
Open Access, Volume 9
Perinephric and psoas abscesses leading to empyema: An unusual tuberculosis presentation
Justin Luke D Yap*; Justin Nico L Aspirin
Department of Radiology, Northern Mindanao Medical Center, Philippines.
Justin Luke D Yap
Department of Radiology, Northern Mindanao Medical Center, Philippines.
Email: justinyap21@gmail.com
Received : Sep 11, 2023,
Accepted : Oct 17, 2023
Published : Oct 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Tuberculous psoas abscess usually results from tuberculous spondylitis but may also develop from direct spread or via hematogenous route [1]. Our case involves direct spread from an adjacent perinephric abscess with associated thoracic extension from suspected direct erosion or a diaphragmatic defect. We present a case of pleural empyema arising from abdominal tuberculous abscesses. This is an 11-year-old male who initially presented with a three-week history of cough, intermittent fever, and dyspnea. Congenital diaphragmatic hernia was first suspected at the emergency department when an opacified left hemithorax with cystic lucencies was noted. Further imaging of the chest and upper abdomen was done in our institution revealing large left perinephric and psoas abscesses with intra-thoracic extension resulting in empyema thoracis and necessitans. Culture of the abscess fluid yielded no growth but GenExpert tested positive for M. tuberculosis. Tuberculosis remains a major illness in developing countries and has a multitude of infection sites and clinical presentation. Our case presented as an ascending thoracic extension of a perinephric and psoas abscess, likely from a diaphragmatic defect. The absence of spinal involvement proves its renal origin. The importance of CT scan is highlighted in medically-confounding cases such as this one.
