
Open Access, Volume 9
Malignant phyllodes tumor with lymphatic metastatic dissemination following surgery and radiotherapy
Wolfsohn Jesse1; Safadi Ali2; Yagudaev Eva3; Safadi Wajdi4*
1Ben-Gurion University of the Negev Faculty of Health Sciences, Israel.
2University of Campania Luigi Vanvitelli School of Medicine and Surgery, Italy.
3Ben-Gurion University of the Negev Faculty of Health Sciences, Medical School for International Health, Israel.
4Clalit Health Services, Department of Surgery Israel.
Safadi Wajdi
Clalit Health Services, Department of Surgery, Israel.
Email: golancare@hotmail.com
Received : Sep 09, 2023,
Accepted : Oct 13, 2023
Published : Oct 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Phyllodes tumors (PTs) are fibroepithelial neoplasms, and constitute less than 1% of all female breast tumors [1]. Malignancy is observed in 10% of PTs, with metastases usually spreading hematogenously. Although up to 15% of hematogenously metastasized PTs include palpable axillary lymph nodes, less than 1% of these cases have been found to have lymph nodes that are positive for malignancy [1]. We present a patient in her forties with a malignant PT that metastasized distantly to the axillary, mediastenal, and retroperitoneal lymph nodes, with liver metastasis, despite surgical excision and radiotherapy. Unfortunately, the patient succumbed to the disseminated PT. Despite the rarity of this condition, we recommend that breast surgeons and other members of the treating team for PTs should be highly aware of lymphatic dissemination so that the health outcomes of patients are optimized.
Keywords: Phyllodes tumors; Lymph nodes; Radiotherapy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Wajdi S (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Jesse W, Ali S, Eva Y, Wajdi S. Malignant phyllodes tumor with lymphatic metastatic dissemination following surgery and radiotherapy. Open J Clin Med Case Rep. 2023; 2136.
Background
Phyllodes tumors (PTs) are rare fibroepithelial breast tumors, which account for less than 1% of all breast neoplasms, and typically develop in women aged 40-50 Years [2,3]. This is about 15-20 Years later than the typical presentation of breast fibroadenomas, although it can still be difficult to differentiate these two entities [2]. Whereas fibroadenomas grow up to 2-3 cm, PTs grow continuously, and have been found with diameters of 40 cm [4]. Moreover, the term “Phyllodes” originates from the Greek word for “leaf”. This resembles its histologic appearance, and is notable for a biphasic appearance with both stromal and epithelial components [1]. The World Health Organization classifies PTs as either benign, borderline, or malignant, based on the degree of “nuclear atypia, sromal cellularity, mitotic activity, tumor margin appearance, and stromal overgrowth” [1]. As the stromal component expands, the epithelial component, which is almost always benign, appears to diminish, such that the “leaf-like” appearance may be lost [5].
Furthermore, malignancy is observed in 10% of PTs with metastases usually spreading hematogenously, with the most common sites being the lungs, bones, and brain. Although up to 15% of hematogenously metastasized PTs include palpable axillary lymph nodes, less than 1% of these cases have been found to have lymph nodes that are positive for malignancy [4]. This is because lymphadenopathy usually corresponds to reactive hyperplasia from tumor necrosis or infection. Therefore, routine axillary lymph node dissection is not recommended, and should only be performed on patients with evidence of PT metastasis through the lymph node [6].
Likewise, the local recurrence rate of PTs is 20% on average, with a distant metastasis rate of 3.5%. However, malignant PTs are notable for their local recurrence rate of 40%, and distant metastasis rate of 30% [7].
Treatment for PTs typically involves surgical removal of the tumor, and in the case of malignant tumors, additional treatment such as radiotherapy, which prevents local recurrence, may be necessary [2- 8]. The prognosis for PTs is generally good with an 87% 10-year survival rate, especialy for benign tumors. However, the outcome can depend on the specific type and stage of the tumor [2-8].
In addition, there is some controversy surrounding the necessary width of surgical margins. Although 1 cm margins are traditionally preferred, it is difficult to achieve this width, such that the patient may require a re-excision surgery, which poses the risk of additional surgery-related complications [9]. Likewise, while 1 cm surgical margins decrease local recurrences of PTs, the width of the surgical margins have no significant benefit in reducing the occurrences of distant metastases [9-10]. This may result from the highly aggressive nature of malignant PTS, such that distant metastases may have already developed by the time of surgical excision [10].
