
Open Access, Volume 9
Laparoscopic treatment of adult diaphragmatic hernia after minimally invasive hepatectomy: A case report and literature review
Miroslava Kuzmova; Alexandre Goussens; Alexandra Dili; Claude Bertrand*
Unit of Digestive, Endocrine and General Surgery, Department of Surgery, Université Catholique de Louvain, CHU UCL Namur (Site Godinne), B-5530 Yvoir, Belgium.
Claude Bertrand
Unit of Digestive, Endocrine and General Surgery, Department of Surgery. Université Catholique de
Louvain, CHU UCL Namur (Site Godinne), B-5530 Yvoir, Belgium.
Tel: +32-81-423062;
Email: cl.bertrand@chuuclnamur.uclouvain.be & clbertrand@skynet.be
Received : Sep 16, 2023,
Accepted : Oct 25, 2023
Published : Oct 27, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: History of surgery is the second most common cause of acquired diaphragmatic hernia (DH) after trauma. Herein, we present a case of diaphragmatic hernia following minimally invasive laparoscopic liver surgery. We also reviewed the literature on adult DH after hepatectomy, the primary surgical cause.
Methods: Clinical case presentation and systematic literature review of adult DH after hepatectomy.
Results: A 71-year-old male patient was diagnosed a DH 42 months after a right extended laparoscopic hepatectomy for alveolar echinococcosis. A minimal invasive approach permitted a primary suture with intraperitoneal onlay mesh. There is no sign of recurrence at the 19-months follow-up.
The literature review reported only 80 cases. The incidence, type of liver surgery and indications, delay before DH diagnosis, clinical presentation, treatment, and recurrence rate were assessed. Based on this, an algorithm for work-up and treatment is proposed.
Conclusion: Although rare, diaphragmatic hernias should be considered in the differential diagnosis of abdominal and/or respiratory symptoms in patients with a history of liver surgery. Computed tomography imaging is the first-choice diagnostic modality, and surgical repair is key. The primary suture should be associated with mesh use. A long-term follow-up of at least two years was proposed to detect DH recurrence.
Keywords: Diaphragmatic hernia; Acquired pathology; Adult; Liver surgery; Hepatectomy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Bertrand C (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kuzmova M, Goussens A, Dili A, Bertrand C. Laparoscopic treatment of adult diaphragmatic hernia after minimally invasive hepatectomy: A case report and literature review. Open J Clin Med Case Rep. 2023; 2144.
Introduction
Diaphragmatic hernia (DH) is defined as the protrusion of abdominal content into the thoracic cavity through a defect in the diaphragm [1,2]. It is an uncommon pathology and its symptomatology varies from asymptomatic to life-threatening. DH can be classified into two groups: congenital and acquired. Congenital diaphragmatic hernia (CDH) is the most common type but is rare in adults. Acquired DH accounts for a large proportion of DH cases diagnosed in adults, mostly post-trauma, and more rarely iatrogenic, or in a few cases, spontaneous. Liver surgery, although rarely described, is an iatrogenic cause of DH. Herein, we report a case of DH after laparoscopic right hepatectomy, diagnostic workup, and management. A review of the literature focused on post-hepatectomy DH in adult patients.
Materials and methods
The clinical case of a patient with symptomatic diaphragmatic hernia after laparoscopic hepatectomy is described with the evaluation of the risk factors of this complication and the modalities of diagnosis and treatment. A literature review was performed by searching the PubMed and MEDLINE databases using the following keywords: “diaphragmatic hernia”, “acquired diaphragmatic hernia, “liver surgery, “hepatic surgery, and “hepatectomy”. Case reports and original series were selected. Overall, two Japanese-language and twenty-eight English-language publications published between 2002 and 2022 were considered. All the studies that contained materials relevant to this topic were reviewed.
Results
Case presentation: A 71-year-old male patient presented with intermittent postprandial epigastric pain. The dizconfort occurred 30 minutes after a meal and lasted from a few minutes to 2 hours. The symptoms were associated with dyspnea and a recent weight loss of 10 kg in the last 2 or 3 months.
His medical history included ischemic heart disease, arterial hypertension, auricular fibrillation, and sleep apnea syndrome. He presented with alveolar echinococcosis with a liver lesion 67×70 mm in diameter with central calcifications, hypermetabolic at PET tomography, heterogeneous aspect, cystic component, perilesional vascularization, and positive anti-Ecchinoccus antibodies (Figure 1). He was initially treated with 400 mg of albendazole twice daily and then underwent liver surgery. Extension of the lesions indicated a right hepatectomy extending to segment 4b using the laparoscopic approach. There was an important fibroinflammatory infiltration around the hepatic lesion, and extensive adhesiolysis was necessary to cleave the lesion from the diaphragm and remove some muscular fibers. However, no diaphragmatic damage was observed at the end of the surgery. Histology confirmed alveolar echinococcosis lesions in the resected liver invading the diaphragmatic muscle fibers.
In the context of intermittent epigastric pain, the patient was readmitted to the emergency department 42 months post-hepatectomy. The blood test results were normal. Right basal condensation and costophrenic angle blunting were observed on the chest radiography (Figure 2A). Thoracoabdominal computed tomography (CT) showed elevation of the right hemidiaphragm with DH of the colon, but no sign of bowel obstruction or colic ischemia (Figures 2B, 2C). Contrast radiography of the colon did not confirm herniation DH of the colon, only showing the elevation of the right half of the diaphragm with the colon that was located just below (Figure 2D). Therefore, except for the first CT scan, no other examination could highlight DH. For completeness, the patient also underwent gastroscopy and colonoscopy, both of which were normal.
The decision to proceed with surgical exploration was made because of the persistence of symptoms and the risk of strangulation. Different approaches were possible, including abdominal or thoracic surgery using open or mini-invasive surgery. We decided to proceed with a laparoscopic exploration. Numerous adhesions were observed between the greater omentum, residual liver, and diaphragm, requiring careful adhesiolysis. The ligamentum teres was left intact to avoid twisting of the liver, and the lateral slice of the liver and inferior vena cava were exposed. A 2–3 cm diameter defect near the vena cava in the right half of the diaphragm was confirmed. This symptomatic DH only contained the greater omentum but no bowel at the time of surgery. The defect was closed using non-resorbable stitches (Ticron 2/0®) and covered with a composite synthetic mesh (Parietex composite, 12 cm diameter) attached to the diaphragm with biological glue to avoid any recurrence (Figure 3).
No postoperative complications occurred and the patient was discharged on day 3. The patient was asymptomatic with no sign of recurrence or complication at 19 months follow-up, which will be pursued annually due to echinococcosis.
