
Open Access, Volume 9
Twin reverse arterial perfusion sequence: A case report and literature review
John H Dickson1; Wekere FCC2*; Ngeri B2; Sapira-Ordu L2; John AD1,2; Eli S2; Mba AG2; Tamunokoro TN2; Bema Kpoobari2; Wadi Innocent2; Okah Kingdom2
1Department of Obstetrics and Gynaecology, Rivers State University Teaching Hospital, Port Harcourt, Rivers State, Nigeria.
2Department of Family Medicine, University of Port Harcourt, Rivers State, Nigeria.
Wekere FCC
Department of Family Medicine, University of Port Harcourt, Rivers State, Nigeria.
Email: fccwekere@yahoo.com
Received : Sep 18, 2023,
Accepted : Oct 27, 2023
Published : Nov 02, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Twin reverse arterial perfusion sequence (TRAPS) is one of the complications of monochorionic twin gestation. It is characterised by large intertwined arterial-arterial anastomosis in which blood flows from one twin (pump twin) to the other twin (perfused twin) In a retrograde pattern.
We report a case of monochorionic diamniotic twin gestation complicated by TRAPS in a 38-year-old G4P3 trader who was referred to the antenatal clinic of Rivers State University Teaching Hospital on account of unusual abdominal distension of one-week duration at 31 weeks gestational age. Ultrasound scan done at presentation showed a monochorionic diamniotic twin with the first twin in a transverse lie with an estimated foetal weight of 1.7kg, foetal heart rate of 150 beats per minute, and Twin 2, had no foetal head, no cardiac pulsation with significant tissue swelling. A diagnosis of TRAPS was made for which she was admitted and delivered by emergency caesarean section. The pump twin was admitted into the Special Care Baby Unit (SCBU) And succumbed to cardiac failure 24 hours after delivery.
Monochorionic pregnancy complicated by TRAPS is associated with poor foetal outcomes. Early diagnosis and adequate management will enhance clinical outcomes. The diagnosis of TRAPS requires a high index of suspicion. Clinicians and radiologists need to be aware of the features in order to make prompt diagnosis and take appropriate action which may include early referral to the fetal medicine unit for appropriate intervention and improved outcome for the pump twin.
Keywords: Blood; Case report; Diagnosis; Cardiac failure.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Wekere FCC (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Dickson JH, Wekere FCC, Ngeri B, Sapira-Ordu L, John AD, Eli S, Mba AG, et al. Twin reverse arterial perfusion sequence: A case report and literature review. Open J Clin Med Case Rep. 2023; 2146.
Introduction
Monochorionic twins are prone to a variety of complications due to vascular abnormality of the single placenta supplying the twin. These complications include twin-twin transfusion syndrome, twin anaemia/ polycythaemia, twin reversed arterial perfusion sequence amongst others [1-3]. TRAPS is a condition characterised by large intertwined arterial-arterial anastomosis in which blood flows from one twin (pump twin) to the other twin (perfused twin) in a retrograde pattern. As a result, the perfused twin- the parasite receives the deoxygenated arterial blood from the pump twin leading to a complete acardia (holocardiac) or rudimentary non-functional heart (hemicardiac) [1]. TRAPS is a rare complication affecting 1% of monochorionic twin pregnancy [6] and [1] of 35000 pregnancies [7,8]. However, with the spread of assisted reproductive technology and improved diagnostic ultrasonography, the incidence of TRAPS is increasing towards 2.6% of monozygotic twins and [1] of 9500 to 11000 pregnancies [9,10].
The ultrasound finding suggestive of TRAPS is the demonstration at colour Doppler of a paradoxical circulation in the acardiac twin with arterial blood flowing towards rather than away and a caudal to cranial course in the abdominal aorta [7]. Early diagnosis and intervention could savage 85% of cases, but with a late diagnosis, a substantial proportion die in utero at about 18 weeks of gestation and about 55% are lost in later gestational age or early neonatal period [1]. The main goal of treatment is to preserve the survival of the pump twin who is at increased risk of morbidity and mortality from cardiac failure and or sequelae of prematurity [9]. We report a case of TRAPS diagnosed in the third trimester, had caesarean section but the pump twin succumbed to cardiac failure 24 hours after delivery.
