
Open Access, Volume 9
Rotavirus vaccination coverage before and during the covid-19 pandemic in Fako division, Cameroon
Beatrice Ameh Tangunyi Loh1 *; Valentine Ngum Ndze²; Anye Delphine Tangoh³; Nyingchu Robert Vuchuh⁴; Godlove Bunda Wepnje⁵
1Department of Medical Laboratory Science, University of Buea, Cameroon.
2Department of Public Health, University of Buea, Cameroon.
3Department of Medical Laboratory Science, University of Buea, Cameroon.
4Department of Medical Laboratory Science, University of Buea, Cameroon.
5Department of Zoology and Animal Physiology, University of Buea, Cameroon.
Beatrice Ameh Tangunyi Loh
Department of Medical Laboratory Science, University of Buea, Cameroon.
Email: beatriceameh@gmail.com
Received : Sep 18, 2023,
Accepted : Oct 26, 2023
Published : Nov 02, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Rotavirus vaccines aim to reduce morbidity and mortality associated with severe gastroenteritis. Repeat infections are common but less severe than the primary infection. Rotarix vaccine is given orally in two doses at 2 and 4 months of age in Cameroon. Rotavirus remained a threat to the health of young children during the COVID-19 pandemic and many parts of the world witnessed a decline in vaccine coverage during this pandemic. We sought to find out If the story was the same in Fako Diivision, Cameroon, amidst a sociopolitical conflict.
Methods: A retrospective study was done in 4 hospitals on Rotavirus immunization records of children under 5 from 2016-2022. Stratified sampling used, descriptive stats reported. Differences evaluated with Pearson’s chi square (P<0.05).
Results: 61.6% of children vaccinated, 80% received 2 doses, 3.4% late vaccination. Highest rate in age group 0-5 months (66.2%). More vaccinated during Covid (62.7%) Than before (57.7%). Same trend at National (78% during and 51% before) And Regional (67% during and 24% before) levels.
Discussion: 80% vaccination rate is below WHO target. There was increased uptake of Rotavirus vaccine during the COVID-19 season at all levels in the country, indicating relative stability in trends of children vaccination programs throughout the country. Late vaccination rates were lower than expected.
Conclusion: Rotavirus vaccination saw an increase in trend during the COVID-19 season in Fako Division. This study informs Global and national policy makers about this unexpected increased vaccine uptake at all levels in Cameroon.
Keywords: COVID-19; Vaccines; Infections; Health; Children.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Beatrice Ameh TL (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Beatrice Ameh TL, Valentine NN, Anye DT, Nyingchu RV, Godlove BW. Rotavirus vaccination coverage before and during the covid-19 pandemic in Fako division, Cameroon. Open J Clin Med Case Rep. 2023; 2145.
Introduction
Rotavirus is in the family Reoviridae and is a genus of double-stranded RNA viruses [1]. The viral particle has three layers covering the genome. With the outermost shell containing two important proteins: VP7, or G-protein, and VP4, or P-protein. VP7 and VP4 induce neutralizing antibodies that are thought to be involved in immune protection [2]. Rotaviruses are the causes most of the severe, dehydrating diarrhea in children less than 5 years of age globally. Three-quarters of children acquire their first episode of Rotavirus diarrhea before the age of 12 months in developing countries [3,4]. Rotaviruses are excreted in exceedingly high concentrations and persist for numerous days in both feces and vomit of infected persons [5]. Transmission primarily occurs through the fecal-oral route, either via direct person-to-person contact or indirectly through contaminated fomites [6]. The transmission of rotavirus is remarkably contagious, and its incubation period commonly spans 48 hours. Throughout this timeframe, the virus may be excreted in the fecal matter of an asymptomatic individual [7]. Rotavirus is global. Improved sanitation alone cannot prevent infection in children under 5 [2].