Keywords: Case; Cough; Fever; Abdomen; Tuberculosis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Justin luke DY (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Yap JLD, Aspirin JNL. Perinephric and psoas abscesses leading to empyema: An unusual tuberculosis presentation. Open J Clin Med Case Rep. 2023; 2138.
Introduction
A tuberculous psoas abscess usually results from tuberculous spondylitis but may develop without any demonstrable spinal involvement. In patients with no evidence of spondylitis, this can be attributed to direct spread from an adjacent organ or via a hematogenous route [8]. Thoracic extension of abdominal infections is rare and mechanisms are poorly understood, but several routes have been proposed such as direct erosion or through a congenital diaphragmatic defect [5]. We present a case of pleural empyema secondary to multiple abdominal tuberculous abscesses arising from the left perinephric and psoas regions, highly likely through direct spread.
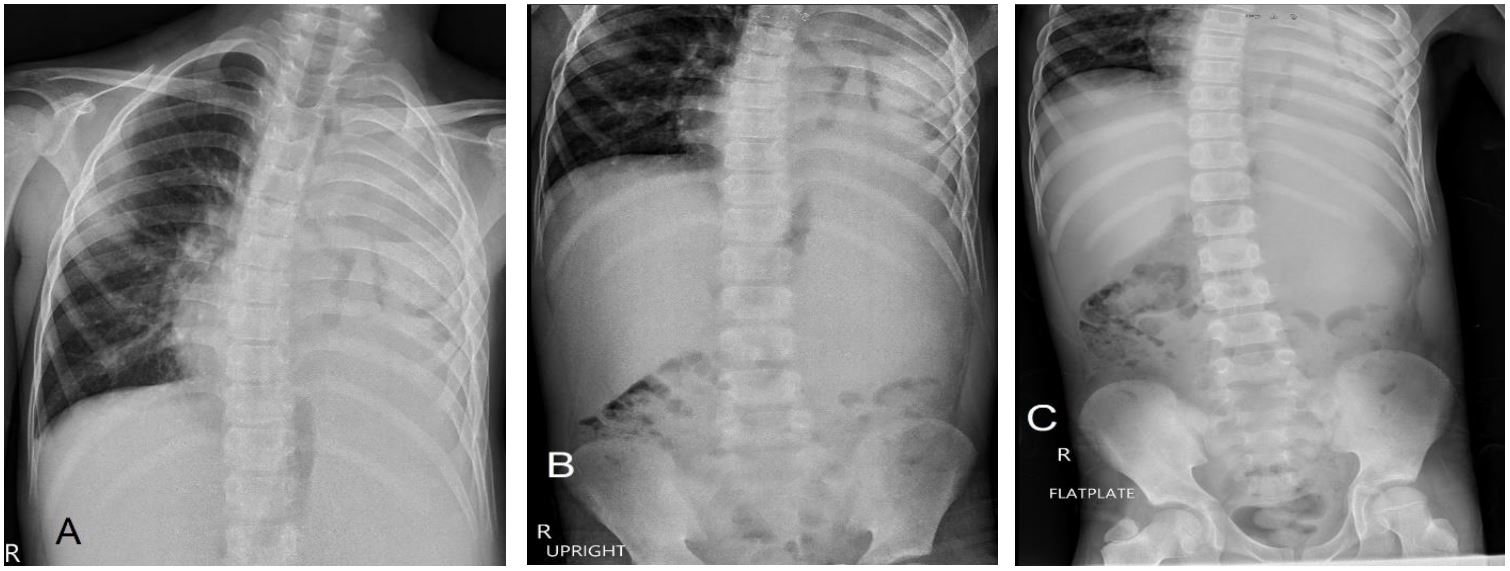
Figure 1: Radiographs on admission. (A) Chest AP view showing near-total opacification of the left hemithorax with trace
lucencies and (B-C) Abdominal images showing soft tissue fullness in the left hemiabdomen which appears to extend into the
ipsilateral hemithorax with inferomedial displacement of the gas-filled bowel loops.
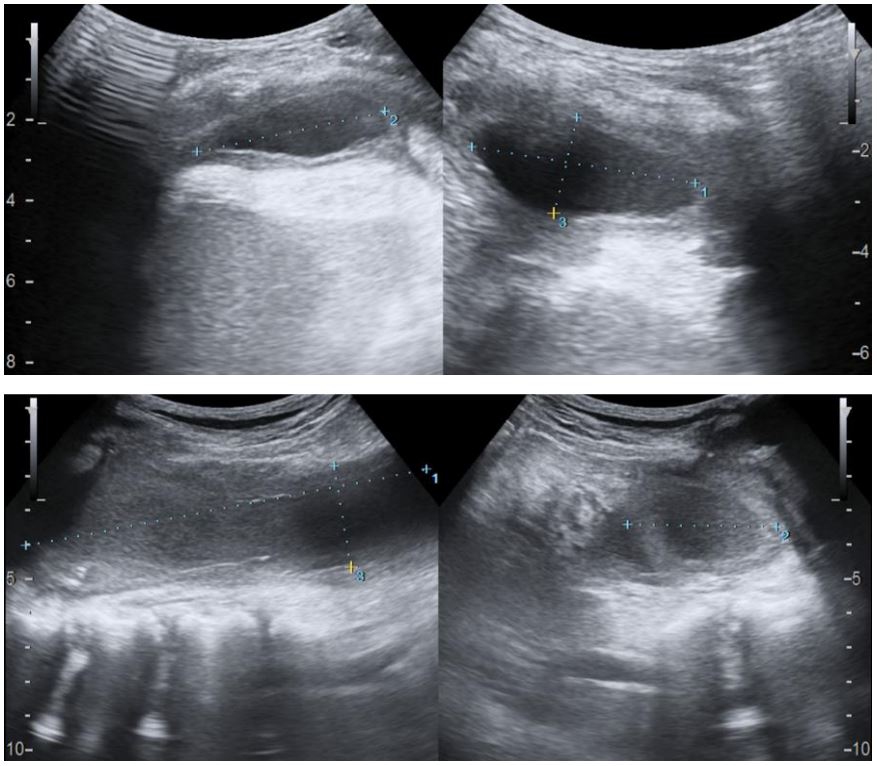
Figure 2: Chest ultrasound showing left empyema (A) and left
psoas abscesses (B) with margins demarcated by calipers.