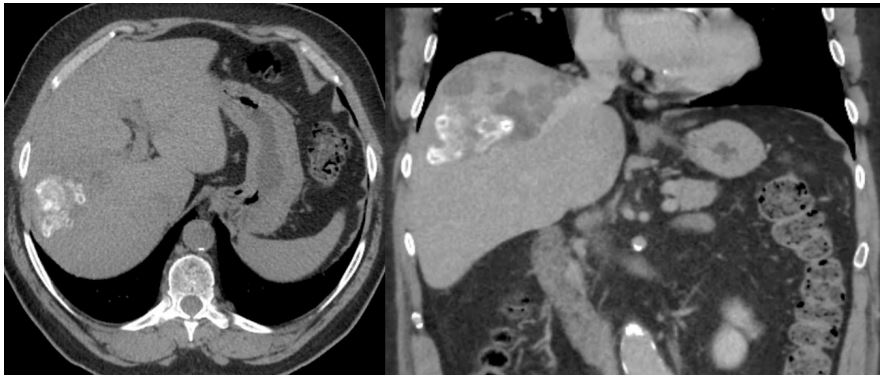
Figure 1: Initial liver lesion with central calcifications: alveolar echinococcosis.
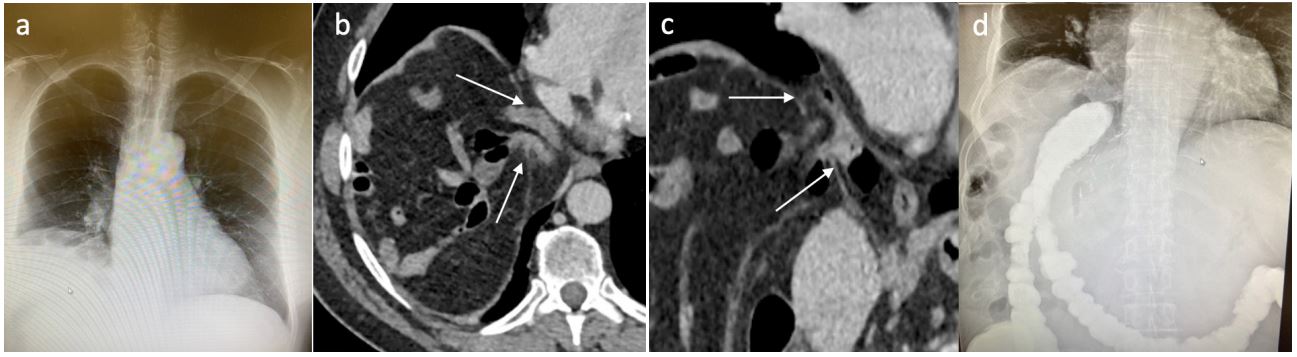
Figure 2: Diagnostic work-up of DH: a. chest X-ray: right diaphragm’s elevation; b-c: axial and coronal CT (arrows: defect’s
limits); d: colon X-ray.
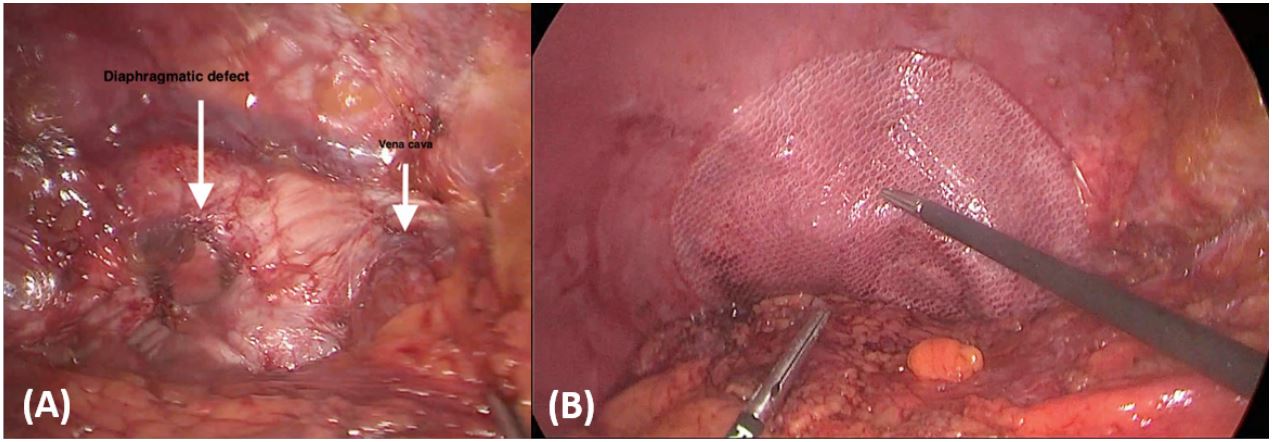
Figure 3: Per-operative view: A. diaphragmatic defect (long arrow) And vena cava (short arrow). B. direct suture covered
by a mesh.
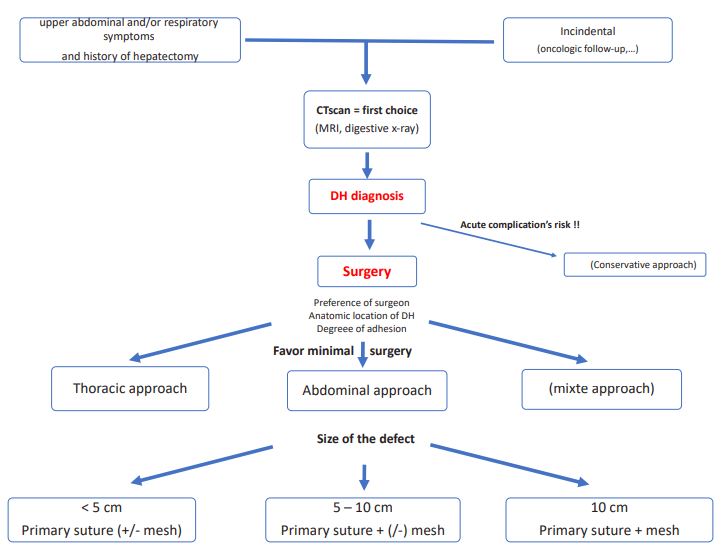
Figure 4: Algorithm for diaphragmatic hernia work-up and treatment.