Repeat Rotavirus infections are less severe but common, leading to the development of vaccines to reduce morbidity and mortality [8,9]. Two live, oral rotavirus vaccines are currently licensed for use, RV5 (RotaTeq) and RV1 (Rotarix) vaccines [2]. Rotarix is an attenuated human virus while RotaTeq is a pentavalent product With reassortant virus from human and bovine origin [10,11].
Vaccine mode of action: As a multi-dose oral agent, existing vaccines are believed to specifically stimulate the production of IgA in the gastrointestinal tract, which is where infections typically occur [7,12].
Vaccination schedule and administration: RotaTeq (RV5) is given in three doses at 2 months, 4 months, and 6 months of age while Rotarix (RV1) is given in two doses at 2 months and 4 months of age. The first dose of either vaccine should be given before a child is 15 weeks of age. Also, children should receive all doses of rotavirus vaccine before they turn 8 months old. Both vaccines are given orally by putting drops in the infant’s mouth [13,14]. In Cameroon, Rotarix™ was introduced in March 2014 [15]. According to the WHO vaccination schedule for Cameroon, the first dose is given at four weeks and the second dose at six weeks [16].
Rotavirus vaccination in the presence of covid-19 and sociopolitical conflict: Vaccine-preventable childhood diseases did not go away during the COVID 19 pandemic and rotavirus remained a threat to the health of young children [17]. Globally, preliminary data from the first 4 months of 2020 indicated a decline in diphtheria-tetanus-pertussis coverage, generally considered the marker of vaccination coverage across countries [18]. The Centers for Disease Control and Prevention (CDC) Also reported a decline in vaccine coverage during the COVID-19 pandemic in April 2020 in the state of Michigan in the United States [19]. Delivery of immunization services was also limited due to the prioritization of COVID-19 patients [20]. The Anglophone crisis in Cameroon which started in 2016 as a small protest degenerated to a full-blown armed conflict between separatists and the government, with far reaching effects especially on the healthcare system [21]. We sought to find out if the general low trend in vaccine coverage during COVID-19 held true for Fako Division of Cameroon, particularly for Rotavirus, a relatively new vaccine and in the face of a sociopolitical war.
Methods
This was a retrospective cross-sectional study carried out in four hospitals within the Fako Division of the South West Region of Cameroon where there is little or no data on Rotavirus vaccination coverage. This Division is cosmopolitan with children from all socioeconomic and cultural backgrounds. The study population included Rotavirus immunization records in four hospitals from the year 2016 to 2022 of children less than 5 years of age. National and Regional Rotavirus vaccination data was collected from the South West Delegation of Public Health. Sample size of 500 was calculated with inspiration from a study by Ndze et. al. on Rotavirus among children less than five years of age in the North West region of Cameroon [22]. The stratified sampling method was used. Continuous variables were summarized into means and standard deviations while categorical variables reported as frequencies and percentages were used to evaluate the descriptive statistics. The differences in proportions were evaluated using Pearson’s chi square (X²). Level of significance was set at P<0.05.
Results
Characteristics of children <5 years vaccinated before and during Covid
A total of 237 children reported for vaccination before and during Covid as shown in (Table 1). The median age was 2.0 months (range: 0.03 – 24 months) With a majority (56.15) Of the children being males. Most of the children were in the age group 0 – 5 months (84.8%). Vaccination was reported among 61.6% of the children and more than 80% had received 2 doses. The rate of late vaccination was 3.4% (8/237).
Table 1: Characteristics of children <5 years.
| Variable | Category | %(n) |
|---|---|---|
| Sex | Male | 56.1(133) |
| Female | 43.9(104) | |
| Age group (months) | 0 – 5 | 84.8(201) |
| 6 – 11 | 11.8(28) | |
| 12 – 18 | 3.0(7) | |
| 19 – 35 | 0.4(1) | |
| Vaccinated | Yes | 61.6(146) |
| No | 38.4(91) | |
| Number of doses | One | 17.1(25) |
| Two | 82.9(121) |
Association between vaccination coverage, sex and age: Male children were more vaccinated than females (63.2% vs 59.6%). However, the difference was not significant (P = 0.578) as shown in (Table 2). Vaccination was significantly associated with age group with children 0-5 months recording the highest number of vaccination (66.2%) When compared with the other age groups. Children 19 – 35 months did not receive any vaccination. Dose of vaccination correlated positively with age (r = 0.199; P = 0.016).