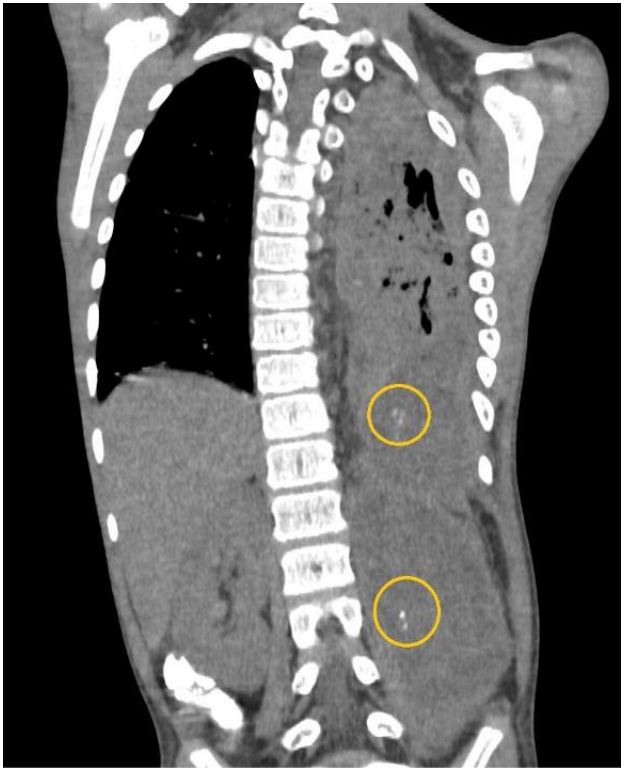
Figure 3: Plain CT coronal image highlighting the calcifications (yellow circles) within the abscesses.by calipers.
Case Presentation
We present a case of P.M. An 11-year-old who initially presented with a three-week history of cough, Intermittent fever, and dyspnea. The initial diagnosis of left congenital diaphragmatic hernia was suspected from the chest radiograph and ultrasound in another institution as an opacified left hemithorax and bowel loops within the left thoracic cavity were found, respectively. The patient was subsequently referred to our institution where chest radiograph (Figure 1), chest ultrasound (Figure 2) and contrast-enhanced CT scan of the chest and upper abdomen (Figure 3-7) were done showing left perinephric and left psoas abscesses with intra-thoracic extension, probably through a left diaphragmatic defect, forming empyema thoracis and empyema necessitans. Culture of abscess fluid yielded no bacterial growth but GenExpert test was positive for M. tuberculosis.
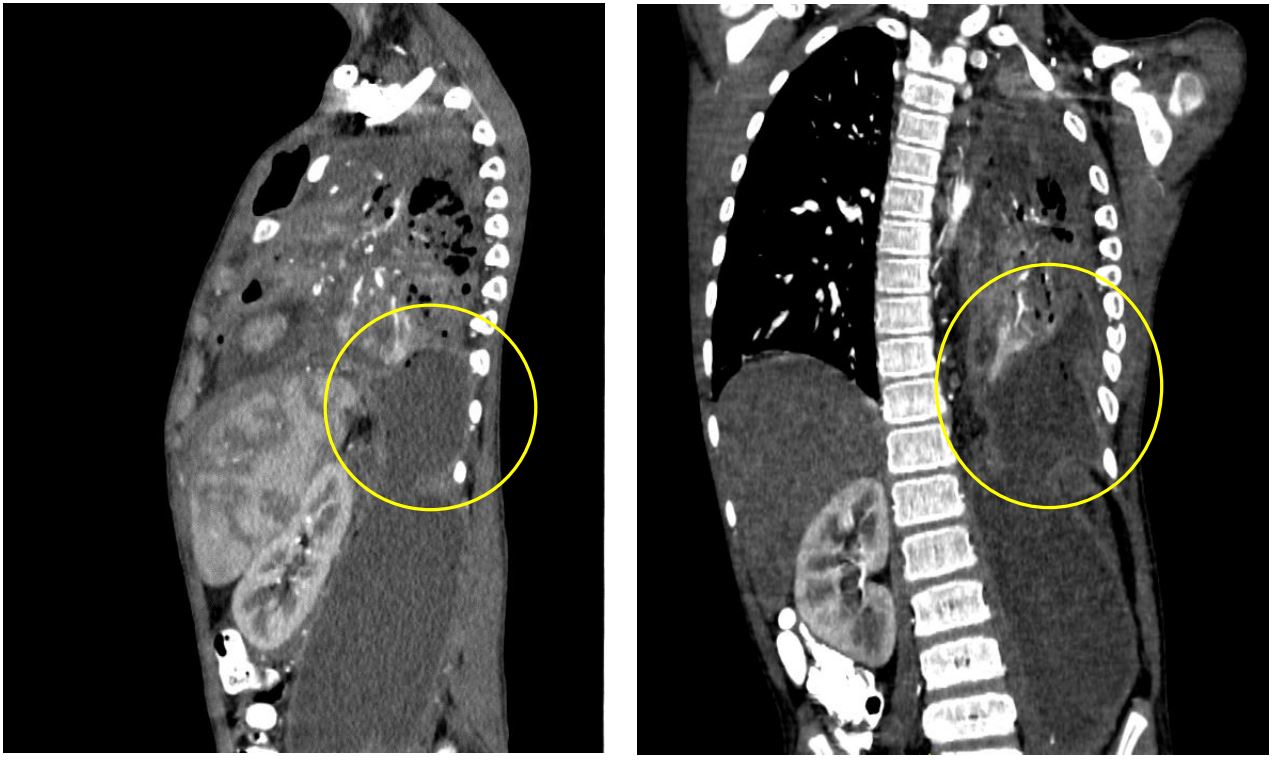
Figure 4: Contrast-enhanced CT showing extent of the intra-thoracic involvement of the abdominal abscesses (yellow circles).
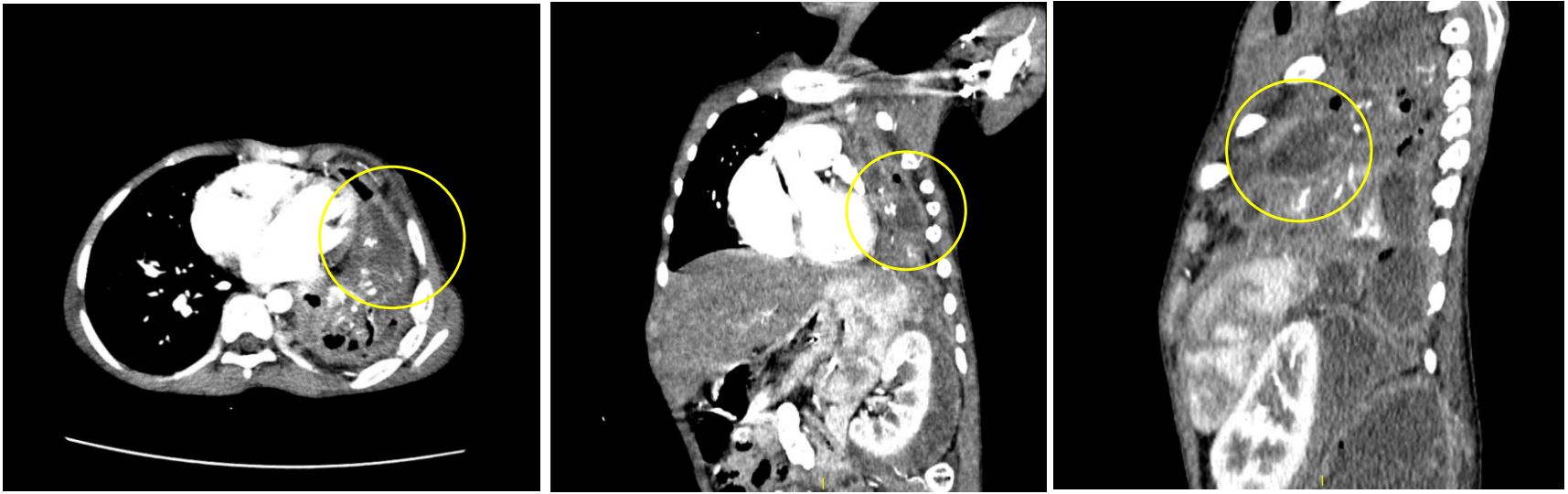
Figure 5: Contrast-enhanced CT showing axial (A), Coronal (B), And sagittal (C) Views depicting a hypodense collection
within a thick-enhancing pleura in the left lower hemithorax (yellow circle), Compatible with empyema thoracis.