Case Presentation
A woman in her forties was found to have a mass in the outer quadrant of the right breast, which was measured at 4 cm on ultrasound. Subsequently, a core needle biopsy was performed, which diagnosed the mass as a fibroadenoma. However, due to the large size of the mass, a lumpectomy was performed, which diagnosed the mass as a high-grade malignant PT. Since the margins were still involved, a re-lumpectomy was performed with 1 cm free margins. Several months later, an enlarged axillary lymph node was diagnosed via ultrasound. Indeed, the corresponding lymph node biopsy confirmed that the PT had spread into the axillary lymph node. After investigation with PET-CT that showed single lymph node involvement in the right axilla, bilateral mastectomy with right axillary lymph node dissection was performed. Although bilateral mastectomy was not indicated, this procedure was performed due to the patient’s preferences. Afterwards, both breasts were found to be clear, but 1/16 lymph nodes were positive for malignancy. The patient was then started on radiotherapy. However, shortly after, an additional axillary mass was identified. In fact, chest and abdominal CT demonstrated that there were distant metastases in the axillary, mediastinal, and retroperitoneal lymph nodes, and the liver. The patient was then started on chemotherapy. However, A follow-up CT showed that the metastases had increased in size.
Investigations
Initially, 4 cm right-sided breast mass was identified on ultrasound (Figure 1). From there, a core needle biopsy was performed, which demonstrated a fibroadenoma. However, the histology from the ensuing lumpectomy demonstrated the presence of a malignant PT. After several courses of radiotherapy, the discovery of the right-sided axillary lymph node necessitated PET-CT, which showed high intake of FDG (Figure 2). The corresponding core needle biopsy confirmed that it contained metastasized PT. After performing bilateral mastectomy with right axillary lymph node dissection, the histology proved that the breasts were clear, but that 1/16 lymph nodes contained PT. Significantly, the occurrence of an additional axillary mass a couple months later prompted an abdominal and chest CT. This demonstrated metastases in the axillary, mediastinal, and retroperitoneal lymph nodes, with liver metastasis (Figures 3 and 4). No further biopsies were performed, and follow-up abdominal and chest CT demonstrated that the metastases had increased in size (Figures 5 and 6).
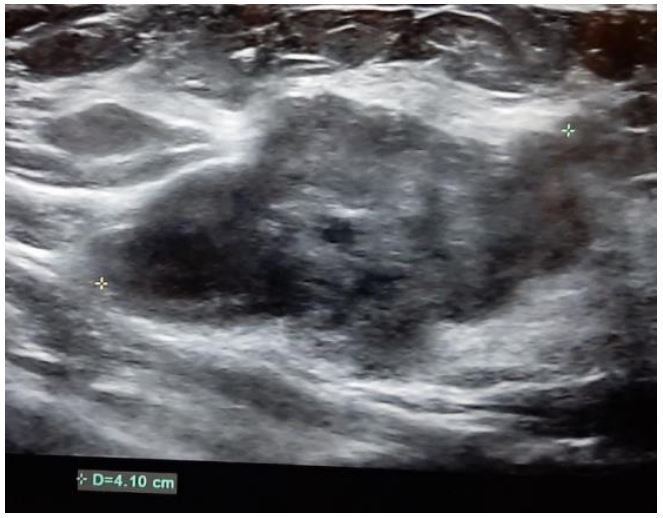
Figure 1: Ultrasound demonstrating a 4 cm right breast
mass with irregular borders.
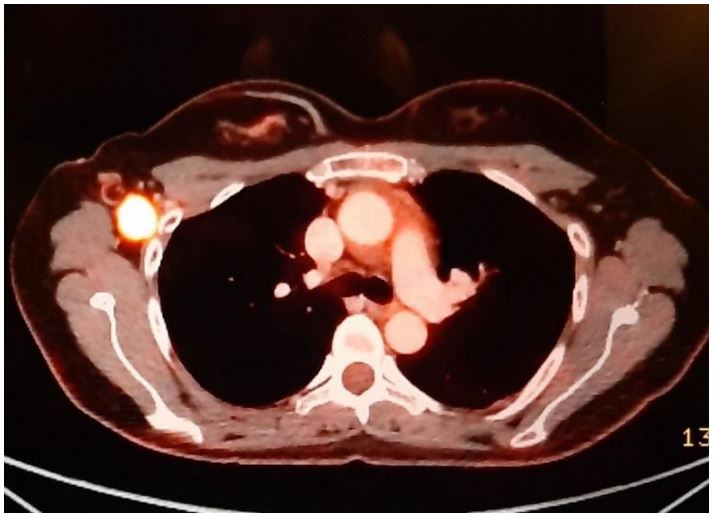
Figure 2: PET-CT demonstrating high intake of FDG in
the right axillary lymph node.