Table 1: Summary of 81 cases of DH occurring after different type of liver surgery published in the literature. A: pre-operative parameters.
| Author | Year | Type of study | Cases n |
incidence % |
Indication for surgery |
Initial surgery |
Timing from initial surgery to DH (months) |
Symptoms | Author |
|---|---|---|---|---|---|---|---|---|---|
| Hemming [37] | 2002 | Case report | 1 | CRLM |
Ex-vivo resection/ reimplant segm 2+3 |
4 | Sepsis + death | Hemming [57] | |
| Sugita [38] | 2003 | Case report | 1 | FNH | LH | 8 | Abdo pain | Sugita [62] | |
| Hawxby [39] | 2006 | Case report | 1 | LDLT | RH | 36 | Abdo + respi | Hawxby [54] | |
| Matz [40] | 2009 | case report | 1 | CRLM | RH | 36 | Abdo pain | Matz [63] | |
| Perwaiz [41] | 2010 | Case report | 1 | LT recipient | Recipient of LT | 28 | Abdo pain | Perwaiz [64] | |
| Schellhaas [42] | 2010 | Case report | 1 | Hemangioma | RH | 48 | Respi | Schellhaas [65] | |
| Kousoulas [43] | 2010 | Retrospective study | 2 | 2.30 | LDLT | RH | N/A | N/A | Kousoulas [51] |
| LDLT | RH | N/A | N/A | ||||||
| Wagner [44] | 2010 | Case report | 1 | Recipient LT | LT | 48 | Abdo | Wagner [59] | |
| Dieter [45] | 2011 | Case report | 2 | LDLT | RH | 36 | Abdo + respiratory |
Dieter [66] | |
| LDLT | RH | 48 | Abdo + respiratory | ||||||
| Tabrizian [46] | 2012 | Case series | 10 | 1.01 | Tabrizian [47] | ||||
| Met RCC | RH | 5 | SBO | ||||||
|
Polycystic liver disease |
RH | 8 | SBO | ||||||
| LDLT | RH | 24 | Abdo pain | ||||||
| Ruptured adenoma | RH | 29 | Abdo pain | ||||||
| Met ovarian C | RH | 7 | Acute abdomen | ||||||
| HCC/HCV cirrh | RH | 13 | Asympto | ||||||
| HCC/HCV cirrh | RH | 17 | Asympto | ||||||
| Hemangioma | RH | 48 | Abdo pain | ||||||
| Met GIST |
LL, pancreacs, spleen |
20 | LBO | ||||||
|
Inflammatory adenoma |
Left lat resection | 10 | Abdo symptoms | ||||||
| Vernadakis [47] | 2012 | Case report | 1 | 0.61 | LDLT | RH | 30 | Abdo pain + SBO |
Vernadakis [52] |
| Soufi [48] | 2013 |
Case report / literature review |
1 | Bening liver cyst |
Laparoscopic fenestration |
12 | Abdo + respi | Soufi [67] | |
| Yonemura [49] | 2013 | Case report | 1 | Hemangioma | RH | 20 | Abdo | Yonemura [68] | |
| Lodhia [50] | 2014 | Case report | 1 | CRLM | LH | 8 | Asympto | Lodhia [69] | |
| Mizuno [51] | 2014 | Letter to the editors | 1 | LDLT | LH | 34 | Abdo pain | Mizuno [70] | |
| Jeng [52] | 2015 | Case report | 1 | 2.04 | LDLT | RH | 0.7 | Abdo pain | Jeng [43] |
| Livingstone [53] | 2016 |
Case report / literature review |
2 | LDLT | RH | 60 | Abdo symptoms Livingstone [58] | ||
| LDLT | RH | 19 | Abdo + respiratory + sepsis | ||||||
| Esposito [54] | 2017 |
Case series / literature review |
3 | 2.31 | HCC | RH | 31 | Abdo pain | Esposito [44] |
| HCC | RH | 16 | Asympto | ||||||
|
Mucinous cystadenoma |
RH | 4 | Asympto | ||||||
| Lochan [55] | 2017 | Case report | 1 | LDLT | RH | 12 | Abdo pain | Lochan [71] | |
| Oh [56] | 2017 | Retrospective study | 9 | 2.68 | 9 cases of LDLT | All RH | Median of 6 |
3 abdo symptoms/6 asympto |
Oh [45] |
| Takaichi [57] | 2018 | Case report | 1 | Trauma | RH | 3 | SBO | Takaichi [55] | |
| Manzini [58] | 2019 | Retrospective study | 5 | 0.83 | CCC | RH | 5 | SBO | Manzini [48] |
|
and literature review |
Echino | RH | 15 | Abdo pain | |||||
| Giant hemangioma | RH | 96 | LBO | ||||||
| IPN + Echino | RH | 22 | Mild symptoms | ||||||
| CRLM | RH | 27,5 | Asympto | ||||||
| Kawada [59] | 2020 | Case report | 1 | HCC | LH | 9 | Abdo pain | Kawada [72] | |
| Lee [60] | 2021 | Case report | 1 | HCC | RH | 12 | Chest pain | Lee [53] | |
| Raakow [61] | 2021 | Retrospective study | 5 | 0.17 | CRLM | RH | 21 | LBO | Raakow [46] |
| CCC | RH | 15 | Shortness of breath | ||||||
| CRLM | RH | 34 | Colon stenosis on colonoscopy | ||||||
| HCC | RH | 44 | Asympto | ||||||
| Cholecystitis | RH | 36 | Acute abdomen | ||||||
| Takagi [62] | 2021 | Case report | 1 | LDLT | LH | 4 | Abdo pain | Takagi [73] | |
| Martin [63] | 2021 |
Case series / literature review |
13 | 0.76 | 13 cases | Hepatic surgery | Median of 65,1 | Martin [49] | |
| 5 LDLT | 5 RH | 7 Abdo + respiratory | |||||||
| 5 Tumour | 5 RH | 6 Asympto | |||||||
| 1 Cyst | 1 LH | ||||||||
| 2 recipients LT | 2 recepient LT | ||||||||
| Watkins [64] | 2021 | Case report | 1 |
AdenoC oe + liver met |
Left lat excision + minimally invasive Ivor- Lewis |
48 |
Respi + renal failure |
Watkins [89] | |
| Kara [65] | 2022 | Retrospective study | 9 | 1.36 | Mean 47.33 | 7 abdo | Kara [70] | ||
| 5 LDLT | 5RH | ||||||||
| 1 recipient LT | 1 recipient LT | 2 respi | |||||||
| 3 echino | 3 RH | ||||||||
| Conde [66] | 2022 | Case report | 1 | HCC | RH | 24 | Abdo | Conde [90] | |
| Kuzmova | 2023 | present case report | 1 | Ecchinoc | RH | 42 | Abdo | Kuzmova | |
B: per- and post-op parameters.