Discussion
In developing countries, Tuberculosis (TB) is common and remains a scourge which may involve any system, including the respiratory, gastrointestinal, cardiac, central nervous, musculoskeletal and genitourinary systems. Out of all the systems, pulmonary tuberculosis remains the most common while the genitourinary system remains to be the most common extrapulmonary site [2].
Iliopsoas abscess is a rare clinical entity and is described as a collection of pus in the iliopsoas compartment. It can be classified as either a primary or secondary process. Primary psoas abscess occurs most commonly in patients with history of diabetes, injection drug use, alcoholism, acquired immune-deficiency syndrome (AIDS), renal failure, hematological malignancy, immunosuppression or malnutrition [1-3]. Secondary psoas abscess results from spread from a primary infection with a skeletal origin being the most common [1,3,8]. Direct spread from tuberculous spondylitis have been observed presenting as calcifications within the abscess being virtually diagnostic of its tuberculous etiology [2].
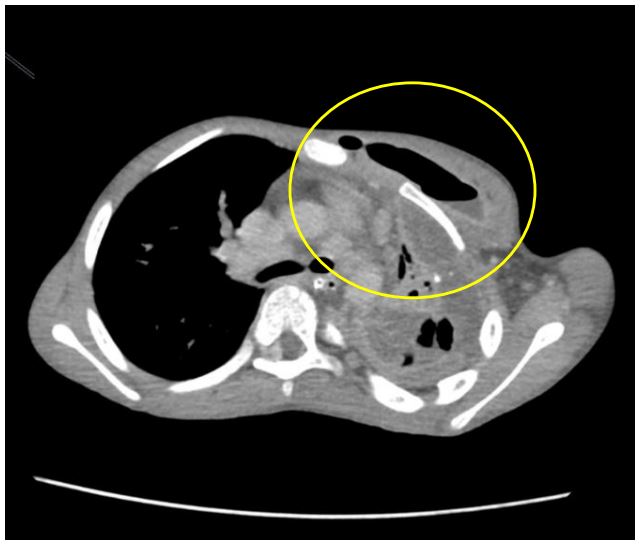
Figure 6: Contrast-enhanced CT scan (axial view)
showing rim-enhancing hypodense collection with
air-fluid layering in the left anterior chest wall (yellow
circle), suggestive of empyema necessitans
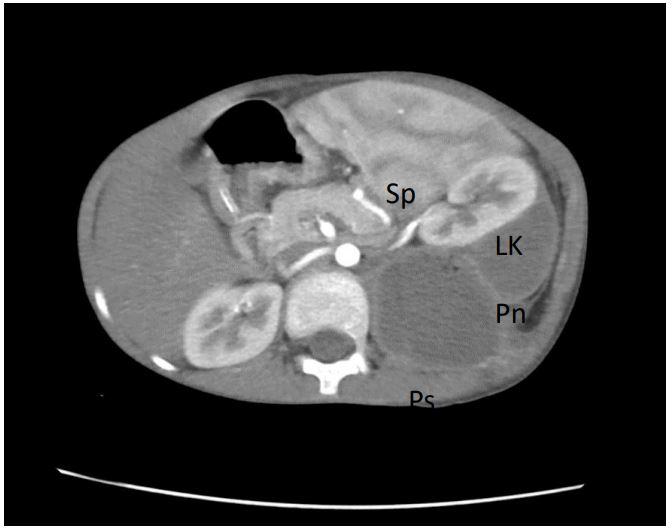
Figure 7: Contrast-enhanced CT showing close relationship between perinephric (Pn) and psoas (Ps)
abscesses and anterior displacement of the left kidney
(LK) and spleen (Sp).
A renal origin, due to its close proximity to the psoas muscle, can likewise cause direct spread of renal or perirenal infections through the perirenal space although less likely and uncommon (Figure 7) [3,4]. The abundant blood supply of the muscle is believed to predispose it to hematogenous spread from occult sites of infection [3]. With no skeletal involvement observed in our case, a renal origin through a co-existing perinephric abscess is believed to be the primary site of infection.
