
Open Access, Volume 9
Endometriosis presents with massive hemorrhagic ascites and catamenial hemopneumothorax
Aisel Alikhanova1*; Yinglin Gao1; Gary Thompson2; Sarah Duan2; Ricardo Chujutall1
1Loma Linda University Medical Center, Loma Linda, United States.
2Riverside University Health System Medical Center, Moreno Valley, United States.
Aisel Alikhanova
Loma Linda University Medical Center, Loma Linda, United States.
Email: aisel.alikhanova@gmail.com & AAlikhanova@llu.edu
Received : Sep 25, 2023,
Accepted : Oct 31, 2023
Published : Nov 02, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Endometriosis is an inflammatory disorder in women of reproductive age where endometrial cells grow outside the uterus. Although its pathogenesis is complex and not fully understood, it’s believed to stem from a combination of factors including congenital predisposition, environmental influences, epigenetic alterations, autoimmune responses, and allergic tendencies [1]. In rare cases, it can result in hemorrhagic ascites or even thoracic endometriosis syndrome (TES), where endometrial tissue is in the thorax, potentially causing catamenial pneumothorax and catamenial hemothorax. We report a case of a 32-year-old African American woman with both hemorrhagic ascites and hemopneumothorax.
Case Report: This case describes a 32-year-old African American woman with endometriosis, uterine leiomyoma, and major depressive disorder, who presented with progressive abdominal distention and exertional dyspnea. Clinical evaluation revealed tense ascites and a significant right hydropneumothorax. Diagnostic and therapeutic paracentesis and thoracentesis were performed, removing 2 Liters and 900ml of dark sanguineous fluid, respectively. Further assessment through right chest video-assisted thoracoscopic surgery (VATS) with biopsy identified numerous nodular lesions on the right lower lobe and hemidiaphragm, confirming stage 4 endometriosis.
Conclusion: Hemorrhagic ascites and TES are infrequent complications associated with endometriosis. It is crucial for clinicians to consider endometriosis in reproductive-age women, especially those who have not given birth, when encountering cases of hemorrhagic ascites and pleural effusions. Timely diagnosis and appropriate management are essential to prevent complications and ensure patient well-being.
Keywords: Disorder; Cells; Uterus; Syndrome.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Alikhanova A (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Alikhanova A, Gao Y, Thompson G, Duan S, Chujutall R. Endometriosis presents with massive hemorrhagic ascites and catamenial hemopneumothorax. Open J Clin Med Case Rep. 2023; 2149.
Background
Endometriosis occurs when endometrial tissue, typically found inside the uterus, spreads to areas outside the uterus, such as the peritoneum, ovaries, and rectovaginal septum. This condition impacts around 10-15% of women during their reproductive years and about 35-50% of women dealing with pelvic pain and/or infertility [2]. Common symptoms include menorrhagia, abdominal distention, and dyspnea. Rarely, it can lead to hemorrhagic ascites or even thoracic endometriosis syndrome (TES), A condition where endometriosis is found within the thorax and can lead to catamenial pneumothorax and catamenial hemothorax. We present a case of a 32- year-old African American female presenting with both hemorrhagic ascites and hemopneumothorax.
Case Report
Our patient is a 32-year-old African American female with endometriosis, uterine leiomyoma, major depressive disorder who presented to our hospital with progressive abdominal distention and new-onset dyspnea on exertion for two weeks prior to admission. She denies a history of tobacco, alcohol, or illicit drug use, and was not sexually active. The patient was previously being treated with oral contraceptives (OCPs) for her endometriosis but were discontinued approximately 1 year ago in anticipation for a planned pregnancy.
On admission, her vitals were within normal limits. Physical exam revealed an ill-appearing female who appeared in mild discomfort with significantly diminished lung sounds over the right lower chest and dullness to percussion. Her abdomen was non-tender but was moderately distended with a positive fluid wave and shifting dullness. Other systems were unremarkable. Initial lab values showed microcytic anemia with Hgb of 7.6, but normal renal and hepatic function testing. Chest, Abdomen and Pelvis CT without contrast showed a moderate right hydropneumothorax, moderate to large pleural effusion without lung mass, as well as large ascites and heterogeneous uterus with questionable prominent cervix, and normal ovaries.
