
Open Access, Volume 9
A medical and literature undescribed case of acute abdomen - Consequences of bilateral torsion of the adnexa: Case report
Milos Milincic1 ; Stefan Dugalic1,2; Jovana Todorovic3; Aleksandar Dmitrovic1,2; Dusica Kocijancic1,2; Mirjana Jovandaric4; Miroslava Gojnic1,2
1Division of Gynecology and Obstetrics, University Clinical Centre of Serbia, Belgrade, Serbia.
2Faculty of Medicine, University of Belgrade, Belgrade, Serbia.
3University of Belgrade, Faculty of Medicine, Institute of Social Medicine, Belgrade, Serbia.
4Division of Neonatology, Clinic of Gynecology and Obstetrics, University Clinical Centre of Serbia, Belgrade, Serbia.
Miloš Milinčić
Faculty of Medicine, University of Belgrade, Belgrade, Serbia.
Tel: +381658720461;
Email: milosmilincic@gmail.com
Received : Sep 11, 2023,
Accepted : Oct 18, 2023
Published : Oct 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Torsion is the turning of the adnexa around its axis. It accounts for 3% of all gynecological emergencies. It also happens during pregnancy, as much as 20-25% of all torsions. It most often occurs in pathologically altered ovaries, 60-80% of cases. Causes in pregnancy are more often benign than in nonpregnant women. The diagnosis is established by clinical picture, physical and ultrasound examination. Due to the specificity of pregnancy, it is more difficult to diagnose, especially in the third trimester. Torsion is treated surgically by laparoscopy or laparotomy. Options are detorquation or removal of the necrotic adnexa.
Case report: We report the first case of bilateral adnexal torsion in the third trimester of pregnancy. A 32-year-old pregnant woman came to our institution in the 28th week of a spontaneous twin pregnancy with pain in the right hemiabdomen and an episode of vomiting. After clinical, laboratory and ultrasound evaluation, as well as artificial maturation of fetal lungs, cesarean section and bilateral adnexectomy were successfully performed. Pathohistological findings showed infarction and necrosis of the adnexa.
Conclusion: Torsion of the adnexa is not uncommon in pregnancy, with 20-25% of all torsions occurring in pregnant women. Torsion of the adnexa should be considered in the differential diagnosis of pain in pregnancy, especially if it is accompanied by nausea, vomiting and fever.
Keywords: Ovarian torsion; Bilateral torsion of the adnexa; Torsion of the adnexa in pregnancy; Pregnancy; Cesarean section.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Milinčić M (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Milincic M, Dugalic S, Todorovic J, Dmitrovic A, Kocijancic D, et al. A medical and literature undescribed case of acute abdomen - Consequences of bilateral torsion of the adnexa: Case report. Open J Clin Med Case Rep. 2023; 2139.
Introduction
Adnexal torsion involves turning the adnexa around its axis [1]. In most cases, both structures (ovary and fallopian tube) rotate around the axis between the infundibulopelvic ligament and the utero-ovarian ligament. Rarely, the ovary can turn itself around the mesoovary, and the fallopian tube around the mesosalpinx. This condition can occur on a pathologically unchanged adnexa, but in 55-75% of cases, we find unilateral changes on the ovary [2]. Torsion accounts for 3% of all gynecological emergencies. It occurs most often in reproductive age, but it can also occur in menopause. It also occurs during pregnancy, 20- 30% of all torsions with 3.5 times more likely in twin pregnancy [3]. It can be partial or complete when necrosis and consequent life-threatening peritonitis occur. It is more common on the right side because the left adnexa is limited by the sigmoid colon [4]. Adnexal masses from 6 to 10 cm have the highest probability of twisting [5]. Patients most often report sharp localized pain, nausea, and vomiting. Febrility speaks in favor of necrosis [2]. The diagnosis is made by clinical examination and an ultrasound exam. CT and MRI are usually not needed [6].