| Author | no operation |
Surgical approach | Herniated organ |
Primary suture |
Mesh | DH diameter | F/U | Recurrence | Time to recurrence |
|---|---|---|---|---|---|---|---|---|---|
| repair | Months | (months) | |||||||
| Hemming [37] | 1 | Death | SB | N/A | Died | ||||
| Sugita [38] | Laparotomy | ST | Yes | No | N/A | N/A | N/A | ||
| Hawxby [39] | Thoracotomy | TC | Yes | No | N/A | Several | No | ||
| Matz [40] | Laparotomy | RC | Yes | No | N/A | N/A | N/A | ||
| Perwaiz [41] | Laparotomy | TC | Yes | No | 4cm | 7 | No | ||
| Schellhaas [42] | Laparotomy | SB+RC | Yes | No | N/A | N/A | N/A | ||
| Kousoulas [43] | N/A | N/A | Yes | N/A | N/A | N/A | N/A | ||
| N/A | N/A | Yes | N/A | N/A | N/A | N/A | |||
| Wagner [44] | Combined | Liver | Yes | Yes | 15x10cm | 0.5 | No | ||
| Dieter [45] | Thoracotomy | RC+TC+SB | Yes | Yes | 7cm | N/A | No | ||
| Thoracotomy | RC+SB | Yes | Yes | 7cm | N/A | No | |||
| Tabrizian [46] | Yes | no | Median of 36 | ||||||
| Laparotomy | SB | Yes | <5cm | No | |||||
| Laparotomy | SB | Yes | yes | >10cm | No | ||||
| Laparotomy | C | Yes | no | 5-10cm | No | ||||
| Laparotomy | N/A | Yes | yes | >10cm | No | ||||
| Laparotomy | SB | Yes | no | <5cm | No | ||||
| Laparotomy | N/A | Yes | no | <5cm | Yes | 10 | |||
| Laparotomy | C | Yes | no | <5cm | No | ||||
| Laparotomy | SB+C+Kidney | Yes | yes | >10cm | No | ||||
| Laparotomy | C | Yes | no | <5cm | No | ||||
| Laparoscopy | ST | Yes | no | <5cm | No | ||||
| Vernadakis [47] |
Laparotomy | SB+Om | Yes | No | 4-5cm | 23 | No | ||
| Soufi [48] | Laparotomy | C+Om | Yes | No | 10cm | N/A | N/A | ||
| Yonemura [49] | Laparoscopy | TC+Om | yes | N/A | N/A | N/A | N/A | ||
| Lodhia [50] | Thoracotomy | Om | Yes | No | 0.5 | N/A | N/A | ||
| Mizuno [51] | Laparotomy | ST | Yes | No | 4x3cm | 21 | No | ||
| Jeng [52] | Laparotomy | SB | Yes | No | 4x4cm | 18 | No | ||
| Livingstone [53] |
Laparotomy | RC | Yes | No | N/A | N/A | N/A | ||
| Laparotomy | SB+TC | Yes | No | N/A | N/A | N/A | |||
| Esposito [54] | Laparotomy | C | Yes | No | 3cm | 10 | No | ||
| Laparotomy | C | Yes | No | 9cm | 1 | No | |||
| Laparotomy | SB+C | Yes | Yes | 3.5cm | 5 | No | |||
| Lochan [55] | Laparotomy | SB+C | Yes | No | N/A | 12 | No | ||
| Oh [56] | 6 | 3 N/A | N/A | N/A | N/A | mean 2.8cm | N/A | N/A | |
| Takaichi [57] | Laparoscopy | SB | Yes | No | 5.3cm | 6 | No | ||
| Manzini [58] | Laparotomy | SB | Yes | No | 2.2x2.5cm | 36 | No | ||
| Laparotomy | SB | Yes | No | 5.4x5.5cm | 8 | No | |||
| Laparotomy | C | Yes | No | 3.5x 3.3cm | N/A | N/A | |||
| 1 | Refused | C | 3.5x3.9cm | ||||||
| 1 | Refused | Om | 4x4cm | ||||||
| Kawada [59] | Laparoscopy | ST | Yes | No | N/A | N/A | N/A | N/A | |
| Lee [60] | 1 | Death | SB | N/A | |||||
| Raakow [61] | Laparotomy | RC+Om | Yes | no | 4cm | 12 | Yes | 12 | |
| Laparotomy | RC+Om | Yes | yes | <5cm | 12 | Yes | 12 | ||
| laparoscopy | C+Om | Yes | yes | 4cm | 52 | No | |||
| Laparotomy | C | Yes | No | 5cm | 14 | No | |||
| Laparotomy | SB+C | Yes | No | 7cm | 22 | Yes | 22 | ||
| Takagi [62] | Thoracoscopy | ST | Yes | No | 3cm | 20 | No | ||
| Martin [63] | Mean 6cm | mediane of 35.5 | |||||||
| 12 Laparotomy | 5C | Yes | 2/13 mesh |
1 Yes | 4.5 | ||||
| 1 Thoracotomy | 4C+SB | Yes | |||||||
| 2SB | Yes | ||||||||
| 2liver | Yes | ||||||||
| 2Om | Yes | ||||||||
| 1C+ST+Spleen | Yes | ||||||||
| Watkins [64] | Combined | TC | Yes | No | 3cm | 12 | No | ||
| Kara [65] | 8 N/A | N/A | 8 Yes | 8 No | N/A | N/A | N/A | ||
| N/A | |||||||||
| 1 | Death | N/A | |||||||
| Conde [66] |
Discharge pending surgery |
SB+RC+pancreas | N/A | N/A | N/A | ||||
| Kuzmova | Laparoscopy | C+Om | yes | yes | 3cm | 12 | No | ||
Literature Review
Congenital DH, due to a defect in the fusion of different parts of the diaphragm, ranges from 0.8 to 5 per 10,000 births [1,3,4]. CDH diagnosis in adults is rare, representing 0.17 to 6% of these cases [5]. Acquired DH is primarly caused by trauma, blunt trauma, or penetrating trauma. Diaphragmatic injury occurs in 0.1% of blunt thoracic trauma, 10-15% of cases of penetrating trauma to the lower chest and 3-5% of cases of blunt trauma to the abdomen [6]. It represents less than 1% of all trauma patients [7,8]. Traumatic DH is usually located on the left side because of the presence of the liver on the right side, which covers the diaphragm and protects it from injury. Surgery is the second most common cause of acquired DH is surgery [1]. DH has been described after different types of surgery, including left colectomy [9], Ad- DH has been described after different types of surgery, including left colectomy [9], Adrenalectomy [10], spleno-distal pancreatectomy [11], gastrectomy [12], nephrectomy [13-16], debulking surgery [17,18], coronary artery bypass graft with the right gastroepiploic artery [19], pericardial window fenestration, and lung surgery [20,21]. However, most postsurgical DH cases have been described after hepatectomy and radiofrequency ablation [22-24]. DH can also appear spontaneously [25, 26, 27], after an effort [28], during pregnancy [29], or in the catamenial period [30] and may be due to endometriosis [31- 34] or retroperitoneal hydatidosis [35].