Table 2: Vaccination coverage with respect to sex and age.
| Variable | Vaccinated %(n) | Unvaccinated %(n) | Chi square; P value |
|---|---|---|---|
| Sex | |||
| Male | 63.2(84) | 36.8(49) | 0.310; 0.578 |
| Female | 59.6(62) | 40.4(42) | |
| Age group in months | |||
| 0 – 5 | 66.2(133) | 33.8(68) | |
| 6 – 11 | 39.3(11) | 60.7(17) | 12.501; 0.006 |
| 12 – 18 | 28.6(2) | 71.4(5) | |
| 19 – 35 | 0.0(0) | 100.0(1) | |
Rotavirus Vaccination coverage before and during COVID-19(Fako Division): Although the difference was not significant, more children were vaccinated during Covid (62.7%) Than before Covid (57.7%) as shown in (Figure 1). There was a significant increase in the number of doses of the vaccine before and during Covid (Table 5). More of one and two doses of the vaccine was recorded during Covid (60.0% and 83.5% respectively).
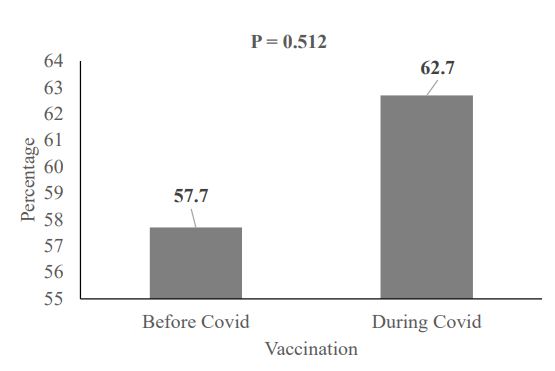
Figure 1: Vaccination coverage before and during
COVID-19 (Fako Division).
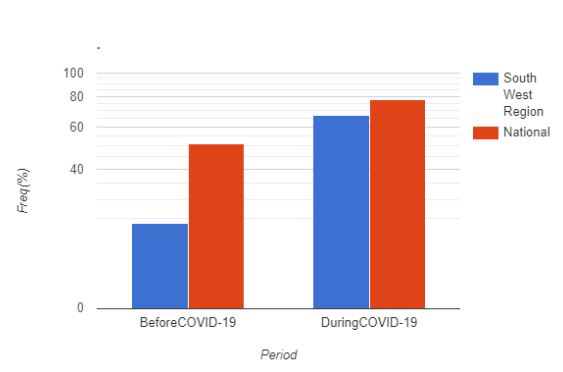
Figure 2: Regional and National Rotavirus vaccine
coverage (before and during COVID-19).
Regional and National Rotavirus vaccine coverage (before and during COVID-19)
As shown in (Figure 2), Rotavirus vaccination coverage was higher during the COVID-19 season (78%) Than before (51%) at the national level. The same trend is seen at the regional level with rate rising from 24% before to 67% during the COVID-19 season. The difference was not significant (P=0.596).
