
Open Access, Volume 9
Be alert to aspiration in elderly bedridden patient
Chen Bingxu; Shi Jie; Qiu Yuangang; Ju Zhenyu; Chen Jie*
Department of Cardiology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Youdian Road No. 54, Hangzhou, Zhejiang Province, China.
Key Laboratory of Integrative Chinese and Western Medicine for the Diagnosis and Treatment of Circulatory Diseases of Zhejiang Province, Hangzhou, Zhejiang Province, Chin.
Chen Jie
Department of Cardiology, The First Affiliated Hospital of Zhejiang Chinese Medical University (ZhejiangProvincial Hospital of Chinese Medicine), Youdian Road No. 54, Hangzhou, Zhejiang Province, China;
Key Laboratory of Integrative Chinese and Western Medicine for the Diagnosis and Treatment of Circulatory Diseases of Zhejiang Province, Hangzhou, Zhejiang Province, China.
Tel: +86-13858028886;
Email: ktrina_cj@163.com
Received : Sep 20, 2023,
Accepted : Oct 30, 2023
Published : Nov 02, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Aspiration is one common complication during medical service practice, and could also incur severe outcome in elderly patient. We had three patients experienced this kind of accidence unfortunately last month, and only one survived at last. Hence, we advised physicians should be more alert to this complication, especially for elderly patients with some illness, and perform the deglutition training program regularly in case.
Keywords: Aspiration; Elderly patients; Deglutition training.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Jie C (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Bingxu C, Jie S, Yuangang Q, Zhenyu J, Jie C. Be alert to aspiration in elderly bedridden patient. Open J Clin Med Case Rep. 2023; 2147.
Introduction
It is usually said that aspiration is a kind of complications caused by gravity or indwelling a gastric tube in the esophagus after anesthesia, however, it is also one common fatal complication in elderly patients, especially for those bedridden. Here we provided 3 cases which occurred recently in our hospital. Unfortunately two of them passed out soon after aspiration.
Case Presentation
Our first patient is 95 year old patient who was admitted in our cardiology department for chronic heart failure rehabilitation more than 6 months, Besides, he had cerebral ischemic stroke, coronary artery disease hypertension in the past medical history, he also had partial gastrectomy surgery 30 years ago. His medicine plan followed the strict guideline including anti-coagulant, statin, diuretic and so further. He took food by the gastric tube for a long time, and performed the passive training and balance training everyday, and was stable during the past 5 months. One day, his care worker said he was choked by the nutrient solution, our nurse came to his bed immediately and sucked out coffee-like content by the suction catheter. The next few hour his temperature rose significantly,his sputum test showed the Klebsiella pneumoniae, we did the physical cooling for him and gave the antibiotics by his blood test and drug sensitivity test. We decided to performed the CT days later , however during his removal to the examination bed in the CT room, he was choked by his oral secretion again. He temperature rose sharply and we tried the everything except the Invasive procedures such as tracheal intubation for he had done the NO CODE consent. Unfortunately, he passed out for the shock by the intensive infection a few days later.
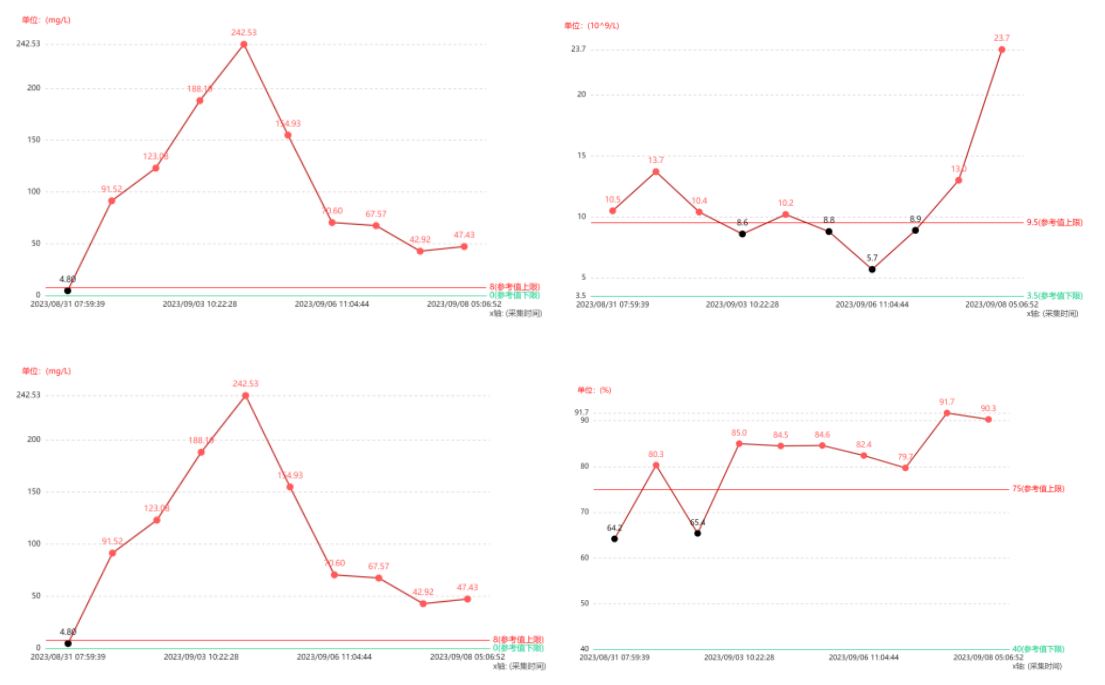
Figure 1: The suction content by our nursing worker. His WBC, N%, CRP and PCT trend
figure as follows.