Any infectious process that spreads to the psoas muscle can progress into the posterior mediastinum and cause pleural complications [5-9]. Several routes and mechanisms have been described such as direct erosion through the diaphragm, trans-diaphragmatic migration of infected abdominal fluid, or as insinuated this case, a probable congenital diaphragmatic defect which is the proposed route for ascending retroperitoneal infection into the thoracic cavity causing empyema thoracis and subsequently empyema necessitans (Figures 5,6) [5-7]. Empyema thoracis is defined by the presence of frank pus in the pleural space and commonly from extension of a pulmonary infection. Moreover, Pleural complications secondary to an ascending abdominal infection is relatively rare [6].
CT scan remains the mainstay for investigating possible abdominal or genitourinary tuberculosis and its complications as it can also outline the location and possible extension of a psoas abscess. It can also identify the predisposing pathology as perinephric abscess or a bowel inflammatory lesion. Non-contrast CT could also depict calcifications within the abscess which, as discussed above, is virtually diagnostic for tuberculosis. Contrast-enhanced CT optimizes visualization of the abscess extensions and margins (1).
Conclusion
In conclusion, tuberculosis remains a major illness especially in developing countries and has a wide and varied presentation. Here we are presented with an unusual case which was initially assessed as congenital diaphragmatic hernia but with subsequent imaging proved to be an ascending thoracic extension of a perinephric and psoas abscess, likely from a diaphragmatic defect. The psoas abscess presented in this case is, in itself, unusual because no spinal involvement was noted, hence a renal source of infection was more plausible. This case also highlights the importance of CT scan as an invaluable tool in the radiologic armamentarium for the prompt detection and diagnosis of medically-confounding cases.
References
- Ali HM, Shoshan HMA. Multifocal primary musculoskeletal tuberculosis in nonimmunocompromised patient from nonendemic area. BJR Case Rep. 2020; 6: 29 20190077.
- Burrill J, Williams C, Bain G, Conder G, Hine AL, Misra RR. Tuberculosis: A Radiologic Review. Radiographics. 2007; 27(5): 1255-1273.
- Kurian E, Anand R, Bos R, Joseph J. A case report of perinephric abscess extending as psoas abscess. Int J Adv Med 2021; 8: 1743-5
- Merchant S, Bharati A, Merchant N. Tuberculosis of the genitourinary system-Urinary tract tuberculosis: Renal tuberculosisPart I. Indian J Radiol Imaging. 2013; 23: 46-63.
- Sharma, R. et. al. Routes of Transdiaphragmatic Migration from the Abdomen to the Chest. Radiographics Vol. 2020; 40: 5.
- Tamburrini S, Lugarà M, Saturnino PP, Ferrandino G, Quassone P, Leboffe S, Sarti G, Rocco C, Panico C, Raffaele F, Cesarano T, Iannuzzi M, Cagini L, Marano I. Pleural empyema secondary to nephropleural fistula in complicated pyonephrosis. Radiol Case Rep. 2021; 16(9): 2714-2718.
- Tan PSC, Badiei A, Fitzgerald DB, Kuok YJ, Lee YCG. Pleural empyema in a patient with a perinephric abscess and diaphragmatic defect. Respirol Case Rep. 2019; 29; 7: e00400.
- Vasigh M, Karoobi M, Montazeri M, Moradi G, Asefi H, Gilani A, Meshkati Yazd SM. Isolated psoas abscess caused by Mycobacterium tuberculosis: A rare case report. Clin Case Rep. 2022; 27; 10(5): e05823. doi: 10.1002/ccr3.5823. PMID: 35664522; PMCID: PMC9136494.
- Veerappan I, Shanmugam A, Kumar S, Velayutham P. Bilateral psoas and bilateral perinephric abscesses complicating acute pyelonephritis in pregnancy. Indian J Nephrol. 2013; 23: 59-62.
- Wei HL, Wang L, DU XG, Wu Y, Li H, Cai Y, Song XH, Li CX, Dong LP, Liu ZF, Zhao X, Dong JW. Renal tuberculosis and iliopsoas abscess: Two case reports. Exp Ther Med. 2014; 7: 1718-1720.