Table 3: Number of doses received before and during Covid.
| Number of doses | Vaccination status | Chi square; P value | |
|---|---|---|---|
| Before Covid % (n) | During Covid %(n) | ||
| One | 40.0(10) | 60.0(15) | 6.991; 0.008 |
| Two | 16.5(20) | 83.5(101) | |
Table 4: Vaccination coverage before and during Covid stratified by age and sex.
| Sex | Number of children vaccinated | Proportion of children vaccinated (%) | P value | ||
|---|---|---|---|---|---|
| Before Covid | During Covid | Before Covid | During Covid | ||
| Male | 19 | 65 | 22.6 | 77.4 | 0.611 |
| Female | 11 | 51 | 17.7 | 82.3 | 0.640 |
| Age group (months) | |||||
| 0 – 5 | 23 | 110 | 17.3 | 82.7 | 0.195 |
| 6 – 11 | 5 | 6 | 45.5 | 54.5 | 0.225 |
| 12 – 18 | 2 | 0 | 100.0 | 0.0 | 0.053 |
| 19 – 35 | 0 | 0 | 0 | 0 | - |
Vaccination coverage before and during Covid stratified by sex and age. Vaccination coverage with respect to sex was not significantly different before and during Covid. However, 77.4% and 82.3% of males and females were vaccinated during Covid. Children in the 0-5 months recorded the highest vaccination coverage of 82.7% during Covid as compared to 17.3% before Covid. No child in the 19-35 months was vaccinated before and after Covid, meanwhile, no child in the 12-18 months was vaccinated during Covid as shown in (Table 4).
Discussion
A vaccination rate of 80% is better than the national rate for Cameroon which stood at 65% in 2021 [23]. It is also higher than the 78.60% reported in a study done in two health Districts of Ethiopia [24]. This higher rate in our study area can be accounted for by the huge influx of internally displaced people into our study area, leading to exaggerated figures. This coverage isas well higher than would have been seen if Rotareq, a three-dose vaccine was used. Raju et al. [25] Reports that the two-dose vaccine may have advantages over three-dose vaccines in terms of earlier schedule completion and higher compliance because some children may choose not to receive the third dose. A few children took late doses of vaccine (3.4%), In variance to reports the UNICEF which states, “the COVID-19 pandemic severely disrupted childhood immunization, with 67 million children missing out entirely or partially on routine immunization between 2019 and 2021” [26]. We expected many of the internally displaced children who must have missed taking the vaccine to take late doses but because the vaccine is restrictive of age, they must have missed out completely. It is recommended that the vaccination should be finished by the 32nd week [23]. Interestingly, more children were vaccinated during the COVID-19 season (62.7%) Than before (57.7%) Although the difference was not significant (P=0.512). This is contrary to a report by preventrotavirus which say the COVID-19 pandemic has greatly impacted routine immunization and data collection such that across the world, vaccination coverage for all routine immunizations has decreased in 2020, including for rotavirus vaccine (preventrotavirus.org, n.d.). It is as well contrary to a study in Brazil which reported a decline in Rotavirus vaccine coverage during the COVID-19 season [27].
Conclusion
This study shows a consistent increase in Rotavirus vaccine uptake during the COVID-19 season than before at all levels (National, Regional and at the Divisional level). This goes as an indication to policy makers that in spite of the generally low vaccine coverage reported in other parts of the world, Cameroon reported and increase in coverage. This serves as an indicator for all other children’s vaccines in Cameroon. We recommend an adjustment on the age for vaccination to include older children who missed a dose so that in case of a pandemic like COVID-19 or a sociopolitical conflict as experienced in our study area, affected children should not miss out on their immunization completely.
Declarations
Declaration of interest: The writers have no pertinent associations or fiscal engagements with any establishment or entity that possesses financial stakes in, or discrepancies concerning the subject matter or materials reviewed within this manuscript.
Acknowledgement: We acknowledge Ngwa-Tamu Leonard, Loh Elton Mbah, Djomnang T. Michel Stephane and Tchouanguem Kamle Christ for helping out with data collection.
References
- Gov.au. Available from. 2023. https://immunisationhandbook.health.gov.au/contents/vaccine-preventable-diseases/rotavirus.
- Rotavirus [Internet]. Cdc.gov. Available from. 2022. https://www.cdc.gov/vaccines/pubs/pinkbook/rota.html.3. Yeasmin S, Hasan SMT, Chisti MJ, Khan MA, Faruque ASG, Ahmed T. Factors associated with dehydrating rotavirus diarrhea in children under five in Bangladesh. An urban-rural comparison. PLoS One [Internet]. 2022; 17(8): 0273862. Available from: http://dx.doi.org/10.1371/journal.pone.0273862.