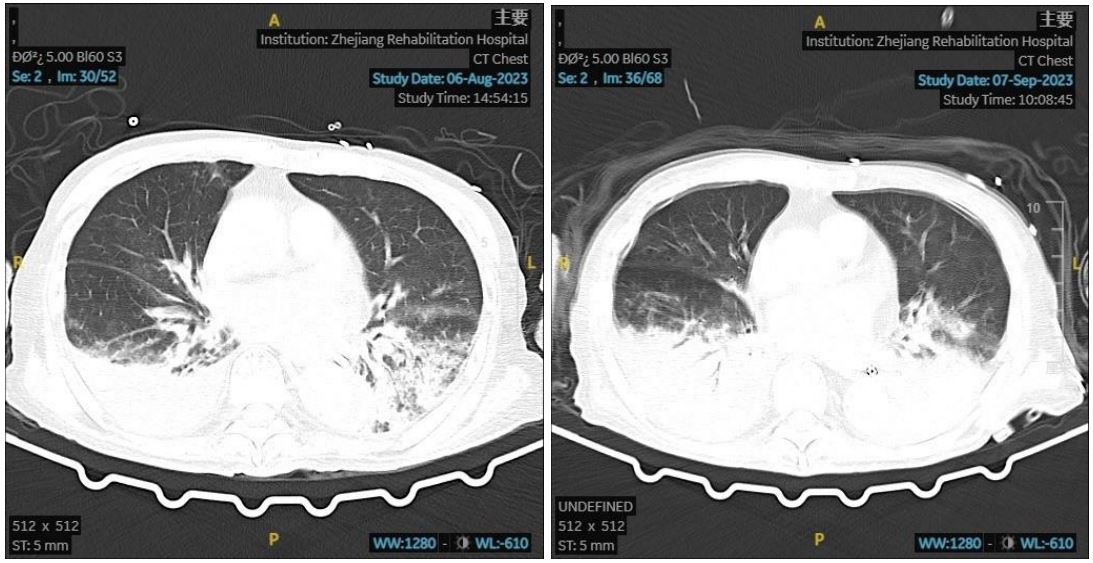
Figure 2: His CT results before and after.
Our second patient is a 74 year old man, he was admitted in our ward for the infection caused by the deep venous puncture in one nursing home which inserted into the abdominal cavity. He had ischemic infarction and coronary atherosclerotic heart disease, and he followed the strict medicine plan. He had a partial gastrectomy surgery 40 years ago, and he had a gastric tube as well this time. He also had the dermotosis which was diagnosis with urticaria by our dermatologist. His blood test was gradually back to normal after one course of treatment. However, he has the aspiration accidentally during his meal and oxygen saturation dropped suddenly, we did the tracheal cannula for him and sent to the intensive care unit immediately. Unfortunately, he was failure to survive this time.