This review focuses on adult DHs after hepatectomy, which could become an important issue. Indeed, as described after laparoscopic esophagectomy for hiatal and para-hiatal hernia [36], the incidence of acquired DH could increase in the near future owing to less adhesion formation associated with minimally invasive surgery. Considering that ADH is linked to liver surgery, 30 papers [37-66] were selected, allowing the identification of mostly case reports and only six papers with a series of at least five cases. The incidence, type of liver surgery, indications, and delay in DH diagnosis, clinical presentation, treatment, and recurrence were assessed (Table 1). It summarizes 80 other cases of DH occurring after different types of liver surgery.
The incidence of ADH after liver surgery has been evaluated in 10 reports [43,46,47,52,54,56,58,6 1,63,65], with a global incidence of 0,75%. The incidence was 2.5% for living donor surgery, varying from 0.61% to 9.6%, and 0,4% after resection for hepatic tumors, varying from 0 to 2.31. The most important serie [61] evidenced a low incidence (0.17% (5/3017] ), all after right liver hepatectomies with an incidence of 0.7% in this group (5/714). Tabrizian, in a series of 993 patients, described an incidence of 1.9% after right hepatectomy and 0.,4% after left hepatectomy [46]. The impact of right-sided hepatectomy was also evident in this review with of 65/81 cases (80%). The other cases included seven left hepatectomies (8.6%), five liver transplant recipients (6.2%), three cases of complex surgery (3.7%), and one laparoscopic biliary cyst fenestration (1.2%) among the 81 cases.
There is no information on the use of a minimally invasive approach for liver surgery or its potential influence on the rate of DH. Except for the case reported here, only one other case has been documented after a laparoscopic approach for fenestration of biliary cyst [48]. Indeed, minimally invasive hepatectomy induces fewer adhesions, which could be the origin of more frequent ADH, as described after minimally invasive oesophagectomy [36]. However, no evidence supports this hypothesis.
Considering the indication for liver surgery prior to ADH, LDLT was the most common indication (32 cases, 39.5%), followed by malignant disease (25 cases, 30.9%). This could be attributed to the fact that these populations benefit from regular follow-up. The third most common indication for hepatic surgery was resection of benign hepatic tumors (11 cases; 13.6%), followed by liver transplant recipients (5 cases; 6.2%) and infectious diseases (6 cases; 7,4%). Diaphragmatic invasion, malignancy, infection, and largevolume lesions could be associated with a risk of postoperative DH [46]. This was the case in our patient, as alveolar echinococcosis is an infiltrative parasitic pathology. Indeed, during surgical mobilization of the liver, small cautery-related thermal injuries can weaken the diaphragm, and these lesions may remain unnoticed [54]. There is possibility to test intraoperatively the integrity of the diaphragm by a «bubble test» which consists in positioning the patient in Trendelenburg position, filling the upper quadrant with saline and asking the anesthesiologist for a Valsalva. The presence of air bubbles indicates diaphragmatic defect [18]. Because of the strong contractile force of the diaphragm, these microlesions may increase over time, leading to a transmural diaphragmatic defects and DH [58]. Poor nutritional status, postoperative ascites, and other causes of high intra-abdominal pressure can increase the risk of DH [39,46,60]. Nevertheless, its etiology appears to be multifactorial [25, 31, 32]. To avoid the possible development of DH, the smallest defect should be closed [14].
According to our review, the delay in DH occurrence ranges from 20 days to 244.7 months with a mean of 31.68 months.
Regarding symptomatology, the literature review revealed that 21/81 (25.9%) patients may be asymptomatic or present with mild discomfort. Abdominal (39/81 (48.1%)), respiratory (6/81 (7.4%)), and associated complaints (12/81 (14.8%)) were reported. Acute symptoms of bowel obstruction, bowel perforation with sepsis or respiratory distress, and even post-mortem diagnoses have been documented. Indeed, two patients developed sepsis [37, 53], and in three cases, DH even led to death [37, 60, 65]. This finding underlines the importance of detecting this rare complication of hepatic surgery.
Different organs pass through the diaphragm to the thoracic cavity. The most frequently herniated organ was the colon (38/81 cases, 46.9%), followed by the small bowel (25/81 cases, 30.9%) and stomach (6/81 cases, 7.4%). DH could contain the liver (3 cases) [44,54], kidney (1 case) [46], Pancreas (1 case) [66], spleen (1 case) [63], and omentum without any other organ in 4/81 cases (4.9%).
In general, five radiological methods can be used to identify DH: chest radiography, barium study, US, CT, and magnetic resonance imaging (MRI). However, every imaging method can be falsely reassuring if the DH is intermittent, as in our case. Radiography and contrast may also be helpful in this regard. Some authors suggest that radiological screening with conventional chest radiography after right hepatectomy can improve the early diagnosis of DH; however, conventional chest radiography has shown only limited sensitivity for the detection of diaphragmatic defects [2,61,67]. Contrast radiography can reveal dilated segments of the intestinal tract, the proximal site of obstruction, and the eventual presence of abdominal contents in the thoracic cavity [2]. US can evaluate the integrity of the diaphragm, herniated organ, and the use of Doppler signals to analyze the vascularization of herniated organs, but it is user-dependent [2,61]. CT scan is the most effective because of its short duration and relatively easy access. Moreover, CT scans are included in the follow-up of most cancers and are often used in emergencies. It allows simultaneous investigation of the abdominal and thoracic cavities, differentiation of DH from diaphragmatic relaxation, and detection of the type of herniated organ with potential complications [2,58,61] MRI is not the first-choice imaging, but it can be an alternative because of its sensitivity to soft tissue. MRI can clearly show a normal diaphragm as a continuous linear structure, and discontinuity appears in the case of hernial defects [2].
A diagnosis of DH should be made promptly because of the risk of complications and the necessity for surgical repair. Surgery is indicated even for asymptomatic patients, except for those with too many morbidities, for whom the benefits of surgery are lower than the risks. Of the 81 patients, 12 did not undergo any surgery. Three patients died before an eventual surgery [60,65], 2 refused surgery [58], and 1 patient was discharged with pending surgery [65]. In one study, only symptomatic patients (3/9) benefited from the surgery. The other 6 patients did not receive any surgical intervention as they remained asymptomatic [56].
Regarding the treatment, different approaches exist: thoracic or abdominal approach, open or mini-invasive surgery, depending on the preference of the surgeon, surgical history of the patient, anatomic location of the defect, and degree of infra-diaphragmatic adhesions. A thoracic approach might be easier to use to treat recurrent diaphragmatic hernia, mostly following previous abdominal repair, because of numerous adhesions due to previous surgeries [54]. In our literature review, among 69 operated patients laparotomy was performed in 42 (60.9%) patients, thoracotomy in 5 (7.2%), laparoscopy in 6 (8.7%), thoracoscopy in 2 (2.9%), and combined thoracic and abdominal approach in 2 (2.9%). The type of approach was not specified in 13 patients. The most common setting for DH is an emergency situation; therefore, the open approach is usually performed, even though the laparoscopic approach is superior with regard to convalescence, especially with regard to postoperative pain and mobilization [61].