The patient underwent a diagnostic and therapeutic paracentesis removing two liters of dark sanguineous fluid. She then underwent a diagnostic and therapeutic right thoracentesis, which removed 900 mL of dark sanguineous fluid. Fluid cytology did not show any malignant cells. Tumor markers, including CEA, AFP, CA-19-9, and HCG were negative, CA-125 slightly elevated. The Obstetrics and Gynecology team was consulted, who were suspicious of endometriosis as the cause of the hemorrhagic ascites. Pulmonology and Thoracic Surgery consulted, a right chest video-assisted thoracoscopic surgery (VATS) with biopsy was recommended to establish a definitive diagnosis for the pleural effusion given suspicious nodule found on imaging. Two additional liters of dark, chocolate-colored fluid were evacuated during the VATS, and small nodular lesions were seen on the right lower lobe and hemidiaphragm and its pathology revealed extensive thoracic endometriosis.
The patient was re-started on oral OCP therapy (OrthoCyclen) 0.25-35 mg-mcg per tablet during the hospitalization. At the time of discharge, the patient had a residual small right pleural effusion and small ascites but was asymptomatic with the resolution of her presenting symptoms. In her one-month followup, the patient reported compliance with OCPs and had no recurrence of symptomatic ascites or pleural effusions.
Table 1: Lab results.
| Value | Reference range | ||
|---|---|---|---|
| CBC | Wbc* | 6.5 X 10e9/L | 4.3 -11.3 X 10e9/L |
| Hgb* | 7.6 X10e9/L | 12.0 - 15.3g/dL | |
| Plt* | 335 X10e9/L | 147 - 409 X10e9/L | |
| CMP | Na* | 138 mmol/L | 136-145 mmol/L |
| K* | 3.1 mmol/L | 3.6-5.0 mmol/L | |
| Inflammatory marker | ESR* | 15 MM/hr | 0-20 MM/hr |
| CRP* | <0.290 MM/hr | 0.00-0.30 MM/hr | |
| ProBNP | ProBNP* | 45 pg/mL | 0-125 pg/mL |
| Peritoneal fluid | pH | 8.0 | n/a |