Case Report
The patient was a 32-year-old pregnant woman, who presented to our hospital in the 28th week of spontaneous twin monochorionic-monoamniotic (MCMA) pregnancy with pain in the right hemiabdomen of 24 hours duration. She had one episode of vomiting and absence of stool in the last 72 hours with a loss of appetite. An examination by a surgeon and a urologist was performed, who excluded the indication for urgent surgical treatment, as did the clinical radiologist after two consecutive abdominal ultrasounds. Physical examination revealed mild pain in the left hemiabdomen. At the time of hospitalization, the patient received artificial lung maturation of the fetuses in the form of Dexamethasone shots, fluid replacement, intravenous antibiotics, and antispasmodics. The patient was not given analgesics in order not to mask the clinical picture. She had a history of prior surgery in form of two cesarean sections five and two years prior to this, third pregnancy. The current twin pregnancy was conducted in a spontaneous cycle without ovulation induction, so Ovarian hyperstimulation syndrome (OHSS) was excluded as the cause of torsion.
Laboratory blood examination revealed increased white blood cell count (WBC) of 14.0× 109 /L, neutrophil granulocyte percentage 90%, erythrocyte sedimentation rate (ESR) of 40 mm/h, C Reactive Protein (CRP) 167 mg/L, and normal tumor markers−cancer antigen 125 (CA125) 17 kU/L (ref. 0-35 kU/L), Human Epididymis Protein 4 (HE4) 49.7 pmol/L (ref. before menopause <70 pmol/L) and Risk of Ovarian Malignancy Algorithm (ROMA) index of 7.40% (ref. <7.40%). During hospitalization, the patient developed a subfebrile temperature of 37.5 degrees. After 48 hours thanks to the suggestion of the on-call doctor and the suspected acute abdomen, she was examined immediately in the morning by a gynecologist with the following ultrasound result.
Transabdominal ultrasound identified intrauterine MCMA twin pregnancy. The right ovary measured 14x6.5x9.7 cm with multiple peripherally displaced ovarian follicles resembling a string of pearls (Figures 3 and 4). The left ovary measured 12x7x9.1 cm also with peripheral follicles and stromal oedema (Figure 5). In both ovaries, there was an absent doppler flow. In the region of the right adnexa, there was a collection of free fluid up to 8 mm (Figure 3). Umbilical arterial (UA) Doppler assessment was used in the surveillance of fetal well-being, which showed good fetal condition (Figures 6 and 7).
Adequate artificial lung maturation of the fetuses was conducted, with fibrin degradation products (FDP) came in negative, clear amniotic fluid and normal cardiotocography (CTG) without tachycardia of both fetuses, as well as without ultrasonographycal disturbed circulation. The circumstances of the laboratory findings and ultrasound of the adnexal masses dictated to approach the surgical procedure, as the ‘’Council for Cesarean sections’’ decided to perform a cesarean section and to proceed according to the findings. Transversal laparotomy was performed with the following findings: a large amount of dark, partially coagulated blood was present in the abdominal cavity. The uterus was the size for an eight-month pregnancy. The cesarean section was made. Five minutes after the extraction both of the born twins got an Apgar score of 3. The adnexal finding: a bilaterally necrotic, livid adnexa with a completely altered normal morphological structure was present, with bilateral bleeding of dark deoxygenated blood (Figure 1). The right ovary and right fallopian tube were 20x15 cm in size and had undergone 720 degrees torsion (3 rotations). The left ovary and left fallopian tube were 18x15 cm in size and had undergone 1080 degrees torsion (4 rotations). A decision was made to proceed with a bilateral salpingo-oophorectomy based on the patient’s vital indications. A surgeon was called upon and explored the rest of the abdominal cavity and confirmed that the other abdominal organs were unchanged, except for the omentum which appeared fine-grained, and a biopsy of the omentum with a diameter of 4x3 cm was performed (Figure 2). Both adnexa, biopsy of the omentum, and the placenta were sent for pathohistological (PH) verification.