Different repair techniques exist: primary suture without mesh and primary suture reinforced with mesh. Primary suture repair was performed in all 65 operated patients with a known type of repair; however, in only 12 cases (18.5%), a mesh was used. The clear criteria for the use of mesh are not currently determined, and the choice of the approach depends on several factors mentioned above [54]. Tabriziani, et al. described primary closure of the diaphragmatic defect using non-absorbable sutures via an abdominal approach for patients with small-sized (<5 cm) and moderate-sized (5-10 cm) hernias [46]. The use of a mesh is also recommended by other authors for larger diaphragmatic defects (>10 cm) [46,57,58]. On the other hand, Raakow, et al. recommended the systematic use of meshes associated with sutures. Indeed, in their study, 80% of recurrences occurred without the use of a mesh [61]. In this review, the diameter was known for 58 cases. Most patients were diagnosed with DH with a defect equal to or smaller than 5 cm (32;55.2%), compared to defects between 5 and 10 cm (21;36.2%) and larger than 10 cm (5;8.6%).
Recurrence was documented in only five cases: two with small defects (<5 cm) and no mesh, one with a small defect and mesh; one with a large defect (7 cm) without mesh, and one unspecified. There are no guidelines regarding the frequency and length of follow-up in patients with DH. Patients with a history of oncological disease or liver transplantation will continue their usual follow-up. Every patient who benefits from surgical repair of DH should be followed up regularly to detect an eventual recurrence of DH before developing any complications. There is insufficient data in the literature concerning the recurrence rate and timing after surgery. The longest reported follow-up was similar in the two largest series: Martin’s series with a median follow-up of 35.5 months (from 1 to 173.1 [63]), and Tabrizian’s series with a median follow-up of 36 months (from 10 to 167 [46]). Only two other patients had a follow-up period of >3 years : one patient in Raakow’s retrospective study (52months) [61] and one in Manzini’s retrospective study (36 months) [58]. Globally, among the five documented cases of recurrence, all were detected in less than 22 months after DH repair [46,61,63]. The median delay in recurrence was 12 months. Considering the timing of the documented DH recurences, two-years follow-up should be recommended. Based on this review, we propose an algorithm for DH workup and treatment (Figure 4).
Conclusion
In summary, although iatrogenic diaphragmatic hernia is rare, the incidence of DH could increase in the near future owing to fewer adhesions linked to minimally invasive surgical approaches; however, there is no evidence in the literature. Diaphragmatic hernia can have fatal consequences, due to the incarceration of abdominal organs. Its clinical presentation varies, with mild symptoms and fatal complications linked to incarceration of abdominal organs. Therefore, it is important to include DH in the differential diagnosis of right upper abdominal and/or respiratory symptoms in all patients with a history of previous liver resection. The major risk factors are right-sided hepatectomy for large-volume lesions, and invasion or adhesion to the diaphragm. Computed tomography (CT) is the first-choice diagnostic modality followed by radiography.
Once DH is diagnosed, it should be repaired surgically, probably even in asymptomatic patients, owing to the risk of complications. Different approaches can be chosen according to the patient’s surgical history, DH characteristics, and surgeon expertise. Abdominal DH repair without mesh represents the most commonly used technique reported in the literature; however, the use of a non-resorbable mesh should certainly be recommended for large DH, even systematically. A 2 years follow-up seems sufficient to detect most DH recurrences.
Declarations
Statement of ethics: The patient gave informed consent.
Conflict of interest statement: No conflict of interest.
Author contributions: First and last authors: clinical care, data acquisition and analysis, paper drafting; second author: clinical care and paper drafting; third author: paper drafting and revision.
References
- Spellar K, Lotfollahzadeh S, Gupta N. Diaphragmatic Hernia. StatPearls Publishing. 2023 Jan. 2022.
- Eren S, Ciris F. Diaphragmatic hernia diagnostic approaches with review of the literature. European Journal of Radiology 2005; (54): 448-459.
- Skari H, Bjornland K, Haugen T, Emblem R. Congenital diaphragmatic hernia: a meta-analysis of mortality factors. J Pediatr Surg. 2000; 35: 1187-97.
- Sadler TW. Medizinische Embryologie. 10th ed. Stuttgart: Thieme. 2003.
- Testini M, Girardi A, Isernia RM, De Palma A, Catalano G, Pezzolla A, et al. Emergency surgery due to diaphragmatic hernia: case series and review. World J Emerg Surg. 2017; 12:23.
- Nishijima D, Zehbtachi S, Austin RB. Acute posttraumatic tension gastrothorax mimicking acute tension pneumothorax. American Journal of Emergency Medicine. 2007; 25: 734-736.
- Simon LV, Lopez RA, Burna B. Diaphragmatic rupture Statpearls. 2022.
- Bocchini G, Guida F, Sica G, Codella U, Scaglione M. Diaphragmatic injuries after blunt trauma: are tey still a challenge? Reviewing CT findings and integrated imaging. Emerg Radiol. 2012; 19(3): 225-35.
- Dell’Abate P, Bertocchi E, Dalla Valle R, Viani L, Del Rio P, Sianesi M. Iatrogenic diaphragmatic hernia following laparoscopic left colectomy for splenic flexure cancer An unusual complication. Ann Ital Chir. 2016; 87.
- Vilallonga R, Caubet E, González O, Neff KJ, Fort JM, Mazarro A, Armengol M. Laparoscopic repair of a postadrenalectomy leftsided diaphragmatic hernia complicated by chronic colon obstruction. Surg Endosc. 2013 May;27(5):1826-8.
- Pansini G, Pascale G, Pigato I, Malvicini E, Andreotti D, Caruso A, Stano R, Occhionorelli S. A rare diaphragmatic hernia with a delayed presentation of intestinal symptoms following spleno-distal pancreatectomy: a case report. J Surg Case Rep. 2017; (7): 135.
- Suh Y, Lee JH, Jeon H, Kim D, Kim W. Late onset iatrogenic diaphragmatic hernia after laparoscopy-assisted total gastrectomy for gastric cancer. J Gastric Cancer. 2012; 12(1): 49-52.
- Mínguez Ruiz G, García Florez LJ, Arias Pacheco RD, García Bear I, Ramos Pérez V, Pire Abaitua G. Post-nephrectomy diaphragmatic hernia. Increase suspicion and decrease morbi-mortality: two cases report. J Surg Case Rep. 2018; 2018(8): 224.
- Frohme C, Walthers EM, Schrader AJ, Olbert P, Hofmann R, Hegele A. Intrathoracic hernia after laparoscopic nephrectomy: clinical manifestation and conservative management. Urologe A. 2009; 48(12): 1499-502.