| Glucose | <1 | n/a | |
| LDH* | 1735 U/L | n/a | |
| Protein | 4.3 g/dL | n/a | |
| Wbc* | 1035/cumm | n/a | |
| Rbc* | 583,442/cumm | n/a | |
| Fungus | No Growth | No Growth | |
| Acid fast | No Growth | No Growth | |
| Culture | No Growth | No Growth | |
| Cytology |
An adequate number of
reactive mesothelial cells
are present, admixed with scattered lymphocytes, macrophages, and blood. No malignant cells identified. |
n/a | |
| Pleural fluid | pH | 7.0 | n/a |
| Glucose | 59 | n/a | |
| LDH* | 1140 U/L | ||
| Protein | 4.6 g/dL | n/a | |
| Wbc* | 2274/cumm | n/a | |
| Rbc* | 514157/cumm | n/a | |
| Fungus | No Growth | No Growth | |
| Acid fast | No Growth | No Growth | |
| Culture | No Growth | No Growth | |
| Cytology |
Reactive mesothelial cells
are present, admixed with
scattered lymphocytes, macrophages, and blood. No malignant cells are identified. |
n/a | |
| Iron Panel | Fe saturation | 4% | 20-55% |
| Fe* | 14mcg/dL | 50-170 mcg/dL | |
| TIBC* | 371mcg/dL | 250-450 mcg/dL | |
| Ferritin | 49.5 ng/mL | 8-252 ng/mL | |
| Tumor Marker | CA-125* | 114.9 U/mL | 1.5-35 U/mL |
| CEA* | 0.6ng/mL | 0.0-5.0ng/mL | |
| AFP* | 0.9ng/mL | 0.5-8.0 ng/mL | |
| Others | CA 19* | <2.0 | 2.0 - 37.0 U/mL |
| CG* | <1miu/mL |
NON-PREG FEMALE 1-3 miu/ mL |
|
| Albumin | 3.5g/dL | 3.4-5.0g/dL | |
| Total protein (serum) | 7.4 g/dL | 6.4 - 8.2 g/dL | |
| LDH* (serum) | 218 U/L | 84 - 246 U/L |
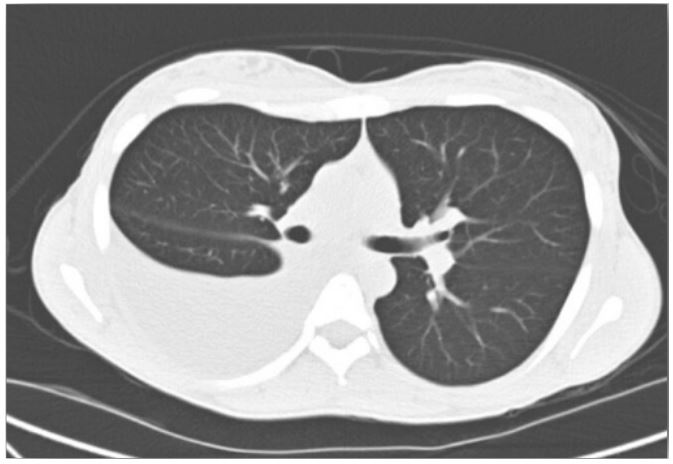
Figure 1: Computed tomography chest revealed a large
right-sided pleural effusion.
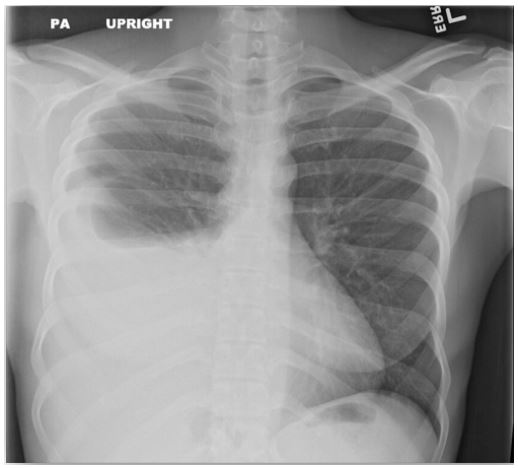
Figure 2: Chest X-ray revealed large right-sided pleural
effusion.
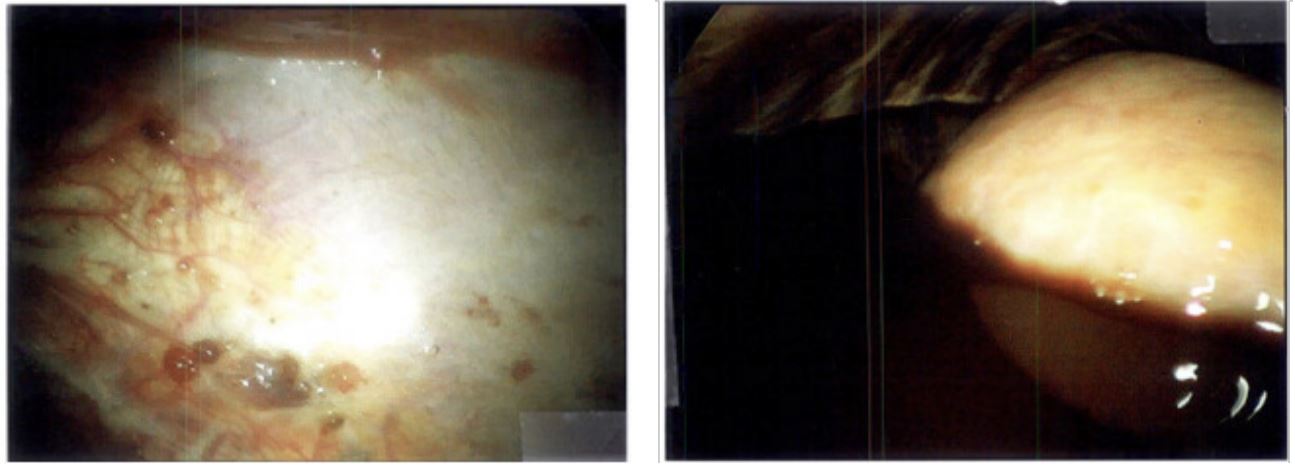
Figure 3: Right video assisted thoracoscopy revealed chocolate-colored fluid and small nodular lesions (later found to be
endometrial tissue on pathology).