There were no intraoperative complications. Laboratory blood examination saw a drop in WBC of 6.2×109 /L, neutrophil granulocyte percentage 69%, and CRP 25.5 mg/L. The patient was discharged on the fifth postoperative day with the therapy of oral antibiotics and iron supplementation. She had an uneventful postoperative recovery period. Both neonates remained in the Department of Neonatology for further care and treatment. Thanks to neonatological care and previous artificial maturation of the lungs, both neonates recovered well.
The PH finding revealed that both adnexa were presented with distinctly livid surfaces, and hemorrhagic infarcted appearance. On the cross-sections, both ovaries were enlarged, completely hemorrhagically infarcted, without identifiable vital tissue. Both uterine tubes were macroscopically enlarged, fused with the ovaries, and completely hemorrhagically infarcted. The omentum that was submitted was without focal changes and condensations. Microscopically the analyzed histological sections show a completely hemorrhagic infarcted tissue of the adnexa on both sides, permeated with diffuse hemorrhage, and locally pronounced mixed inflammatory infiltrate. The outlines of adnexal structures and the outlines of cystic spaces with the possible appearance of follicular cysts and focally discrete, vital parts of a hemorrhagic cyst of the corpus luteum, which is also mostly infarcted, can be recognized. No tumor changes were seen in the analyzed material.
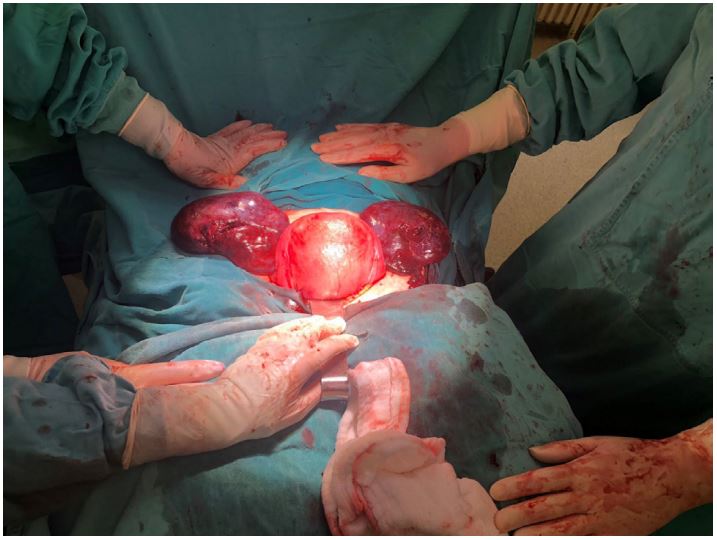
Figure 1: Extremely enlarged, livid and necrotic adnexa
alongside gravid uterus.

Figure 2: Omental flap that appeared fine-grained.
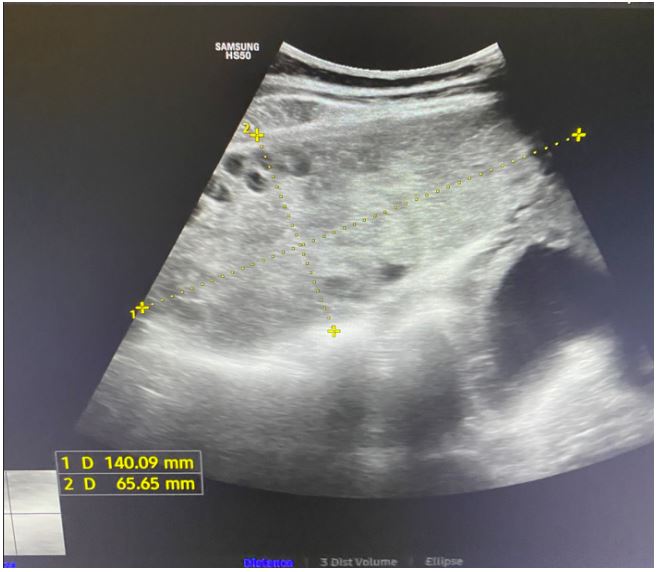
Figure 3: Abdominal ultrasound: The highly enlarged
right ovary with ‘’String of pearl’’ phenomena, and a collection of free fluid on the far right.