- Rotavirus [Internet]. Who.int. Available from. 2023. https://www.who.int/teams/health-product-policy-and-standards/standards-and-specifications/vaccines-quality/rotavirus
- Nyblade C, Zhou P, Frazier M, Frazier A, Hensley C, Fantasia-Davis A, et al. Human Rotavirus replicates in salivary glands and primes immune responses in facial and intestinal lymphoid tissues of gnotobiotic pigs. Viruses [Internet]. 2023;15(9):1864. Available from: http://dx.doi.org/10.3390/v15091864
- Vardoulakis S, Espinoza Oyarce DA, Donner E. Transmission of COVID-19 and other infectious diseases in public washrooms: A systematic review. Sci Total Environ [Internet]. 2022; 803(149932): 149932. Available from: http://dx.doi.org/10.1016/j.scitotenv.2021.149932.s.
- Skansberg A, Sauer M, Tan M, Santosham M, Jennings MC. Product review of the rotavirus vaccines ROTASIIL, ROTAVAC, and Rotavin-M1. Hum Vaccin Immunother [Internet]. Available from. 2021; 17(4): 1223-34. http://dx.doi.org/10.1080/21645515.2020.1804245.
- Geard N, Bradhurst R, Tellioglu N, Oktaria V, McVernon J, Handley A, et al. Model-based estimation of the impact on rotavirus disease of RV3-BB vaccine administered in a neonatal or infant schedule. Hum Vaccin Immunother [Internet]. Available from. 2022; 18(6). http://dx.doi.org/10.1080/21645515.2022.2139097.
- Report of the regional immunization technical advisory group [Internet]. Who.int. Available from. 2020. https://www.afro.who.int/sites/default/files/202102/WHO%20AFRO%20RITAG%20meeting%20report_July%202020.pdf.
- Global Vaccine safety. Observed rate of vaccine reactions [Internet]. Who.int. Available from. 2023. https://cdn.who.int/media/docs/default-source/pvg/global-vaccine-safety/rotavirus-vaccine-rates-information-sheet-0618.pdf?sfvrsn=fdd3cc44_4&download=true.
- Sadiq A, Bostan N, Khan J, Aziz A. Effect of rotavirus genetic diversity on vaccine impact. Rev Med Virol [Internet]. Available from. 2022; 32(1). http://dx.doi.org/10.1002/rmv.2259.
- Li M, Wang Y, Sun Y, Cui H, Zhu SJ, Qiu H-J. Mucosal vaccines: Strategies and challenges. Immunol Lett [Internet]. . Available from. 2020; 217: 116-25http://dx.doi.org/10.1016/j.imlet.2019.10.013.
- Rotavirus vaccination [Internet]. Cdc.gov. Available from. 2023. https://www.cdc.gov/vaccines/vpd/rotavirus/index.html.
- Hill HA, Yankey D, Elam-Evans LD, Singleton JA, Pingali SC, Santibanez TA. Vaccination coverage by age 24 months among children born in 2016 and 2017-national immunization survey-child, United States, 2017-2019. MMWR Morb Mortal Wkly Rep [Internet]. 2020; 69(42): 1505-11. http://dx.doi.org/10.15585/mmwr.mm6942a1
- Ghapoutsa RN, Boda M, Gautam R, Ndze VN, Mugyia AE, Etoa F-X, et al. Detection of diarrhoea associated rotavirus and coinfection with diarrhoeagenic pathogens in the Littoral region of Cameroon using ELISA, RT-PCR and Luminex xTAG GPP assays. BMC Infect Dis [Internet]. 2021;21(1). Available from: http://dx.doi.org/10.1186/s12879-021-06318-x.