- Saujani S, Rahman S, Fox B. Budd-Chiari syndrome due to right hepatic lobe herniation: CT image findings of two rare clinical conditions. BJR Case Rep. 2017; 3(3): 20160133.
- Azam A, Michael K. Postnephrectomy diaphragmatic hernia presenting as progressive dyspnoea. BMJ Case Rep. 2020; 13(10): 235881.
- Mestre A, Ferreira Simões A, Marino F, Gonçalves Pereira J. Passing Through a Hole: Delayed Diaphragmatic Hernia After Cytoreductive Surgery. Cureus. 2021; 13(12): 20314. doi: 10.7759/cureus.20314. eCollection 2021.
- Ehmann S, Aviki EM, Sonoda Y, Boerner T, Sassine D, Jones DR, et al. Diaphragm hernia after debulking surgery in patients with ovarian cancer. Gynecol Oncol Rep. 2021; 36: 100759.
- Ikeda Y, Tobari S, Morita N, Okinaga K. Strangulated intrapericardial herniation of the stomach after use of the right gastroepiploic artery for coronary artery bypass grafting. Interact Cardiovasc Thorac Surg. 2005; 4(3): 168-9.
- Sultan A, Usman A, Akhtar S, Rehman A, Siddiqui K. Diaphragmatic Hernia Presenting as Acute Gastric Outlet Obstruction: A Rare Complication of Left Lower Lobectomy. Cureus. 2022; 14(7): 26544.
- Fukami T, Konoeda C, Kitano K, Sakamoto M, Sano A, Yoshida Y, Mura T, Nakajima J. [Iatrogenic diaphragmatic hernia following partial resection of the lung via video-assisted thoracoscopy]. Kyobu Geka. 2010; 63(13): 1151-4.
- Nomura R, Tokumura H, Furihata M. Laparoscopic repair of a diaphragmatic hernia associated with radiofrequency ablation for hepatocellular carcinoma: lessons from a case and the review of the literature. Int Surg. 2014 Jul-Aug;99(4):384-90.
- Saito T, Chiba T, Ogasawara S, Inoue M, Wakamatsu T, Motoyama T, et al. Fatal Diaphragmatic Hernia following Radiofrequency Ablation for Hepatocellular Carcinoma: A Case Report and Literature Review. Case Rep Oncol. 2015; 8(2): 238-45.
- Morito A, Nakagawa S, Imai K, Uemura N, Okabe H, Hayashi H, et al. Successful surgical rescue of delayed onset diaphragmatic hernia following radiofrequency ablation using a thoracoscopic approach for hepatocellular carcinoma: a case report. Surg Case Rep. 2021; 7(1): 130.
- Spiridakis KG, Flamourakis ME, Gkionis IG, Kaloeidi EI, Fachouridi AI, Konstantoulaki SE, et al. Right-sided strangulating diaphragmatic hernia in an adult without history of trauma: a case report. J Med Case Rep. 2021; 15(1): 372.
- Di Mari A, Failla G, Farina R, Conti A, Foti P, Pennisi I, et al. Non traumatic intrathoracic liver herniation mimicking a pulmonary metastasis in patient with breast cancer: A case report. Radiol Case Rep. 2021; 16(11): 3426-3430.
- Gunia DM, Porter DJ, Alijani A, Patil P. A tale of two unconventional adult diaphragmatic hernias. Ann R Coll Surg Engl. 2022.
- Abd Elrazek AE, Shehab A, Elnour AA, Al Nuaimi SK, Baghdady S. Colon in the chest: an incidental dextrocardia: a case report study. Medicine (Baltimore). 2015; 94(6): 507.
- Jacobs R, Honore PM, Hosseinpour N, Nieboer K, Spapen HD. Sudden cardiac arrest during pregnancy: a rare complication of acquired maternal diaphragmatic hernia. Acta Clin Belg. 2012; 67(3): 198-200.
- Sanna S, Taurchini M, Monteverde M, Agnoletti V, Casoni GL. Catamenially recurring pneumothorax with partial liver herniation: a particular view. Respiration. 2011; 82(5): 476-7.
- Triponez F, Alifano M, Bobbio A, Regnard JF. Endometriosis-related spontaneous diaphragmatic rupture. Interact Cardiovasc Thorac Surg. 2010; 11(4): 485-7.
- Gaichies L, Blouet M, Comoz F, Foulon A, Heyndrickx M, Fauvet R. Non-traumatic diaphragmatic rupture with liver herniation due to endometriosis: A rare evolution of the disease requiring multidisciplinary management. J Gynecol Obstet Hum Reprod. 2019; 48(9): 785-788.
- Singh TP, Rizvi SAA, Pretorius CF. Post-menopausal acquired diaphragmatic herniation in the context of endometriosis. Int J Surg Case Rep. 2018; 53: 154-156.
- Yu PS, Sihoe AD. Beware the ‘raised right hemidiaphragm’ in a female patient with previous pneumothorax surgery: liver herniation through a massive endometrosis-related diaphragmatic fenestration. J Thorac Dis. 2015; 7(5): 112-6.
- Boumarah D, Alsinan A, Alothman O, AlDandan O, Alshomimi S. Acquired right-sided diaphragmatic hernia in a patient with retroperitoneal hydatidosis: a case report and review of the literature. J Med Case Rep. 2021; 15(1): 320.
- Oor JE, MD, Wiezer MJ, Hazebroek EJ. Hiatal Hernia After Open versus Minimally Invasive Esophagectomy: A Systematic Review and Meta-analysis. Ann Surg Oncol DOI 10.1245/s10434-016-5155-x.
- Hemming AW, Reed AI, Langham MR, Fujita S, van der Werf WJ, Howard RJ. Hepatic vein reconstruction for resection of hepatic tumors. Ann Surg. 2002; 235(6): 850-8.
- Sugita M, Nagahori K, Kudo T, YamanakaK, Obi Y, Shizawa R, et al. Diaphragmatic hernia resulting from injury during microwave-assisted laparoscopic hepatectomy. Surg Endosc (2003) 17: 1849–1852.
- Hawxby AM, Mason DP, Klein AS. Diaphragmatic hernia after right donor and hepatectomy: a rare donor complication of partial hepatectomy for transplantation. Hepatobiliary Pancreat Dis Int 5(3):459–461 (2006)
- Matz D, Kirchhoff P, Kocher TM, Heizmann O. Consecutive cecum perforation due to incarcerated diaphragmatic hernia after liver surgery. Int. J. Color. Dis. 2009; [24]; 1353-1354.
- Perwaiz A, Mehta N, Mohanka R, Kumaran V, Nundy S, Soin A-S. Right-sided diaphragmatic hernia in an adult after living donor liver transplant: a rare cause of post-transplant recurrent abdominal pain. Hernia 2010; 14: 547-549.