Figure 4: Abdominal ultrasound: Right ovary with stromal oedema.
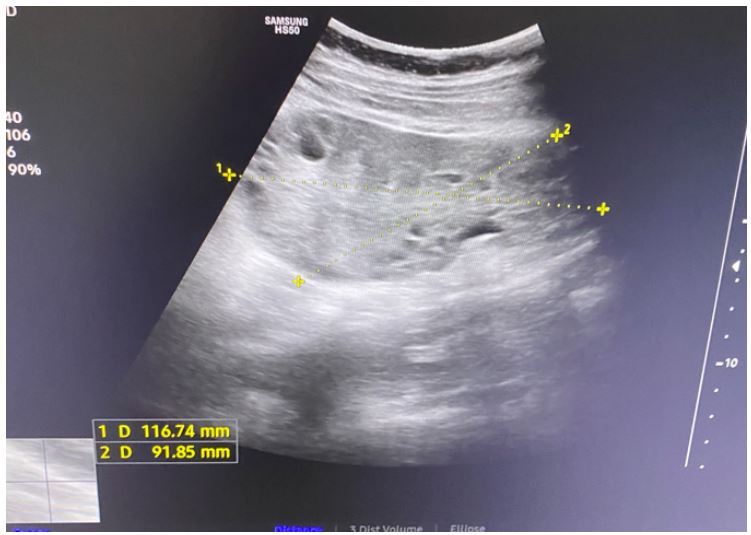
Figure 5: Abdominal ultrasound: Left ovary that shows
enlargement and stromal oedema.
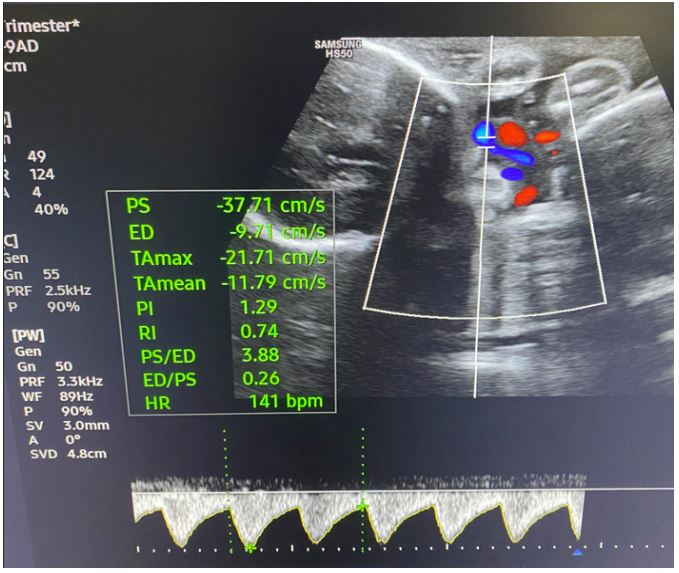
Figure 6: Umbilical arterial (UA) Doppler assessment of
the first twin shows good fetal condition.
