in stage III and 28.1 pg/dl among patients in stage IV.
Commented [AH1]: In this case it cannot be carried out the inferential statistical analysis because in group I we only have one informed patient.
| Symptomatic | tto aine | Symptomatic | tto acos | P_value |
|---|---|---|---|---|
| (N=21) | (N=19) | |||
| BDNF | ||||
| Mean (SD) | 34.2 pg/dl (6.7) | 14.8 pg/dl (4.1) | ||
| Median (IQR) | 35.0 pg/dl (10.0) | 15.8 pg/dl (3.8) | <0.001** | |
BDNF has a median value of 13.0 pg/dl among patients with VAS 0-3, 34.8 pg/dl among patients with VAS 4-7 and 37.5 pg/dl among patients with VAS 8-10. It can be seen that there are statistically relevant differences (p<0.05) between the median values of the different VAS groups.
| 0 | Yo | II | III | IV | |
|---|---|---|---|---|---|
| (N=10) | (N=1) | (N=3) | (N=26) | (N=20) | |
| BDNF | |||||
| Mean (SD) | 11.3 pg/dl (3.8) | 13 pg/dl | 17.6 pg/dl (16.3) | 19.9 pg/dl (11.6) | 26.6 pg/dl (10.1) |
| Medium (IQR) | 11.3 pg/dl (3.6) | 13.0 pg/dl (0.0) | 8.9 pg/dl (14.5) | 16.0 pg/dl (10.3) | 28.1 pg/dl (17.0) |
BDNF breakpoint as a marker for endometriosis below is the ROC curve with the area under the curve for BDNF for women with endometriosis compared to women without endometriosis. The optimal cut-off point is 13,425 pg/dl, with the specificity value being 90.00% and the sensitivity value being 70.00%. The PPV value is 97.22% and the NPV value is 37.50%.
| 0-3 | 4-7 | 8-7 | P_value | |
|---|---|---|---|---|
| (N=39) | (N=10) | (N=11 | ||
| BDNF | ||||
| Mean (SD) | 13.2 pg/dl (4.5) | 33.0 pg/dl (7.4) | 34.9 (6.7) | |
| Medium (IQR) | 13 pg/dl (5.9) | 34.8 pg/dl (10.1) | 37.5 pg/dl (10.9) | <0.001* * |
Figure
Discussion
Disease marker as a determination that can be carried out in a simple way with adequate sensitivity and specificity in all stages of the disease and that allows monitoring the response to treatments, whether hormonal or surgical. Endometriosis is a chronic disease whose diagnosis currently takes about 8 to 10 years and to date there is no marker that allows this time to be shortened. In patients with endometriosis, multiple parameters have been analyzed as markers, as revealed by a recent study by Soto [33] where he analyzes glycoproteins, inflammatory cytokines, and antiangiogenics, reaching the conclusion that today there is no low-cost, non-invasive marker that detect progression and response to treatment.
In the Vessels studio [18]. The determination of BDNF was compared with that of other neurotropic drugs such as G¿NGF and NT4 where after a logistic regression analysis that included these markers and ca 125 and c-reactive protein, it was determined that BDNF is the best marker of endometriosis activity. Recently, Dwiningsih S [19] demonstrate how BNF has higher levels in women with endometriosis than those without the disease and finds an association with the degree of pain. However, it does not analyze the response to treatment, one of the key points to provide an optimal marker.
The results of this study reveal that the serum concentration of BDNF is higher in women with endometriosis than those who do not have this disease. Furthermore, these levels are directly correlated with the degree of pain intensity measured using the Visual Analogue Scale (VAS). It is also demonstrated how the level of said marker decreases in symptomatic cases treated with oral contraceptives. (with dienogest as gestagens)
One of the strengths of this work is including a control group without endometriosis, confirming that BDNF levels are higher in patients with endometriosis. Furthermore, symptomatic patients with endometriosis who did not receive oral suppressive treatment had higher levels than patients treated with hormonal treatment. These data on improvement in pelvic odor symptoms after treatment with dienogest agree with the Uludag data [20]. BDNF is a neurotransmitter belonging to the neurotrophin family that is expressed in the central and peripheral nervous system as well as in the female reproductive system. At the brain level it is related to cell survival, differentiation and neuronal plasticity. At the level of the female reproductive system it correlates with the maturation of the oocyte [21,22].