Discussion
The first case of endometriosis in the literature can be dated back to 1954 which was described by Brew [3]. Endometriosis is an estrogen-dependent disease. It occurs when endometrial tissue, typically found inside the uterus, spreads to areas outside the uterus, such as the peritoneum, ovaries, and rectovaginal septum. Common symptoms include menorrhagia, abdominal distention, and dyspnea. The most common sites for pelvic endometriosis sites are the ovaries, uterine ligaments, pouch of Douglas, and fallopian tubes [4]. Occasionally, as observed in our patient, instances of extra-pelvic endometriosis implantation can manifest in the upper and lower respiratory systems, gastrointestinal tract, and even the pericardium [5].
Hemorrhagic ascites and thoracic endometriosis syndrome (TES) are rare complications of endometriosis. First involves the accumulation of blood in the abdominal cavity, leading to abdominal discomfort and bloating. Its pathophysiology remains unclear; however, it is hypothesized that hemorrhagic ascites could be due to peritoneal irritation from ruptured endometriotic implants, subdiaphragmatic obstruction of lymphatics, retrograde menstruation [6]. Endometrial tissue spreads to the peritoneum and other abdominal structures, resulting in inflammation and bleeding, which contributes to the development of hemorrhagic ascites. Additionally, factors like hepatocellular carcinoma, blunt trauma, and iatrogenicity have been implicated as risk factors for hemorrhagic ascites [7].
Based on current literature, approximately about 63% of women with extra-pelvic endometriosis were of African ancestry, and 82% were nulliparous; in addition, 38% of patients also had a pleural effusion at the time of diagnosis [8]. During the initial presentation, distinguishing between endometriosis with hemorrhagic ascites and other potential conditions like neoplastic growths or inflammatory causes such as pelvic Inflammatory disease, ovarian torsion, or peritoneal carcinomatosis can be challenging. The primary diagnostic method for endometriosis is ultrasound examination. This technique is especially useful for detecting ovarian endometrial cysts and reproductive organ anomalies that contribute to the backward flow of menstrual blood into the peritoneal cavity [9]. A conclusive diagnosis is achieved through a laparoscopic examination, followed by a comprehensive analysis of the pathological findings.
Regarding the extended management of recurrent substantial ascites resulting from endometriosis, the standard treatment encompasses Oral Contraceptive Pills (OCPs), which are combinations of estrogen and progestogen, function by decreasing FSH levels and stabilizing the endometrium. This process results in a reduction of pain. Additional options include GnRH analogs, danazol, and progestogens. Danazol acts by suppressing GnRH secretion, leading to reduced LH and FSH secretion from the pituitary gland. Treatment typically spans a lengthy period of 6-9 months and commences on the second day of the menstrual cycle. However, this medication is associated with numerous side effects, like weight gain, fluid retention etc [10].
The most recent medication sanctioned by the Food and Drug Administration (FDA) is Elagolix. This drug is intended for addressing the moderate to severe pain linked with endometriosis [11].
Surgical interventions can be classified into two categories: conservative and radical. Conservative approaches are recommended for adolescent patients and women of reproductive age who have fertility aspirations. Conversely, radical surgical measures are indicated for patients who do not intend to pursue pregnancy or for those who continue to experience chronic pain despite undergoing pharmacotherapy. In a recent study, bilateral ovariectomy cures the condition without recurrences, whereas after unilateral ovariectomy or cystectomy recurrence rate is more than 50%. In women desiring fertility, preferred conservative treatment with the destruction of endometriosis has a cure rate of 20% [12].