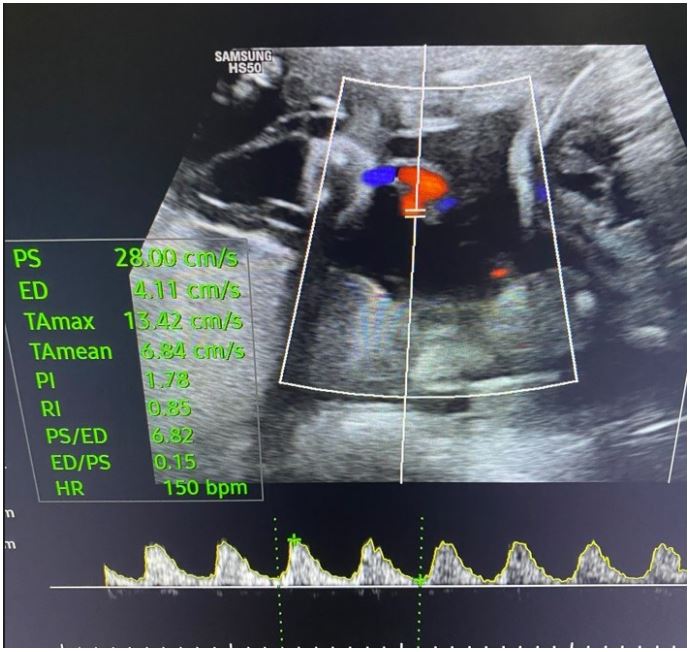
Figure 7: Umbilical arterial (UA) Doppler assessment of the second twin shows good fetal condition.
Discussion
Torsion of the adnexa is one of the most common emergency conditions in gynecology [7] . It occurs most often during the reproductive period. It represents the rotation of the adnexa around its axis and the interruption of blood flow [1]. More mobile adnexal formations have higher rates of torsion [5]. Congenital causes can be excessively long uteroovarian ligaments. Pathologically enlarged ovaries larger than 5 cm rise from the small pelvis and, in the absence of pelvic wall support, become more mobile and susceptible to twisting [5]. The main pathophysiological mechanism is an interruption in blood flow. The ovaries and fallopian tubes resist interruption of blood flow for a long time because they are supplied with double arterial irrigation by the ovarian and uterine arteries. Due to the compression of the venous and arterial blood flow, congestion and edema of the adnexa slowly occur [8]. Necrosis occurs only later when the blood supply is completely cut off. As the edema progresses, congestion, infarction, and necrosis occur [9]. Macroscopically, the adnexa is enlarged, livid, and hemorrhagic. Female patients come to the hospital with sharp pain in the lower abdomen that is getting worse. It is located on the affected side. Nausea and vomiting accompany the clinical picture [10]. If febrility occurs, like in our patient’s case, it indicates tissue necrosis. The diagnosis is established by clinical picture and vaginal or abdominal ultrasound examination. In the differential diagnosis, we can suspect ectopic pregnancy, tuboovarian abscess, hemorrhagic ovarian cyst, endometriosis, diverticulitis, and appendicitis [11] . Ultrasound features a massive edematous adnexa to the midline. Peripherally displaced ovarian follicles – string of pearls. The color doppler presents a whirlpool sign that appears as a twisting of the thickened vascular structures of the enlarged ovary. The uterus is pulled toward the affected ovary with free fluid around it. If there is hemorrhage present the ovarian infarction has likely happened [12]. Torsion is treated with an operative approach. The decision of whether to perform laparoscopy or laparotomy depends on the specific findings. In our case, laparotomy was inevitable due to the pregnancy. Detorsion is always recommended if there is even the slightest chance of saving the ovaries. Only a few minutes after detorsion, circulation is established. Edema, congestion, and lividity of any degree do not necessarily indicate adnexal necrosis. According to the Hytell review, in 2015, 28% of cases of adnexal torsion will re-torsion in the future [13]. That is why various techniques are used to attach the ovaries - oophoropexy to the uterine wall, pelvic wall or lig. rotundum. Another technique involves shortening the uterovarial ligaments.
In pregnancy causes of torsion are mature cystic teratomas and hemorrhagic corpus lutei cysts, which was found in PH results of our patient [14]. Getting a diagnosis during pregnancy, especially in the third trimester, is difficult due to many conditions that cause pain, in particular childbirth, uterine rupture, HELLP syndrome, and placental abruption [15]. Ultrasound diagnosis of the adnexa is less accurate as the pregnancy progresses. The PH findings reveal more frequent benign lesions of the adnexa in pregnant women in contrast to higher neoplastic lesions in non-pregnant women [16].