Several studies have shown elevated BDNF levels in serum of patients with endometriosis. Giavanni [23] describes higher levels in patients with endometriosis and how these levels decrease after surgical intervention. Rocha et al found elevated levels in patients with ovarian endometriosis related to pain intensity, while Vessel did not find this association due to the selected study population since BDNF levels are influenced by multiple factors.
Our results are in agreement with previous studies [24] where they state that BDNF levels show the endometriosis activity, that is, the relationship between active red lesions and inactive black lesions.
The relationship between BDNF and the presence of pain in endometriosis has been widely studied and it has been concluded that this factor is key in the transition from acute pain to chronic pain. The pathogenesis of pain in endometriosis is due to multiple pathophysiological mechanisms such as the presence of inflammation, neuro angiogenesis as described by Morotti [25-27]. Elevation of BDNF levels together with an increase in angiogenesis causes the presence of more intense pain symptoms [28,29]. Our group [30] In 2007, it already demonstrated greater vascularization in patients with symptomatic ovarian endometriomas. The presence of high levels of BDNF corroborates the phenomenon of neuroangiogenesis as one of the mechanism of pain origin [31]. This correlation between BDNF and inflammation in endometriosis opens the door to monitoring anti-inflammatory drugs as a pain treatment for the disease. If BDNF levels are not modified after the administration of a certain drug, we should opt for another line of treatment. This is a hypothesis that requires a prospective study to analyze the effect of the different NSAIDs and the response in time to them.
In ovarian endometriosis, the use of serum, clinical and ultrasound markers could facilitate the creation of a score that would avoid delaying the diagnosis of endometriosis. Our group has worked in isolation with the vascularization of the Ovarian endometrioma determined by Doppler ultrasound30, BDNF levels and VEGF levels, all of which found a correlation with the intensity of pain, which would allow the creation of a score that would facilitate the diagnosis of the disease [32].
References
- Fritz M, Speroff L. Clinical gynecologic endocrinology and infertility. 8th ed. Philadelphia: Lippincott Williams & Wilkins. 2011: 938.
- Garcia-Velasco JA, Somigliana E. Management of endometriomas in women requiring IVF: To touch or not to touch. Hum Play. 2009; 24: 496-501.
- Houston DE. Evidence for the risk of pelvic endometriosis by age, race and socioeconomic status. Epidemiol Rev. 1984; 6: 167-191.
- Ballard K, Lowton K, Wright J. What’s the delay? A qualitative study of women’s experiences of reaching a diagnosis of endometriosis. Fertile Steril. 2006; 86: 1296-301.
- Sangi-Haghpeykar H, Poindexter AN III. Epidemiology of endometriosis among parous women. Obstet Gynecol. 1995; 85: 983-992.
- Nnoaham KE, Hummelshoj L, Webster P, et al. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertile Steril. 2011; 96: 366-373.e8.
- Howard FM. Endometriosis and mechanisms of pelvic pain. J Minim Invasive Gynecol. 2009; 16: 540-50.
- Wang G, Tokushige N, Markham R, Fraser IS. Rich innervation of deep infiltrating endometriosis. Hum Play. 2009; 24: 827-34.
- Tokushige N, Russell P, Black K, Barrera H, Dubinovsky S, et al. Nerve fibers in ovarian endometriomas. Fertile Steril. 2010; 94: 1944-7.
- Davies A. Neurotrophins: Neurotrophins: Neurotrophic modulation of neurite growth. Curr Biol. 2000; 10: R198-R200
- Zhang X, Yao H, Huang X, Lu B, Xu H, et al. Nerve fibers in ovarian endometriotic lesions in women with ovarian endometriosis. Hum Play. 2010; 25: 392-397.
- McKinnon BD, Bertschi D, Bersinger NA, Mueller MD. Inflammation and nerve fiber interaction in endometriotic pain. Trends Endocrinol Metab. 2015; 26: 1-10.
- Kobayashi H, Yamada Y, Morioka S, Niiro E, Shigemitsu A, et al. Mechanism of pain generation for endometriosis-associated pelvic pain. Arch Gynecol Obstet. 2014; 289: 13-21.