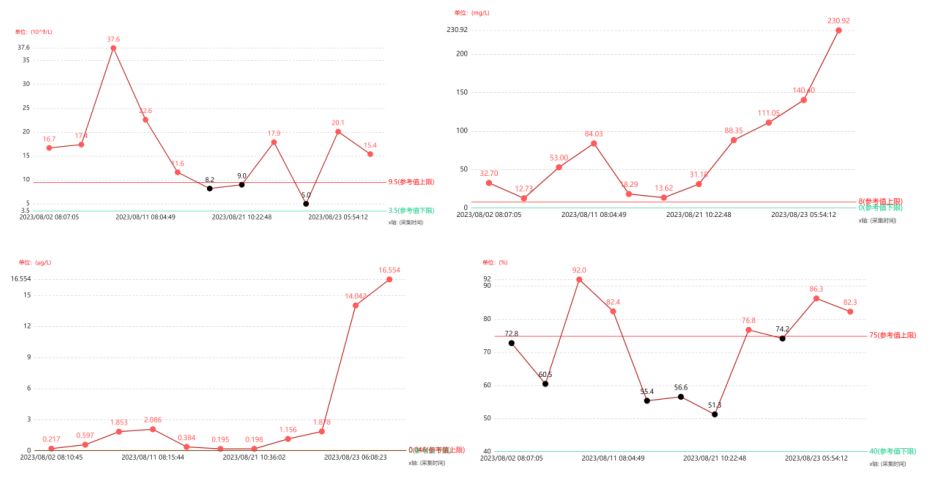
Figure 3: His WBC, N%, CRP and PCT trend figure as follows.
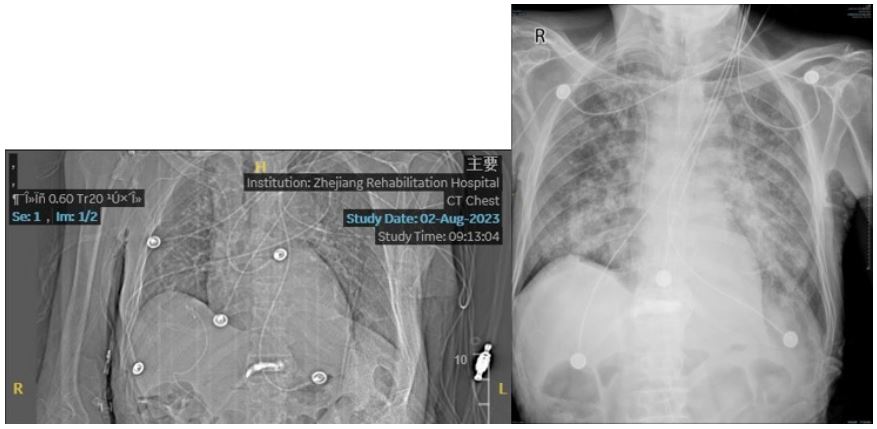
Figure 4: His bedside X-ray results before and after.
Our third patient was a 81 year old man, he was admitted in our department for the covid-19 rehabilitation. He had chronic heart failure and atrial fibrillation, he had diuretic, Xa factor inhibitor and beta block regularly. He had tracheotomy during the COVID-19 infection for the respiratory failure, and we did some preparation work to remove the tracheotomy tube on his throat during this admittance. One day, he felt thirsty and asked for grape juice to drink, and he aspirated the juice unluckily. His vital sign was unstable and we transferred him to the ICU immediately for further treatment, he survived this aspiration attack at last.
Discussion
Aspiration is rather common in elderly patients, it has been reported that approximately 80% of patients with pneumonia aged >70 years are caused by aspiration1. it could be fatal to some fragile patients in a hidden way, and it occurred in our three patients last month. Unfortunately, only [1] patient survived. Here are our reflections about those incidences.
Our [3] patients are all lean figure, and had BMI less than [19]. Some study showed that lower BMI might correlate with infection and it could lead to a poor prognosis once infected [2,3]. Lake et al study revealed that it might impair interleukin-12 (IL-12)/Interferon-γ (IFNγ) Pathway which is closely related with the infection process [4]. It could be an important factor in these elderly patient who were pretty susceptible to bacteria infection. Therefore, we should be vigilant to lower BMI patient and formulated a detailed nutrient diet plan with dietician in early stage in case they had similar circumstances, especially for those high risk ones.