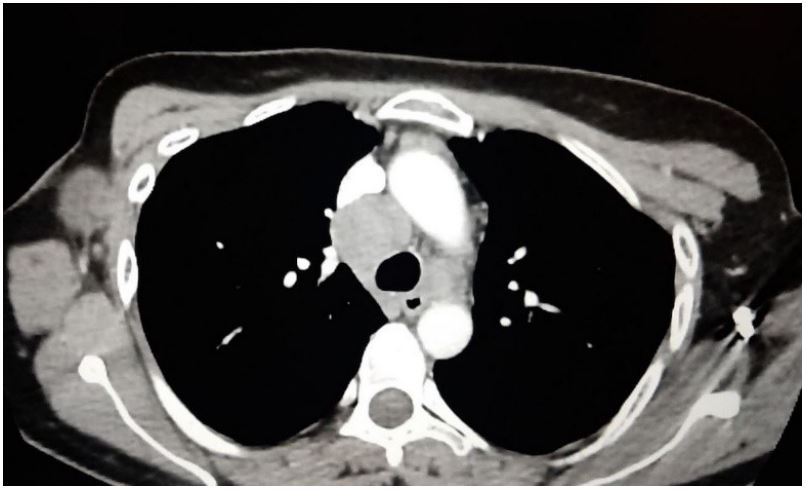
Figure 3: Chest CT demonstrating pathologic axillary
and mediastinal lymph nodes.
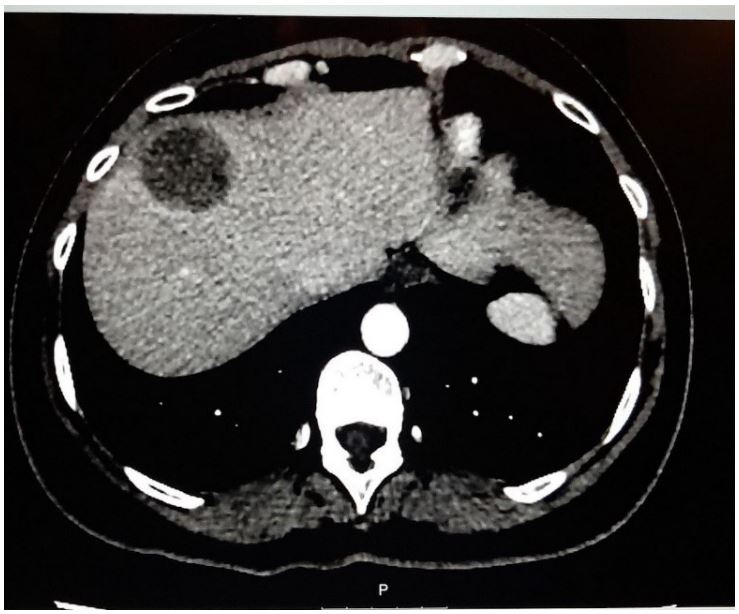
Figure 4: CT demonstrating liver metastasis.
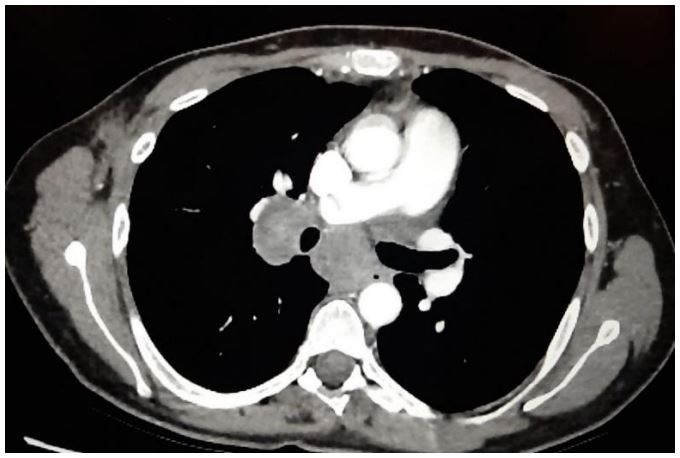
Figure 5: CT demonstrating enlargement of axillary and
mediastinal lymph nodes.