Case Presentation
Mrs N.P was a 38-year-old G4P3 trader who was referred to the antenatal clinic of Rivers State University Teaching Hospital on 13/04/22 on account of unusual abdominal distension of one-week duration at 31 weeks gestational age. Her last mensural period was on 21/09/21. The abdominal swelling was rapidly progressive over a one-week period. There was no history of reduction in urine output, and no early morning facial puffiness. There was associated difficulty breathing but no history of cough, chest pain, or fever. An early ultrasound scan done at 12 weeks had shown a monochorionic diamniotic twin. An ultrasound scan done at the onset of symptoms showed a single active foetus with associated complex huge mass and polyhydramnios. The antenatal period was uneventful before the onset of the above complaint.
On examination, she was dyspnoeic, not pale, and not cyanosed. The respiratory rate was 28 cycles per minute, though the chest was clinically clear. The pulse rate was 90 beats per minute and the blood pressure was 124/72 mmHg. Her abdomen was markedly enlarged, and there were no areas of tenderness. The symphysio-fundal height was 42 cm and is greater than her 31 weeks gestational age. The foetal parts were difficult to palpate and the foetal heart sounds were not heard with a pinard stethoscope. A diagnosis of twin gestation with polyhydramnios? cause was made.
She was admitted into the antenatal ward and nursed in cardiac position. Packed cell volume was 33%, and a repeat ultrasound scan with the Doppler study showed a monochorionic diamniotic twin. Twin 1 was in a transverse lie with an estimated foetal weight of 1.7 kg, foetal heart rate of 150 beats per minute. Twin 2, had no foetal head, no cardiac pulsation with significant tissue swelling. A diagnosis of TRAPS was made.
She received two doses of dexamethasone 12 mg 12 hours apart. A biophysical profile done on 22/04/22 showed a score of 6/10 hence, the patient was counselled on abdominal delivery and she subsequently had a caesarean section on 22nd April 2022. The outcome of the surgery was Twin 1; a live male baby with APGAR scores 8 and 9, birth weight 1.55 kg (Figure 1), And Twin 2 was a severely malformed baby with absent head and upper limbs, weight of 3.2 kg (Figure 2a-c). The single placenta weight was 1.2 kg, the estimated blood loss was 800 ml.
The baby was sent to SCBU for neonatologist evaluation and management however baby died 24 hours later.

Figure 1: The Pump Twin.

Figure 2: Ventral view of the acardiac twin.

Figure 3: Dorsal view of the acardiac twin.
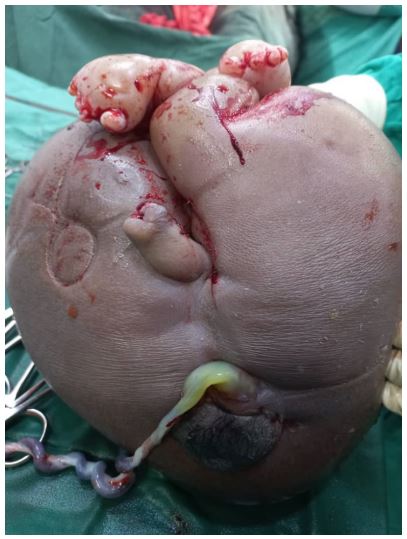
Figure 4: Side view of the acardiac twin.
The parturient was transfused on the second postoperative day based on a packed cell volume of 21%. She received parenteral and oral antibiotics, analgesics, and haematinics. She had an uneventful postpartum recovery and was discharged home on the 5th postoperative day. She was seen at 2 weeks and 6 weeks post-delivery at the post-natal clinic and had no complaints. Her examination findings were satisfactory. Hence, she was discharged to the family planning clinic for uptake of contraception.
Discussion
TRAPS is a condition unique to monochorionic twin [1]. Its incidence is on the increase due to early detection on first-trimester ultrasound scans and increased use of assisted reproductive technology [10]. It is characterised by an acardiac twin with lack of complete cardiac structures perfused by an apparently normal co-twin (the pump twin) which supplies both circulations [11]. The acardiac twin loses direct vascular connection with the placenta villa, thus depending on the pump twin for its supply. The supplied deoxygenated blood perfuses the lower part of the foetus and the upper structures atrophies [9,12]. The pump twin bears the burden of perfusing the acardiac twin thus it is at increased risk of mortality from high output cardiac failure. Hence, the need for early ultrasound screening of monochorionic twins, diagnosis, and appropriate intervention to improve perinatal outcomes.