- Who.int. Available from. 2023. https://cdn.who.int/media/docs/default-source/immunization/vpd_surveillance/vpd-surveillance-standards-publication/who-surveillancevaccinepreventable-19-rotavirus-r2.pdf?sfvrsn=2c43bf06_10&download=true
- Defeatdd.org. [cited 2023 Sep 16]. Available from: https://www.defeatdd.org/blog/rotavirus-vaccine-research-time-covid-19.
- Chiappini E, Parigi S, Galli L, Licari A, Brambilla I, Angela Tosca M, et al. Impact that the COVID-19 pandemic on routine childhood vaccinations and challenges ahead: A narrative review. Acta Paediatr [Internet]. Available from. 2021; 110(9): 252-35. http://dx.doi.org/10.1111/apa.15949.
- Bramer CA, Kimmins LM, Swanson R, Kuo J, Vranesich P, Jacques-Carroll LA, et al. Decline in child vaccination coverage during the COVID-19 pandemic-Michigan care improvement registry, may 2016-may 2020. MMWR Morb Mortal Wkly Rep [Internet]. 2020 69(20): 630-1. https://www.cdc.gov/mmwr/volumes/69/wr/mm6920e1.htm.
- Dzinamarira T, Moyo E, Moyo P, Pierre G, Mpabuka E, Kahere M, Tungwarara N, Chitungo I, Murewanhema G, Musuka G. Childhood immunization services accessibility and utilization during the COVID-19 pandemic in Africa. Journal of Infection. 2022 Oct 1;85(4):436-80.
- Niba JO, Ngasa SN, Chang N, Sanji E, Awa AM, Dingana TN, Sama CB, Tchouda L, Julius ME. Conflict, healthcare and professional perseverance. A qualitative study in a remote hospital in an Anglophone Region of Cameroon. PLOS Global Public Health. 2022; 2(11): e0001145.
- Ndze, V. N., Akum, A. E., Kamga, G. H., Enjema, L. E., Esona, M. D., Banyai, K., & Marie Therese, O. A. Epidemiology of rotavirus diarrhea in children under 5 years in Northern Cameroon. PAMJ [Internet]. 2012; 11(73). Available from: https://www.panafrican-med-journal.com/content/article/11/73/fullhttps://doi.org/10.11604/pamj.2012.11.73.1548
- Vanderslott S, Dattani S, Spooner F, Roser M. Vaccination. Our World in Data [Internet]. Available from. 2013. https://ourworldindata.org/vaccination.
- Derso T, Kebede A, Wolde HF, Atnafu A, Dellie E. Rotavirus vaccine coverage and associated factors among a rural population: Findings from a primary health-care project in two northwest Ethiopia districts. Pediatric Health Med Ther [Internet]. Available from. 2020; 11: 429-35. http://dx.doi.org/10.2147/phmt.s276037.
- Parikh R, Raju B, Vetter V, Kolhapure S. Epidemiology of rotavirus gastroenteritis and need of high rotavirus vaccine coverage with early completion of vaccination schedule for protection against rotavirus diarrhea in India. A narrative review. Indian J Public Health [Internet]. Available from. 2019; 63(3): 243. http://dx.doi.org/10.4103/ijph.ijph_307_18.
- The state of the world’s children 2023 [Internet]. Unicef.org. Available from. 2023. https://www.unicef.org/reports/stateworlds-children 2023?gclid=Cj0KCQjw0bunBhD9ARIsAAZl0E3yPRax8gpNp HhJNraMhiIX3K1xY3YdHZDXnmdqVZ_aPGVB6_mC-waAkrVEALw_wcB
- Barros L, Barros L, do Carmo R, Santos M, da Costa Armstrong A, de Vasconcelos R, et al. Change in Rotavirus vaccine coverage in Brazil from before (2015-2019) Through the COVID-19 pandemic period (2020-2021). Viruses [Internet]. Available from. 2023; 15(2): 292. http://dx.doi.org/10.3390/v15020292.