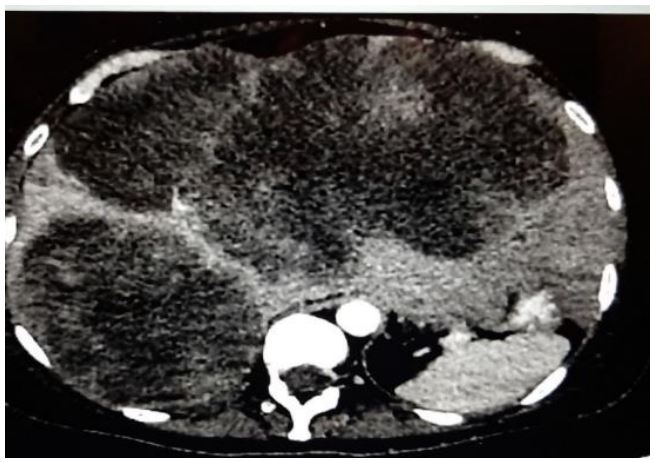
Figure 6: CT demonstrating enlargement of liver metastasis.
Differential diagnosis
Although the patient was initially believed to have a fibroadenoma based on the findings from the core needle biopsy, she was unfortunately found to have a malignant PT in excisional biopsy. Both these lesions originate from intralobular fibrous tissue, and have similar histology initially. However, as the pathologies progress, the histologies differ [11]. Regarding immunohistochemistry, phyllodes tumors have increased staining with proliferating cell nuclear antigen (PCNA), Ki-67, and androgen receptors, which act as markers of proliferation. In addition, PCNA is mainly involved with DNA replication, while androgen receptor staining is mainly involved with stromal proliferation [12-13]. Also, PTs tend to break through and project out from their surrounding capsule. All of these factors are important to be aware of, because it is clinically difficult to distinguish PTs from fibroadenomas. The appropriate diagnosis must be made so that the patient receives optimal medical treatment [11].
Treatment
After a robust treatment course involving lumpectomy, bilateral mastectomy and right-sided axillary lymph node dissection, the patient received radiotherapy to the chest wall and right axilla. However due to recurrence in the axillary lymph nodes and distant metastasis, the patient was started on Adriamycin and Ifosfamide, without any response. After these metastases were found to increase in size, even with chemotherapy, the patient was placed into palliative care.
Outcome
As expected with palliative care, the patient unfortunately succumbed to her advanced medical condition, and expired shortly after being started on chemotherapy.
Discussion
PT is a rare fibroepithelial breast tumor that typically manifests in women between 40-50 years of age as a painless, multinodular breast mass. Unlike fibroadenomas, PTs tend to increase in size more rapidly over time. On breast ultrasound, PTs appear as a hypoechoic solid mass containing cysts; on mammography, they appear as a hyperdense mass. Biopsy is required for diagnostic confirmation. Histological findings of stromal cellularity and leaf-like architecture distinguish PTs from fibroadenomas. Significantly, PTs are categorized as benign, Borderline, and malignant according to the following features: Border infiltration, mitotic activity, stromal atypia, and hypercellularity. Typically, malignant or borderline PTs metastasize hematogenously. In addition, surgical excision is recommended for nonmetastatic disease. Although metastatic PTs carry a poor prognosis, management (e.g., palliative therapy, chemotherapy) should be tailored to the individual patient. Unfortunately, PTs have a high rate of recurrence after surgical excision, proving to be a challenge to treat [14-19]. Our case is notable, because it is a rare case of a malignant PT demonstrating lymphatic metastatic dissemination following radiotherapy, with metastases to the axillary, mediastinal, and retroperitoneal lymph nodes, with liver metastasis.
Since PTs are a rare pathology, there is limited knowledge on this topic. Therefore, further research must be conducted to strengthen the knowledge base on PTs, so that we can advance medical interventions, optimize adjuvant therapies for this pathology, and improve patient care by detecting PTs before lymphatic metastatic dissemination occurs.
Learning points
● Be aware of the possibility of lymphatic dissemination in malignant phyllodes tumors and monitor for lymphatic metastasis post-treatment.