A pathognomic finding is the demonstration at colour Doppler of a paradoxical circulation in the acardiac twin, with arterial blood flowing towards rather than away and a caudal to cranial course in the abdominal aorta (even evident during the first trimester) [7]. Langlotz et al., suggested this peculiar Doppler findings of reverse anastomosis in the first case of TRAPS. In later gestation there is absence of identifiable cardiac pulsation, poorly defined head, trunk and upper extremities. These featured were seen in the foetus. There might be marked oedema and cystic changes in the upper body [7,13].
Morphologically, the acardiac twin is classified as (i) Acardia cephalus (ii) Acardiacacornus (iii) Acardia amorphous (iv) Acardiac anceps [7,10,13]. The case presented was acardia-cephalus, similar to findings in the case reported by Badoe EV et al. It is the commonest sub type of TRAPS [6,14].
Mrs N.B. had monochorionic twin diagnosed at twelve weeks on ultrasound scan, however, features of TRAPS were not recognised by the sonographers. More so, the anomaly scan was missed in the course of the antenatal care. The repeat ultrasound scan done at the onset of symptoms noted an absent head and no cardiac pulsation in the parasitic twin. In a case report by Dhanju G et al, though the first-trimester ultrasound scan missed the diagnosis, the anomaly scan clenched on the diagnosis [10]. The main goal of early intervention is to preserve the pump twin and advance pregnancy to near term as possible. Management options are majorly conservative, palliative and invasive treatment. The choice is determined by the gestational age, availability of the requisite skills and specialized equipment. Palliative treatment involves prolongation of pregnancy by amnio-reduction. The conservative management and follow up involves using ultrasound scan surveillance and intervening when there is evidence of pump twin compromise, or severe over growth of the acardiac twin [5,7]. Rohilla M et. al and Sepulvecla et. al recommended conservative management with surveillance for salvage of the pump twin when the acardiac twin is less than ¼th the weight of the pump twin. Otherwise, invasive intervention is advised. In the past, early treatment modalities were reserved for pregnancies >16/52 gestational age due to poorly designed devices for invasive interventions. However, with the advent of minimally invasive techniques, inventions can be instituted earlier than 16/52 gestational age. Intervention options that can be implemented at earlier gestations include cord coagulation, cord ligation, photo coagulations, intrafoetal radiofrequency ablation, LASER therapy, and HIFU [9,14,15]. Out of all the modern techniques to treat TRAP, some authors Antonio D et al and Livingstone JC et al signified RFA as the most effective with high safety index. Though these treatment modalities are not available in most centres in our vicinity, patients could have conservative management with recourse to early delivery or early referral to neighbouring states with manpower and facility to manage the case. For Mrs N.B, attempt at conservative management was terminated based on features of compromise noted in the pump twin.
A study by Sugibayashi R et al, found that a survival of ≥80% for the pump twin can be achieved with early intervention. Quaas et al [6] in a case series buttress the benefit of early intervention and appropriate management by the foeto-maternal specialist. The overall survival for intervention using infrafoetal laser treatment was 88.9%-91.7% with low loss rates reports by Tavares de souse et al and Berg C et al. [1,9]. However, if undiagnosed a high proportion die in utero and about 50%-70% will be lost in later gestation [5]. Features of poor prognosis for the pump twin include delivery before 32 weeks, a large acardiac twin hydrops, polyhydramnios presence of well-developed upper extremities in the acardiac twin [7]. Mrs N.B had elective caesarean delivery at 32 weeks, and outcome was acardiac twin (weighed 3.2 kg) and a live male 1.7 kg baby who died of cardiac failure within 24 hours of delivery.
Conclusion
The diagnosis of TRAPS requires a high index of suspicion by radiologists and obstetricians. Early diagnosis and intervention may improve outcomes for the pump twin. Appropriate action may include early referral to the foetal medicine unit.
References
- Berg C, Holst D, Mallmann MR, Gottschalk I, Gembruch U, Geipel A. Early vs late intervention in twin reversed arterial perfusion sequence. Ultrasound in Obstetrics & Gynecology. 2014; 43(1): 60-4.
- Sueters M, Oepkes D. Diagnosis of twin-to-twin transfusion syndrome, selective fetal growth restriction, twin anaemia-polycythaemia sequence, and twin reversed arterial perfusion sequence. Best Practice & Research Clinical Obstetrics & Gynaecology. 2014; 28(2): 215-26.