Dieticians usually suggested that those patients should supplement Enteral Nutrition Emulsion (TPF) cause it has complete nutrient component and is more digestive for elderly patients [5], and so did we for these patients. However, we might overlook that velocity of TPF, and default performed a regular speed at 50 ml per hour. However, it might be too fast for these elderly patient, not mention to most of them are bedridden and had poor gastric digestive ability. It might accumulated in the stomach when too fast, especially when they are under other illness condition like hematogenous infection and more likely accompany with intestinal peristalsis. Thus, we recommend that velocity of TPF should be suitable to every patient and it might be better when they are at semireclining position instead supine. As the writer composed this article, another event almost happened in another 80 year old patient, thanks for our nursing worker found and corrected in time this time.
Another high risk factor is impaired swallowing ability. Some studies showed that dysphagia, occurred in 11–14% of adults ≥65 years of age and 36% of residents in the skilled nursing setting [6-8]. Although it is said feeding tube might be safer for these patient, it perhaps impair the medicine efficacy and bioavailability [9,10]. More important, we might ignored the fact long-term feeding tube might impair the patients’ swallowing ability covertly, and our physician usually neglected the patients impaired function. henceforth, physician should pay more attention to those long-term feeding tube patients in case they got aspirated accidentally. Additionally, we should perform the deglutition training regularly for these patient consciously for precaution of aspiration.
Another point to note is that patients with a partial gastrectomy surgery history is more prone to get aspirated, for that they might afflicted with gastrointestinal motility after operation. Alexander et al’ [12] study showed that nearly 25% of these patient had such gastric stasis problem for the disturbance of slow wave in gastrointestinal tissue possibly, which it also present in our two patients. In conclusion, physician should be alert to those elderly patient with gastrectomy history, the velocity of eternal nutrition solution should be adjusted to a receptacle mode according every individuals, and we should perform the deglutition training regularly for these patient in advance.
Acknowledgements: The author would thanks to our staff who dedicated their time and energy for our patients recovery and also pay respect to people who would likely to focus on the elderly patients’ health issue and hope we could improve it together in future.
References
- Teramoto S, Fukuchi Y, Sasaki H, Sato K, Sekizawa K, Matsuse T. Japanese Study Group on Aspiration Pulmonary Disease High Incidence of Aspiration Pneumonia in Community- and Hospital-Acquired Pneumonia in Hospitalized Patients: A Multicenter, Prospective Study in Japan. J. Am. Geriatr. Soc. 2008; 56: 577-579.
- Song JH, Kim BS, Kwak N, Han K, Yim JJ. Impact of body mass index on development of nontuberculous mycobacterial pulmonary disease. The European respiratory journal. 2021; 57(2). 2000454. https://doi.org/10.1183/13993003.00454-2020.
- Kang, J. Y, Han, K, & Kim, M. K. Severity of underweight affects the development of nontuberculous mycobacterial pulmonary disease; a nationwide longitudinal study. Scientific reports, 2022; 12(1). 17180. https://doi.org/10.1038/s41598-022-21511-x.
- Lake MA, Ambrose LR, Lipman MC, et al. “Why me, why now?” Using clinical immunology and epidemiology to explain who gets nontuberculous mycobacterial infection. BMC Med. 2016; 14: 54.
- Brito-de la Fuente, E, Muñiz-Becerá, S, & Ascanio, G. Lipid emulsions in clinical nutrition: Enteral and parenteral nutrition. Advances in food and nutrition research. 2023; 105: 301-342. https://doi.org/10.1016/bs.afnr.2022.12.003.
- Wolf U, Eckert S, Walter G, et al. Prevalence of oropharyngeal dysphagia in geriatric patients and real-life associations with diseases and drugs. Sci Rep. 2021; 11: 21955.
- Roy N, Stemple J, Merrill RM, et al. Dysphagia in the elderly: preliminary evidence of prevalence, risk factors, and socioemotional effects. Ann Otol Rhinol Laryngol. 2007; 116: 858-65.
- Holland G, Jayasekeran V, Pendleton N, et al. Prevalence and symptom profiling of oropharyngeal dysphagia in a community dwelling of an elderly population: a self-reporting questionnaire survey. Dis Esophagus. 2011; 24: 476-80.
- Williams NT. Medication administration through enteral feeding tubes. Am J Health Syst Pharm. 2008; 65: 2347-57.
- White R, Bradnam V. Handbook of drug administration via enteral feeding tubes. 3rd ed. London: Pharmaceutical Press. 2015.
- Fich A, Neri M, Camilleri M, Kelly KA, Phillips SF. Stasis syndromes following gastric surgery: clinical and motility features of 60 symptomatic patients. Journal of clinical gastroenterology. 1990; 12(5): 505-512.