● Sometimes, it is difficult to differentiate phyllodes tumors from fibroadenomas by core needle biopsy
● Large and quickly growing masses in the breast must be excised for pathologic evaluation.
References
- Hayati F, Lian HH, Azizan N, Ali AA, Abidin ZA, Suhaili MA. Approaches to phyllodes tumour of the breast, A review article. International Surgery Journal. 2017; 4(3): 841.
- Limaiem F, Kashyap S. Phyllodes tumor of the breast-statpearls-NCBI bookshelf [Internet]. StatPearls. National Library of Medicine ; 2022 [cited 2023Feb26]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK541138/
- Shafi AA, AlHarthi B, Riaz MM, AlBagir A. Gaint phyllodes tumour with axillary & interpectoral lymph node metastasis; a rare presentation. International Journal of Surgery Case Reports. 2020; 66: 350-5.
- Mishra SP, Tiwary SK, Mishra M, Khanna AK. Phyllodes tumor of breast: A review article. ISRN Surgery. 2013; 2013: 1-10.
- Hauser H, Hammer R, Schöllnast H, Humer-Fuchs U, Kriegl D, Fuchsjäger M, et al. Malignant phyllodes tumor of the breast with axillary lymph node metastasis. Case report and review of the literature. European Surgery. 2022; 54(3): 156-62.
- Koh VC, Thike AA, Tan PH. Distant metastases in phyllodes tumours of the breast: An overview. Applied Cancer Research. 2017; 37(1).
- Belkacémi Y, Bousquet G, Marsiglia H, Ray-Coquard I, Magné N, Malard Y, et al. Phyllodes tumor of the breast. International Journal of Radiation Oncology *Biology* Physics. 2008; 70(2): 492-500.
- Lenhard MS, Kahlert S, Himsl I, Ditsch N, Untch M, Bauerfeind I. Phyllodes tumour of the breast: Clinical follow-up of 33 cases of this rare disease. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2008; 138(2): 217-21.
- Tremblay-LeMay R, Hogue J-C, Provencher L, Poirier B, Poirier É, Laberge S, et al. How wide should margins be for phyllodes tumors of the breast? The Breast Journal. 2016; 23(3): 315-22.
- Toussaint A, Piaget-Rossel R, Stormacq C, Mathevet P, Lepigeon K, Taffé P. Width of margins in phyllodes tumors of the breast: The controversy drags on?-a systematic review and meta-analysis. Breast Cancer Research and Treatment. 2020; 185(1): 21-37.
- Oprić S, Oprić D, Gugić D, Granić M. Phyllodes tumors and fibroadenoma common beginning and different ending. Collegium Antropologicum. 2012; 36(1): 235-41.
- Juríková M, Danihel Ľ, Polák Š, Varga I. KI67, PCNA, and Mcm proteins: Markers of proliferation in the diagnosis of breast cancer. Acta Histochemica. 2016; 118(5): 544-52.
- Kim Y-H, Kim G-E, Lee JS, Lee JH, Nam JH, Choi C, et al. Hormone receptors expression in phyllodes tumors of the breast. Analytical and quantitative cytology and histology. 2012; 34(1): 41-8.
- Fernández-Ferreira R, Arroyave-Ramírez A, Motola-Kuba D, Alvarado-Luna G, Mackinney-Novelo I, Segura-Rivera R. Giant benign mammary phyllodes tumor: Report of a case and review of the literature. Case Reports in Oncology. 2021; 14(1): 123-33.
- Kalambo M, Adrada BE, Adeyefa MM, Krishnamurthy S, Hess K, Carkaci S, et al. Phyllodes tumor of the breast: Ultrasoundpathology correlation. American Journal of Roentgenology. 2018; 210(4).
- Plaza MJ, Swintelski C, Yaziji H, Torres-Salichs M, Esserman LE. Phyllodes tumor: Review of Key Imaging Characteristics. Breast Disease. 2015; 35(2): 79-86.
- Practice bulletin no. 164. Obstetrics & Gynecology. 2016; 127(6).
- Simpson A, Li P, Dietz J. Diagnosis and management of phyllodes tumors of the breast. Annals of Breast Surgery. 2021; 5: 8.
- Tan BY, Acs G, Apple SK, Badve S, Bleiweiss IJ, Brogi E, et al. Phyllodes tumours of the breast: A consensus review. Histopathology. 2015; 68(1): 5-2.