- Osaghae DO, Unuigbe JA. Transfusion syndromes in monochorionic multiplets: An overview. Tropical Journal of Obstetrics and Gynaecology. 2016; 33(2): 135-42.
- Pagani G, D’antonio F, Khalil A, Papageorghiou A, Bhide A, Thilaganathan B. Intrafetal laser treatment for twin reversed arterial perfusion sequence: cohort study and meta-analysis. Ultrasound in Obstetrics & Gynecology. 2013; 42(1): 6-14.
- Bukar M, Kwari SD, Bilkisu I, Mahmud MG, Obed JY. Acardiacacephalus twin: A case report. Tropical Journal of Obstetrics and Gynaecology. 2012; 29(1): 131-3.
- Sugibayashi R, Ozawa K, Sumie M, Wada S, Ito Y, Sago H. Forty cases of twin reversed arterial perfusion sequence treated with radio frequency ablation using the multistep coagulation method: a single-center experience. Prenatal diagnosis. 2016; 36(5): 437-43.
- Adamou N, Yakasai I. Twin reverse arterial perfusion (TRAP): Case report. Open Journal of Obstetrics and Gynecology. 2014; 4(16): 1072-6.
- Cabassa P, Fichera A, Prefumo F, Taddei F, Gandolfi S, Maroldi R, Frusca T. The use of radiofrequency in the treatment of twin reversed arterial perfusion sequence: a case series and review of the literature. European Journal of Obstetrics &Gynecology and Reproductive Biology. 2013; 166(2): 127-32.
- Tavares de Sousa M, Glosemeyer P, Diemert A, Bamberg C, Hecher K. First-trimester intervention in twin reversed arterial perfusion sequence. Ultrasound in Obstetrics &Gynecology. 2020; 55(1): 47-9.
- Dhanju G, Breddam A. Twin reversed arterial perfusion (TRAP) sequence: A case report and a brief literature review. Radiology Case Reports. 2022; 17(5): 1682-91.
- Oluwafemi RO, Owa O. Acepii Alic Nigerian Newborn: A Case Report. Ann Biomed Sci. 2019; 18(2).
- Shettikeri A, Acharya V, Shailaja V, Sahana R, Radhakrishnan P. Outcome of pregnancies diagnosed with TRAP sequence prenatally: a single-centre experience. Fetal Diagnosis and Therapy. 2020; 47(4): 301-6.
- Badoe EV, Darko A, Atuguba BH. Case Report: Twin Reversed Arterial Perfusion Sequence in a Triplet Natural Pregnancy: Case Report from Korle Bu Teaching Hospital, Accra, Ghana and a Review of the Literature. West African Journal of Medicine. 2013; 32(1): 73-5.
- Boele CO, Johnson A; twin reversed arterial perfusion sequence: Best practice and research clinical Obstetrics and Gynaecology. 2022; 84: 127-42.
- Rohilla M, Chopra S, Suri V, Aggarwal N, Vermani N. Acardiac-acephalus twins: a report of 2 cases and review of literature. The Medscape Journal of Medicine. 2008; 10(8): 200-208.
- Sebire NJ, Wong AE, Sepulveda W. Minimally invasive management of twin revered arterial perfusion sequence (TRAP). Fetal and Maternal Medicine Review. 2006; 17(1): 1-22.
- Chaveeva P, Poon LC, Sotiriadis A, Kosinski P, Nicolaides KH. Optimal method and timing of intrauterine intervention in twin reversed arterial perfusion sequence: case study and meta-analysis. Fetal diagnosis and therapy. 2014; 35(4): 267-79.
- Okai T, Ichizuka K, Hasegawa J, Matsuoka R, Nakamura M, Shimodaira K, Sekizawa A, Kushima M, Umemura S. First successful case of non-invasive in-utero treatment of twin reversed arterial perfusion sequence by high-intensity focused ultrasound. Ultrasound in Obstetrics & Gynecology. 2013; 42(1): 112-4.
- Livingston JC, Lim FY, Polzin W, Mason J, Crombleholme TM. Intrafetal radiofrequency ablation for twin reversed arterial perfusion (TRAP): A single-center experience. American journal of obstetrics and gynecology. 2007; 197(4): 399-e1.
- Scheier M, Molina FS. Outcome of twin reversed arterial perfusion sequence following treatment with interstitial laser: a retrospective study. Fetal diagnosis and therapy. 2012; 31(1): 35-41.