- Schellhaas E, Dobler O, Kroesen AJ, Buhr H-J, Hotz HG. Gangrenous Intrathoracic Appendicitis, a Rare Cause of Right-Sided Chest Pain: Report of a Case. Surg Today. 2010; 40: 874-877.
- Kousoulas L, Becker T, Richter N, Emmanouilidis N, Schrem H, Barg-Hock H. Living donor liver transplantation: effect of the type of liver graft donation on donor mortality and morbidity. Transpl Int. 2011; 24(3): 251-8.
- Wagner D, Iberer F, Sereinigg M, Kniepeiss D, Kornprat P, Fahrleitner-Pammer A, et al. Massive diaphragmatic herniation following orthotopic liver transplantation in an adult. Liver Transpl. 2010; 16(6): 783-5.
- Dieter RA, Spitz J, Kuzycz G. Incarcerated Diaphragmatic Hernia with Intrathoracic Bowel Obstruction After Right Liver Donation. Int. Surg. 2011; 96: 239-244.
- Tabrizian P, Jibara G, Shrager B, Elsabbagh AM, Roayaie S, Schwartz ME. Diaphragmatic hernia after hepatic resection: case series at a single Western institution. J Gastrointest Surg. 2012; [16]: 1910-1914.
- Vernadakis S, Paul A, Kykalos S, Fouzas I, Kaiser G, Sotiropoulos G. Incarcerated Diaphragmatic Hernia After Right Hepatectomy for Living Donor Liver Transplantation: Case Report of an Extremely Rare Late Donor Complication. Transplant. Proc. 2012; [44]: 2770-2772.
- Soufi M, Meillat H, Le Treut YP. Right diaphragmatic iatrogenic hernia after laparoscopic fenestration of a liver cyst: report of a case and review of the literature. World J Emerg Surg. 2013; 8(1): 2.
- Yonemura Y, Umeda K, Kumashiro R, Mashino K, Ogawa T, Adachi E, et al. Laparoscopic repair of incarcerated diaphragmatic hernia as a late complication of laparoscopic right hepatectomy: a case report. Fukuoka Igaku Zasshi. 2013; 104(12): 599-602.
- Lodhia JV, Appiah S, Tcherveniakov P, Krysiak P. Diaphragmatic hernia masquerading as a pulmonary metastasis. Ann R Coll Surg Engl. 2015; 97: 27-29.
- Mizuno S, Tanemura A, Isaji S. Incarcerated left diaphrag- matic hernia following left hepatectomy for living donor liver transplantation. Transpl Int 2014; 27(7): 65-67.
- Jeng, KS, Huang, CC, Lin CK, Lin CC, Wu JM, Chen KH, Chu SH. Early Incarcerated Diaphragmatic Hernia Following Right Donor Hepatectomy: A Case Report. Transplant. Proc. 2015; 47: 815-816.
- Livingstone SM, Andres A, Shapiro A.J, Kneteman, NN, Bigam, DL. Diaphragmatic Hernia After Living Donor Right Hepatectomy: Proposal for a Screening Protocol. Transplant. Direct 2016; 2: 84.
- Esposito F, Lim Ch, Salloum Ch, Osseis M, Lahat E, Compagnon Ph, Azoulay D. Diaphragmatic hernia following liver resection: case series and review of the literature. Ann Hepatobiliary Pancreat Surg. 2017; 21(3): 114-121.
- Lochan R, Saif R, Ganjoo N, Sakpal M, Panackal Ch, Raja K, et al. Diaphragmatic herniation following donor hepatectomy for living donor liver transplantation: a serious complication not given due recognition. Ann Hepatobiliary Pancreat Surg 2017; 21: 232-236.
- Oh JW, Oh SN, Jung SE, Byun JY. Diaphragmatic Hernia After Living-Donor Right Hepatectomy: An Important Late Donor Complication. J Comput Assist Tomogr.2017; 41(5): 726-730.
- Takaichi S, Takahashi T, Funaki S, Tanaka K, Miyazaki Y, Makino T, et al. Laparoscopic repair of an incarcerated diaphragmatic hernia after right hepatectomy for hepatic injury: a case report. Surg Case Rep. 2018; 4(1): 135.
- Manzini G, Kuemmerli C, Reiner CS, Petrowsky H, Gutschow CA. Enterothorax After Hepatic Surgery: A Single-Center Experience. World J Surg. 2019; 43(3): 902-909.
- Kawada J, Hata T, Murotani M, Nagano S, Shigetsu K, Imamura H,, et al. Laparoscopic Repair of Incarcerated Diaphragmatic Hernia as a Complication of Left Hepatectomy for Liver Cancer Gan To Kagaku Ryoho. 2020; 47(11): 1630-1632.
- Lee SW, Lee SD, Kim M-Y. Incarcerated diaphragmatic hernia after right hepatectomy: an autopsy case with a review of 45 previous cases. Int J Legal Med. 2021; 135(4): 1549-1554.
- Raakow J, Biebl M, Megas I-F, Schmelzle M, Schoening W, Lurje G,, et al. Incidence, Diagnosis and Repair of a Diaphragmatic Hernia Following Hepatic Surgery: A Single Center Analysis of 3107 Consecutive Liver Resections. J Clin Med. 202; 10(5): 1011.
- Takagi K, Kuise T, Yoshida K, Yoshida R, Umeda Y, Fujiwara T, Yagi T. Adult Bochdalek hernia following living donor left hepatectomy repaired by thoracoscopy-assisted surgery: A case report. Asian J Endosc Surg. 2022; 15: 220-224.
- Martin V, Gregoire E, Chopinet S, Scatton O, Dubois R, Lasseur A,, et al. Acquired diaphragmatic hernia after hepatectomy and liver transplantation in adults and children: A case series and literature review Ann Hepatobiliary Pancreat Surg. 2021; 25: 462-471.
- Watkins AA, Kalluri A, Gupta A, Gangadharan SP. Iatrogenic diaphragmatic hernia with fecopneumothorax following minimally invasive esophagectomy and liver resection. JTCVS Tech. 2021; 11: 89-91.
- Kara S, Korkut E, Aksungur N, Altundas N, Ozturk G. Development of diaphragmatic hernia following hepatectomy. ANZ J Surg. 2022; 92(9): 2163-2166.
- Conde Inarejos B, Valero Liñán AS, González Masiá JA, Miota de Llama JI. Right diaphragmatic hernia after major hepatectomy. Cir Esp (Engl Ed). 2022; (22): 2173-5077. 00151-X.
- Garne E, Haeusler M, Barisic I, Gjergja R, Stoll C, Clementi M. Congenital diaphragmatic hernia: evaluation of prenatal diagnosis in 20 European regions. Ultrasound Obstet Gynecol. 2002; 19(4): 329–333.