Conclusion
Adnexal torsion is not uncommon in pregnancy, resulting in 20-25% of all torsions. To the best of our knowledge, this is the first reported case of bilateral torsion of the adnexa in the third trimester of pregnancy. Torsions of the adnexa should be taken into consideration in the differential diagnosis of pain in pregnancy, especially if it is accompanied by nausea, vomiting, and fever.
References
- Sasaki KJ, Miller CE. Adnexal Torsion: Review of the Literature. J Minim Invasive Gynecol 2014; 21: 196-202.
- Nichols DH, Julian PJ. Torsion of the adnexa. Clin Obstet Gynecol. 1985; 28: 375-80.
- Wiser A, Levron J, Kreizer D, Achiron R, Shrim A, Schiff E, et al. Outcome of pregnancies complicated by severe ovarian hyperstimulation syndrome (OHSS): A follow-up beyond the second trimester. Human Reproduction. 2005; 20: 910-4.
- Hasiakos D, Papakonstantinou K, Kontoravdis A, Gogas L, Aravantinos L, Vitoratos N. Adnexal torsion during pregnancy: report of four cases and review of the literature. J Obstet Gynaecol Res. 2008; 34: 683-7
- Houry D, Abbott JT. Ovarian torsion: a fifteen-year review. Ann Emerg Med. 2001; 38: 156-9.
- Jung SE, Lee JM, Rha SE, Byun JY, Jung JI, Hahn ST. CT and MR imaging of ovarian tumors with emphasis on differential diagnosis. Radiographics. 2002; 22: 1305-25.
- Adeyemi-Fowode O, McCracken KA, Todd NJ. Adnexal Torsion. J Pediatr Adolesc Gynecol. 2018; 31: 333-8.
- Garde I, Paredes C, Ventura L, Pascual MA, Ajossa S, Guerriero S, et al. Diagnostic accuracy of ultrasound signs for detecting adnexal torsion: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2022.
- Feng JL, Zheng J, Lei T, Xu YJ, Pang H, Xie HN. Comparison of ovarian torsion between pregnant and non-pregnant women at reproductive ages: Sonographic and pathological findings. Quant Imaging Med Surg. 2020; 10: 137-47.
- Guile SL, Mathai JK. Ovarian Torsion. StatPearls, Treasure Island (FL). StatPearls Publishing. 2022.
- Silber M, Gilboa Y, Perlman S, Krispin E, Sukenik S, Shochat T, et al. Accurate Diagnosis of Adnexal Torsion-Not Only for Expert Sonographers: A Retrospective Cohort Analysis. J Ultrasound Med. 2021; 41: 725-32.
- Moro F, Bolomini G, Sibal M, Vijayaraghavan SB, Venkatesh P, Nardelli F, et al. Imaging in gynecological disease (20): clinical and ultrasound characteristics of adnexal torsion. Ultrasound Obstet Gynecol. 2020; 56: 934-43.
- Hyttel TEW, Bak GS, Larsen SB, Løkkegaard ECL. Re-torsion of the ovaries. Acta Obstet Gynecol Scand. 2014; 94: 236-44.
- Conte AB, Nyingone S, Jayi S, Diagne BJ, Alaoui FZF, Chaara H, et al. Management of adnexal masses’ torsion during pregnancy. Pan Afr Med J. 2020; 37: 17.
- Djavadian D, Braendle W, Jaenicke F. Laparoscopic oophoropexy for the treatment of recurrent torsion of the adnexa in pregnancy: case report and review. Fertil Steril. 2004; 82: 933-6.
- Didar H, Najafiarab H, Keyvanfar A, Hajikhani B, Ghotbi E, Kazemi SN. Adnexal torsion in pregnancy: A systematic review of case reports and case series. Am J Emerg Med. 2022; 65: 43-52.