Conclusion
Endometriosis is a chronic condition that can significantly disrupt a patient’s life. While recurrent massive hemorrhagic ascites due to endometriosis is rare, it can be misleading and lead to incorrect treatment approaches, possibly even for malignancy. Most reported cases of hemorrhagic ascites have a good prognosis, but instances of hemorrhagic shock underscore the potentially life-threatening nature of endometriosis. Thus, it’s crucial to consider endometriosis as a vital differential diagnosis in reproductive-age women. Healthcare providers should strongly consider endometriosis as a potential cause in reproductive-age women, especially those who are nulliparous and present with hemorrhagic ascites and pleural effusions. While the outlook with OCP treatment is generally positive, delays in diagnosis could significantly affect a patient’s quality of life and overall well-being, potentially leading to serious complications.
Declarations
Acknowledgements: All the contributors meet the criteria for authorship and no financial support or other material support is needed to disclose and acknowledge.
Source of financial support: This publication’s authors confirm that they have no affiliations or involvement with any organization with a financial interest in the subject matter discussed.
Funding Statement: This publication’s authors confirm that they have no affiliations or involvement with any organization with a financial interest in the subject matter discussed.
References
- Smolarz B, Szyłło K, Romanowicz H. Endometriosis: Epidemiology, Classification, Pathogenesis, Treatment and Genetics (Review of Literature). International Journal of Molecular Sciences. 2021; 22(19): 10554. doi: 10.3390/ijms221910554.
- Smolarz B, Szyłło K, Romanowicz H. Endometriosis: Epidemiology, Classification, Pathogenesis, Treatment and Genetics (Review of Literature). International Journal of Molecular Sciences. 2021; 22(19); 10554. doi: 10.3390/ijms221910554.
- Brew A. Endometriosis, including endometriosis of the diaphragm and Meigs syndrome. Proceedings of the Royal Society of Medicine. 1954; 47: 461.
- Macer ML, Taylor HS. Endometriosis and infertility. Obstetrics and Gynecology Clinics of North America. 2012; 39: 535-549.
- Machairiotis N, Stylianaki A, Dryllis G, et al. Extrapelvic endometriosis: A rare entity or an under-diagnosed condition? Diagnostic Pathology. 2013; 8: 194. DOI: 10.1186/1746-1596-8-194. PMID: 24294950; PMCID: PMC3942279. Available from URL: https://pubmed.ncbi.nlm.nih.gov/24294950/.
- Morgan TL, Tomich EB, Heiner JD. Endometriosis presenting with hemorrhagic ascites, severe anemia, and shock. The American Journal of Emergency Medicine. 2013; 31(1): 272. e1-272.e3. Doi: 10.1016/j.ajem.2012.05.008.
- Urrunaga NH, Singal AG, Cuthbert JA, Rockey DC. Hemorrhagic ascites: Clinical presentation and outcomes in patients with cirrhosis. Journal of Hepatology. 2013; 58(6): 1113-1118. PMID: 23348236; PMCID: PMC4092117; NIHMSID: NIHMS591150.
- Nezhat, C, Lindheim, S. R, Backhus, L, et al. Thoracic Endometriosis Syndrome: A Review of Diagnosis and Management. JSLS: Journal of the Society of Laparoendoscopic Surgeons. 2019; 23(3); e2019.00029. DOI: 10.4293/JSLS.2019.00029. PMID: 31427853; PMCID: PMC6684338.
- Leyland N, Casper R, Laberge P, Singh SS. SOGC Endometriosis: Diagnosis and management. J. Obstet. Gynaecol. Can. 2010; 32: 1-32. doi: 10.1016/S1701-2163(16)34589-3.
- Smolarz B, Szyłło K, Romanowicz H. Endometriosis: Epidemiology, Classification, Pathogenesis, Treatment and Genetics (Review of Literature). International Journal of Molecular Sciences. 2021; 22(19): 10554. https://doi.org/10.3390/ijms221910554.
- Taylor HS, Giudice LC, Lessey BA, Abrao MS, Kotarski J, Archer DF, et al. Treatment of Endometriosis-Associated Pain with Elagolix, an Oral GnRH Antagonist. N. Engl. J. Med. 2017; 377: 28-40. doi: 10.1056/NEJMoa1700089.