- Dong F, Zhang Q, Kong W, Chen J, Ma J, et al. Regulation of endometrial cell proliferation by estrogen-induced BDNF signaling pathway. Gynecol Endocrinol. 2017; 33: 485-9.
- Begliuomini S, Casarosa E, Pluchino N, Lenzi E, Centofanti M, et al. Influence of endogenous and exogenous sex hormones on plasma brain-derived neurotrophic factor. Hum Play. 2007; 22: 995-1002,
- Browne AS, Yu J, Huang RP, Francisco AM, Sidell N, et al. Proteomic identification of neurotrophins in the eutopic endometrium of women with endometriosis. Fertile Steril. 2012; 98: 713-9.
- Russo N, Russo M, Daino D, Freschi L, Fiore L, et al. Evaluation of brain-derived neurotrophic factor in menstrual blood and its identification in human endometrium. Gynecol Endocrinol. 2012; 28: 492-5.
- Wessels JM, Kay VR, Leyland NA, Agarwal SK, Foster WG. Assessing brain-derived neurotrophic factor as a novel clinical marker of endometriosis. Fertile Steril. 2016; 105: 119-28.e1-5.
- Sri Ratna Dwiningsih, Christina Meilani, Samsul Hadi. Brain Derived Neurotrophic Factor as a Non-invasive Biomarker for Detection of Endometriosis J Reprod Infertil. 2022; 23: 207-212.
- Semih Z Uludag, Elif Demirtas, Yılmaz Sahin, Ercan M Aygen. Dienogest reduces endometrioma volume and endometriosisrelated pain symptoms. J Obstet Gynaecol. 2021; 41: 1246-1251.
- Dissen GA, Garcia-Rudaz C, Ojeda SR. Role of neurotrophic factors in early ovarian development. Semin Reprod Med. 2009; 27: 24-31.
- Hsun-Ming Chang, Hai-Cui Wu, Zhen-Gao Sun, Fang Lian, Peter CK Leung. Neurotrophins and glial cell line-derived neurotrophic factor in the ovary: Physiological and pathophysiological implications Hum Reprod Update. 2019; 25: 224-242.
- Giannini A, Bucci F, Luisi S, Cela V, Pluchino N, et al. Brain-derived neurotrophic factor in plasma of women with endometriosis. J of Endometriosis. 2010; 2: 144-150.
- Rocha AL, Vieira EL, Ferreira MC, Maia LM, Teixeira AL, et al. Plasma brain-derived neurotrophic factor in women with pelvic pain: a potential biomarker for endometriosis? Biomark Med. 2017; 11: 313-7.
- Morotti M, Vincent K, Becker CM. Mechanisms of pain in endometriosis. Eur J Obstet Gynecol Reprod Biol. 2017; 209: 8-13.
- Anaf V, Simon P, El Nakadi I, Fayt I, Simonart T, et al. Hyperalgesia, nerve infiltration and nerve growth factor expression in deep adenomyotic nodules, peritoneal and ovarian endometriosis. Hum Play. 2002; 17: 1895-900.
- Ding S, Zhu T, Tian Y, Xu P, Chen Z, Huang X, et al. Role of brain-derived neurotrophic factor in endometriosis pain. Reprod Sci. 2017; 25: 1045-57.
- Ding S, Zhu T, Tian Y, Xu P, Chen Z, et al. Role of Brain-Derived Neurotrophic Factor in Endometriosis Pain. Reprod Sci. 2018; 25: 1045-1057.
- Lentz SI, Knudson CM, Korsmeyer SJ, Snider WD. Neurotrophins support the development of diverse sensory axon morphologies. J Neurosci. 1999; 19: 1038-48
- Alcázar JL, García-Manero M Fertil Steril. Ovarian endometrioma vascularization in women with pelvic pain. 2007; 87: 1271-6.
- Obata K, Noguchi K. BDNF in sensory neurons and chronic pain. Neurosci Res. 2006; 55: 1-10.
- Garcia Manero M, Toledo G, Alcazar JL. J Womens Health (Larchmt) Relationship between microvascular density and expression of vascular endothelial growth factor in patients with ovarian endometriosis. 2008; 17: 777-82.
